Devices And Systems For Accessing And Repairing A Heart Valve
Van Hoven; Dylan T. ; et al.
U.S. patent application number 16/882038 was filed with the patent office on 2020-11-26 for devices and systems for accessing and repairing a heart valve. This patent application is currently assigned to EVALVE, INC.. The applicant listed for this patent is EVALVE, INC.. Invention is credited to Dylan T. Van Hoven, Michael F. Wei.
| Application Number | 20200367871 16/882038 |
| Document ID | / |
| Family ID | 1000004883516 |
| Filed Date | 2020-11-26 |











View All Diagrams
| United States Patent Application | 20200367871 |
| Kind Code | A1 |
| Van Hoven; Dylan T. ; et al. | November 26, 2020 |
DEVICES AND SYSTEMS FOR ACCESSING AND REPAIRING A HEART VALVE
Abstract
Medical delivery system for accessing a tricuspid valve via an inferior vena cava, including an outer guide catheter, an inner guide catheter and an interventional catheter. The first deflection portion of the outer guide catheter is steerable to define a first outer-guide-catheter curve and the second deflection portion of the outer guide catheter is steerable to define a second outer-guide-catheter curve and the first deflection portion of the inner guide catheter is steerable to define a first inner-guide-catheter curve.
| Inventors: | Van Hoven; Dylan T.; (San Carlos, CA) ; Wei; Michael F.; (Redwood City, CA) | ||||||||||
| Applicant: |
|
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Assignee: | EVALVE, INC. Santa Clara CA |
||||||||||
| Family ID: | 1000004883516 | ||||||||||
| Appl. No.: | 16/882038 | ||||||||||
| Filed: | May 22, 2020 |
Related U.S. Patent Documents
| Application Number | Filing Date | Patent Number | ||
|---|---|---|---|---|
| 63007854 | Apr 9, 2020 | |||
| 62851573 | May 22, 2019 | |||
| Current U.S. Class: | 1/1 |
| Current CPC Class: | A61M 2205/0266 20130101; A61F 2/2466 20130101; A61B 17/00234 20130101; A61B 2017/00336 20130101; A61F 2/246 20130101; A61B 2017/00243 20130101; A61B 2017/00323 20130101 |
| International Class: | A61B 17/00 20060101 A61B017/00; A61F 2/24 20060101 A61F002/24 |
Claims
1) A medical delivery system for accessing a tricuspid valve via an inferior vena cava, comprising an outer guide catheter having a proximal end portion, a first deflection portion, a second deflection portion, and a distal end portion each aligned in series along a length of the outer guide catheter, and having a steering assembly comprising a first steering mechanism and a second steering mechanism, the outer guide sheath defining a lumen extending from the proximal end portion to the distal end portion; an inner guide catheter positioned coaxially within the lumen of the outer guide catheter, the inner guide catheter having a proximal end portion, a first deflection portion, and a distal end portion each aligned in series along a length of the inner guide catheter, and having a steering assembly consisting essentially of a first steering mechanism, and the inner guide catheter defining a lumen extending from the proximal end portion to the distal end portion; an interventional catheter positioned coaxially within the lumen of the inner guide catheter, the interventional catheter having a proximal end portion and a distal end portion, and having an implantable fixation device coupled to the distal end portion; wherein the first deflection portion of the outer guide catheter is steerable to define a first outer-guide-catheter curve and the second deflection portion of the outer guide catheter is steerable to define a second outer-guide-catheter curve; and the first deflection portion of the inner guide catheter is steerable to define a first inner-guide-catheter curve.
2) The system of claim 1, wherein the first steering mechanism of the outer guide catheter is configured to steer the first deflection portion of the outer guide catheter, and the second steering mechanism of the outer guide catheter is configured to steer the second deflection portion of the outer guide catheter.
3) The system of claim 2, wherein each of the first outer-guide-catheter curve and the second outer-guide-catheter curve are each preformed in the outer guide catheter.
4) The system of claim 1, wherein the first steering mechanism of the inner guide catheter is configured to steer the first deflection portion of the inner guide catheter.
5) The system of claim 4, wherein the first inner-guide-catheter curve is preformed in the inner guide catheter.
6) The system of claim 1, wherein the second outer-guide-catheter curve is in a first plane and the first inner-guide-catheter curve is in a second plane.
7) The system of claim 6, wherein the first plane and the second plane are the same plane.
8) The system of claim 1, wherein the implantable fixation device comprises: a first arm and a second arm; a first proximal element moveable relative the first arm between a first position and a second position; and a second proximal element moveable relative to the second arm between a first position and a second position.
9) A method of repairing a tricuspid valve, comprising: providing a medical delivery system for accessing the tricuspid valve, including an outer guide catheter having a proximal end portion, a first deflection portion, a second deflection portion, and a distal end portion each aligned in series along a length of the outer guide catheter, and having a steering assembly comprising a first steering mechanism and a second steering mechanism, the outer guide catheter defining a lumen extending from the proximal end portion to the distal end portion, an inner guide catheter positioned coaxially within the lumen of the outer guide catheter, the inner guide catheter having a proximal end portion, a first deflection portion, and a distal end portion each aligned in series along a length of the inner guide catheter, and having a steering assembly consisting essentially of a first steering mechanism, and the inner guide catheter defining a lumen extending from the proximal end portion to the distal end portion, and an interventional catheter positioned coaxially within the lumen of the inner guide catheter, the interventional catheter having a proximal end portion and a distal end portion, and having an implantable fixation device coupled to the distal end portion; delivering the outer guide catheter to a right atrium via an inferior vena cava; actuating the first steering mechanism of the outer guide catheter to steer the first deflection portion of the outer guide catheter such that the distal end portion of the outer guide catheter moves within the right atrium relative the tricuspid valve; advancing the inner guide catheter longitudinally relative the outer guide catheter such that the first deflection portion of the inner guide catheter extends distally from the distal end portion of the outer guide catheter; actuating the first steering mechanism of the inner guide catheter to steer the first deflection portion of the inner guide catheter such that the distal end portion of the inner guide catheter moves within the right atrium relative the tricuspid valve; aligning the implantable fixation device with the tricuspid valve by operating the first and second steering mechanism of the outer guide catheter and the first steering mechanism of the inner guide catheter; and deploying the implantable fixation device to repair the tricuspid valve.
10) The method of claim 9, wherein the first deflection portion of the outer guide catheter is steerable to define a first outer-guide-catheter curve and the second deflection portion of the outer guide catheter is steerable to define a second outer-guide-catheter curve.
11) The method of claim 10, wherein the first deflection portion of the inner guide catheter is steerable to define a first inner-guide-catheter curve.
12) The method of claim 11, wherein the first outer-guide-catheter curve is in a first plane and the first inner-guide-catheter curve is in a second plane.
13) The method of claim 12, where in the first plane and the second plane are the same plane.
14) The method of claim 9, wherein the implantable fixation device comprises: a first arm and a second arm; a first proximal element moveable relative the first arm between a first position and a second position; and a second proximal element moveable relative to the second arm between a first position and a second position.
Description
CROSS-REFERENCE TO RELATED APPLICATIONS
[0001] [1] The present application claims the benefit of U.S. Provisional Patent Application No. 62/851,573, filed on May 22, 2019 and U.S. Provisional Patent Application No. 63/007,854, filed on Apr. 9, 2020, the full disclosures of which are hereby incorporated herein by reference.
BACKGROUND
[0002] Field of Disclosed Subject Matter
[0003] The disclosed subject matter is directed to medical devices for endovascular, percutaneous or minimally invasive surgical treatment of bodily tissues, such as tissue approximation or valve repair. More particularly, the present disclosure relates to repair of valves of the heart, such as the tricuspid valve, and venous valves.
[0004] The tricuspid valve regulates blood flow in the heart between the right atrium and the right ventricle. A properly functioning tricuspid valve opens and closes to enable blood flow in one direction--i.e., from the right atrium to the right ventricle. When the right ventricle contracts, the tricuspid valve closes to prevent blood from flowing backwards from the right ventricle to the right atrium, and blood is instead forced through the pulmonary valve and into the pulmonary arteries for delivery to the lungs. However, in some circumstances the tricuspid valve is unable to close properly, allowing blood to regurgitate back into the atrium. Such regurgitation can result in shortness of breath, fatigue, heart arrhythmias, and even heart failure.
[0005] Tricuspid valve regurgitation has several causes. Functional tricuspid valve regurgitation (FTR) is characterized by structurally normal tricuspid valve leaflets that are nevertheless unable to properly coapt with one another to close properly due to other structural deformations of surrounding heart structures. For example, the right ventricle can become dilated as a result of pulmonary hypertension or an abnormal heart muscle condition (cardiomyopathy).
[0006] Other causes of tricuspid valve regurgitation are related to degenerative valves and/or defects of the tricuspid valve leaflets, tricuspid valve annulus, or other tricuspid valve structures. In some circumstances, tricuspid valve regurgitation is a result of infective endocarditis, blunt chest trauma, rheumatic fever, Marfan syndrome, carcinoid syndrome, improper placement of pacemaker leads, or congenital defects to the structure of the heart.
[0007] Tricuspid valve conditions are also often associated with problems related to the left side of the heart, such as mitral valve regurgitation. In particular, FTR is often associated with left heart pathologies, though the tricuspid valve is typically left untreated during left heart surgeries. Left heart pathologies such as mitral valve regurgitation and stenosis can induce pressure and volume overload in the right ventricle, which in turn can induce ventricle enlargement and tricuspid annular dilation. Though often relatively mild at the time of treatment of the left heart, this annular dilation of the tricuspid valve can be progressive and asymmetric, and FTR can become more severe as time goes on. Reoperation for repair of the tricuspid valve is often needed owing to the degenerative character of the pathology.
Description of Related Art
[0008] Tricuspid valve regurgitation is often treated by replacing the tricuspid valve with a replacement valve implant. However, some patients are not suitable candidates for a valve replacement procedure.
[0009] Other treatment options involve repairing the valve through an interventional procedure. Surgical repair of bodily tissues can involve tissue approximation and fastening of such tissues in the approximated arrangement. When repairing valves, tissue approximation (also referred to as "edge-to-edge" repair technique) includes coapting the leaflets of the valve in a therapeutic arrangement which can then be maintained by fastening or fixing the leaflets. Preferably, devices and systems for tricuspid valve repair can be utilized without open chest access, and, rather, can be capable of being performed endovascularly, i.e., delivering repair devices (e.g., a fixation device, also referred to as a valve repair clip) using delivery systems advanced to the heart from a point in the patient's vasculature remote from the heart.
[0010] However, properly positioning and aligning a repair device with respect to the tricuspid valve can be difficult, particularly when approaching the tricuspid valve via the inferior vena cava. FIG. 1A illustrates a schematic cut-away, top-down view of the heart, including the location of the four heat valves (tricuspid, mitral, aortic, and pulmonary) as well as the approximate location of the inferior vena cava. The tricuspid valve typically includes three leaflets: posterior leaflet, anterior leaflet, and septal leaflet. When approaching the mitral valve via inferior vena cava, a delivery system will approach through (up through the page) the inferior vena cava, across the right atrium above the tricuspid valve, across the septum and into the left atrium, and back toward (down into the page) the mitral valve. When approaching the tricuspid valve via the inferior vena cava, a delivery system will approach through (up through the page) the inferior vena cava, then immediately back toward (down into the page) the tricuspid valve, all within the right atrium. This can make maneuverability of the distal end of the delivery system more challenging. As an example, the distal end portion of the delivery system must be steered across a severe angle within the right atrium without engaging the right atrium wall or interfering with the tricuspid valve prior to aligning and deploying the repair device. Accordingly, there is a need for devices and systems capable of accessing the tricuspid valve via the inferior vena cava. Such devices and systems likewise can be useful for repair of other heart valves and tissues in the body other than heart valves.
SUMMARY
[0011] The purpose and advantages of the disclosed subject matter will be set forth in and apparent from the description that follows, as well as will be learned by practice of the disclosed subject matter. Additional advantages of the disclosed subject matter will be realized and attained by the systems and methods particularly pointed out in the written description and claims hereof, as well as from the appended drawings.
[0012] To achieve these and other advantages and in accordance with the purpose of the disclosed subject matter, as embodied and broadly described, the disclosed subject matter is directed to systems and methods for repairing a tricuspid valve.
[0013] In accordance with the disclosed subject matter, a medical delivery system for accessing a tricuspid valve via an inferior vena cava is provided. The system includes an outer guide catheter, an inner guide catheter, and an interventional catheter. The outer guide catheter includes a proximal end portion, a first deflection portion, a second deflection portion, and a distal end portion each aligned in series along a length of the outer guide catheter. The outer guide catheter also includes a steering assembly comprising a first steering mechanism and a second steering mechanism. The outer guide catheter defines a lumen extending from the proximal end portion to the distal end portion. The inner guide catheter is position coaxially within the lumen of the outer guide catheter, and includes a proximal end portion, a first deflection portion, and a distal end portion each aligned in series along a length of the inner guide catheter. The inner guide catheter also includes a steering assembly consisting essentially of a first steering mechanism. The inner guide catheter defines a lumen extending from the proximal end portion to the distal end portion. The interventional catheter is positioned coaxially within the lumen of the inner guide catheter. The interventional catheter includes a proximal end portion and a distal end portion, and an implantable fixation device coupled to the distal end portion. The first deflection portion of the outer guide catheter is steerable to define a first outer-guide-catheter curve and the second deflection portion of the outer guide catheter is steerable to define a second outer-guide-catheter curve. The first deflection portion of the inner guide catheter is steerable to define a first inner-guide-catheter curve.
[0014] In accordance with the disclosed subject matter, the first steering mechanism of the outer guide catheter can be configured to steer the first deflection portion of the outer guide catheter, and the second steering mechanism of the outer guide catheter can be configured to steer the second deflection portion of the outer guide catheter. Each of the first outer-guide-catheter curve and the second outer-guide-catheter curve can each be preformed in the outer guide catheter. The first steering mechanism of the inner guide catheter can be configured to steer the first deflection portion of the inner guide catheter. The first inner-guide-catheter curve can be preformed in the inner guide catheter. The second outer-guide-catheter curve can be in a first plane and the first inner-guide-catheter curve can be in a second plane. The first plane and the second plane can be the same plane.
[0015] The implantable fixation device can include a first arm and a second arm, a first proximal element moveable relative the first arm between a first position and a second position, and a second proximal element moveable relative to the second arm between a first position and a second position.
[0016] In accordance with the disclosed subject matter, a method of repairing a tricuspid valve is provided. The method can include providing a medical delivery system for accessing the tricuspid valve. The medical delivery system can include an outer guide catheter, and inner guide catheter, and an interventional catheter. The outer guide catheter can have a proximal end portion, a first deflection portion, a second deflection portion, and a distal end portion each aligned in series along a length of the outer guide catheter, and a steering assembly including a first steering mechanism and a second steering mechanism. The outer guide catheter can define a lumen extending from the proximal end portion to the distal end portion. The inner guide catheter can be positioned coaxially within the lumen of the outer guide catheter. The inner guide catheter can include a proximal end portion, a first deflection portion, and a distal end portion each aligned in series along a length of the inner guide catheter, and a steering assembly consisting essentially of a first steering mechanism. The inner guide catheter can define a lumen extending from the proximal end portion to the distal end portion. The interventional catheter can be positioned coaxially within the lumen of the inner guide catheter. The interventional catheter can include a proximal end portion and a distal end portion, and have an implantable fixation device coupled to the distal end portion. The method can include delivering the outer guide catheter to a right atrium via an inferior vena cava. The method can further include actuating the first steering mechanism of the outer guide catheter to steer the first deflection portion of the outer guide catheter such that the distal end portion of the outer guide catheter moves within the right atrium relative the tricuspid valve and advancing the inner guide catheter longitudinally relative the outer guide catheter such that the first deflection portion of the inner guide catheter extends distally from the distal end portion of the outer guide catheter. The method can include actuating the first steering mechanism of the inner guide catheter to steer the first deflection portion of the inner guide catheter such that the distal end portion of the inner guide catheter moves within the right atrium relative the tricuspid valve and aligning the implantable fixation device with the tricuspid valve by operating the first and second steering mechanism of the outer guide catheter and the first steering mechanism of the inner guide catheter. The method can include deploying the implantable fixation device to repair the tricuspid valve.
[0017] The first deflection portion of the outer guide catheter can be steerable to define a first outer-guide-catheter curve and the second deflection portion of the outer guide catheter can be steerable to define a second outer-guide-catheter curve. The first deflection portion of the inner guide catheter can be steerable to define a first inner-guide-catheter curve. The first outer-guide-catheter curve can be in a first plane and the first inner-guide-catheter curve can be in a second plane. The first plane and the second plane can be the same plane.
[0018] The implantable fixation device can include a first arm and a second arm, a first proximal element moveable relative the first arm between a first position and a second position, and a second proximal element moveable relative to the second arm between a first position and a second position.
BRIEF DESCRIPTION OF THE FIGURES
[0019] FIG. 1 is a schematic top down, cut-away view of the heart showing the left and right atriums and the four heart valves.
[0020] FIG. 2 is a perspective view of an exemplary interventional catheter assembly in accordance with the disclosed subject matter.
[0021] FIG. 3 is a perspective view of an exemplary medical delivery system for accessing and repairing a heart valve, in accordance with the disclosed subject matter.
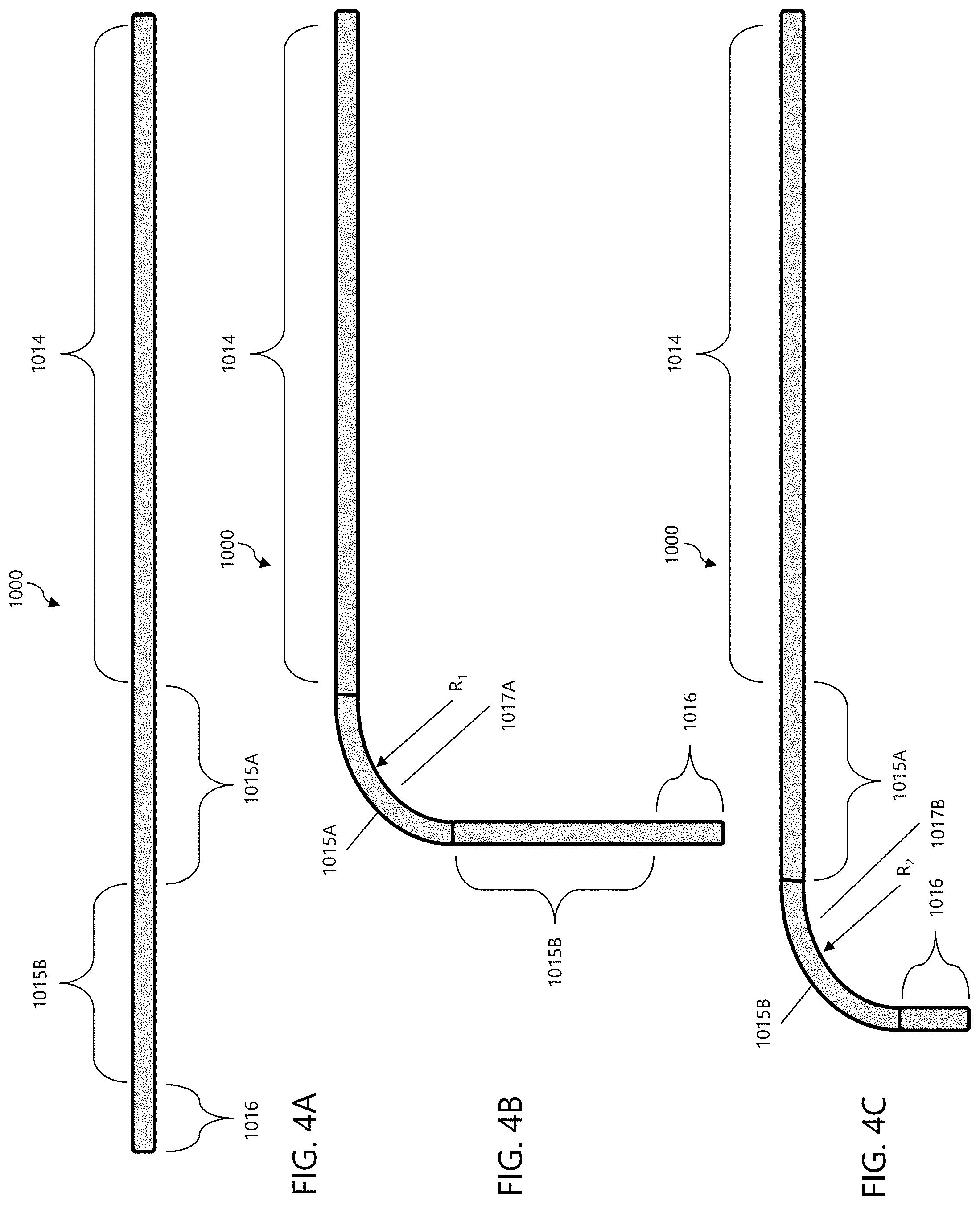
[0022] FIGS. 4A-C are schematic side views of a length of an exemplary outer guide catheter in accordance with the disclosed subject matter.
[0023] FIGS. 5A-5B are schematic side views of a length of an exemplary inner guide catheter in accordance with the disclosed subject matter.
[0024] FIGS. 6A-6B are side views of a distal end portion of exemplary catheters including steering mechanisms in accordance with the disclosed subject matter.
[0025] FIG. 7 is a perspective view of an exemplary tip ring in accordance with the disclosed subject matter.
[0026] FIG. 8 is a perspective view of a distal end portion of an exemplary catheter including multiple tip rings, in accordance with the disclosed subject matter.
[0027] FIG. 9A is a perspective detail view of the engagement between an exemplary outer guide catheter and an exemplary inner guide catheter including notches and protrusions, respectively, in accordance with the disclosed subject matter.
[0028] FIG. 9B is a cross-section view of the outer guide catheter of FIG. 9A.
[0029] FIG. 9C is a cross-section view of the inner guide catheter of FIG. 9A.
[0030] FIG. 10 is a schematic top down view of a tricuspid valve.
[0031] FIG. 11 is a perspective view of an exemplary embodiment of a fixation device for use in accordance with the disclosed subject matter.
[0032] FIG. 12 is a front view of the fixation device of FIG. 11 at a different position, wherein optional arms of greater length are depicted in dashed lines.
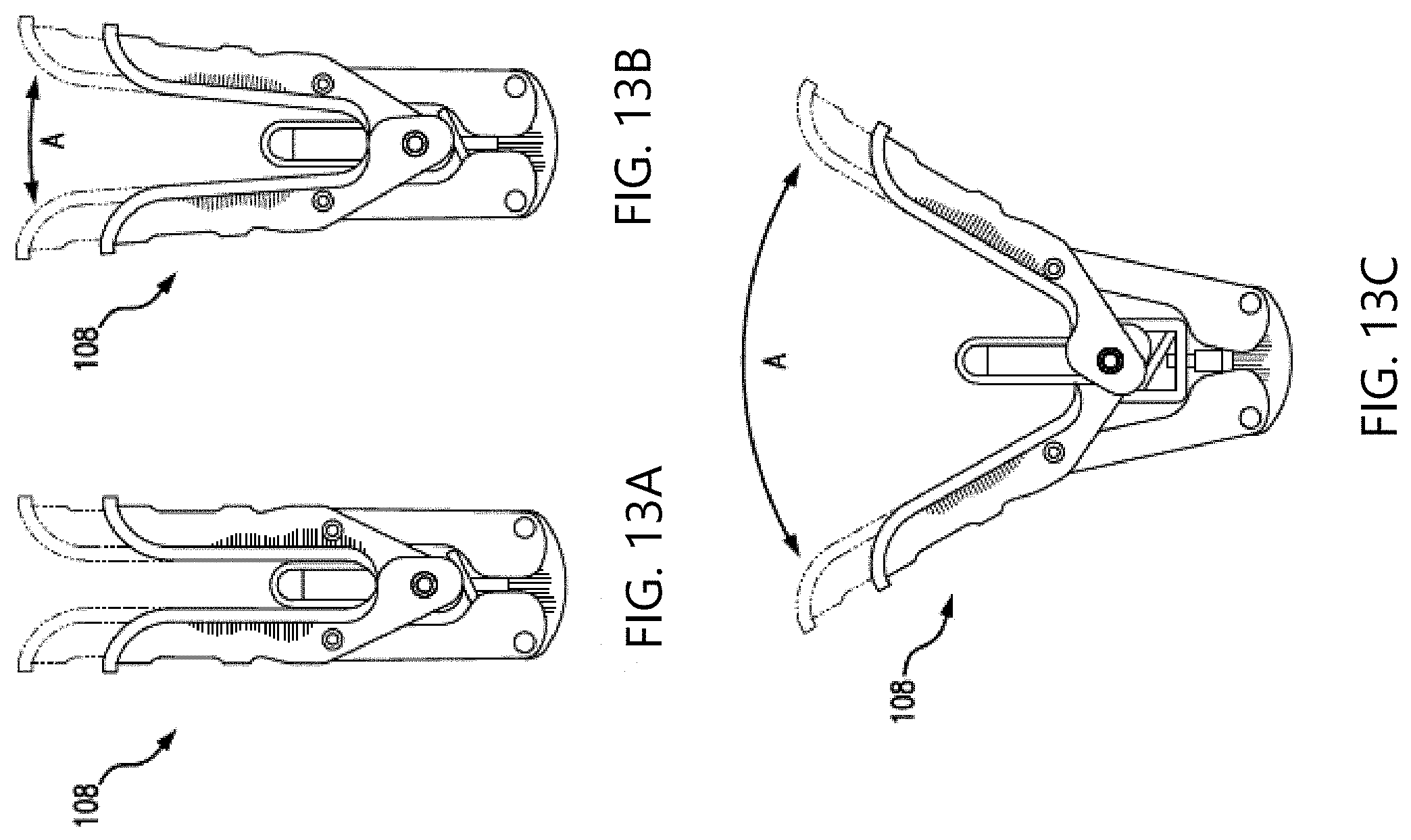
[0033] FIGS. 13A-13C are front views of the fixation device of FIG. 11 at various positions, wherein optional arms of greater length are depicted with dashed lines.
[0034] FIG. 14A is a front schematic view of the fixation device of FIG. 11 having leaflets captured therein.
[0035] FIG. 14B is a side view of the fixation device of FIG. 11 schematically depicting a contact patch area.
[0036] FIG. 15 is flow chart of a method of repairing a tricuspid valve in accordance with the disclosed subject matter.
DETAILED DESCRIPTION
[0037] Reference will now be made in detail to the various exemplary embodiments of the disclosed subject matter, exemplary embodiments of which are illustrated in the accompanying drawings.
[0038] Transcatheter (e.g., trans-septal) edge-to-edge valve repair for the mitral valve has been established using a fixation device, such as the MitraClip Transcatheter Mitral Valve Repair device. These fixation devices generally are configured to capture and secure opposing native leaflets using two types of leaflet contacting elements. The first element is a sub-valvular arm (also known as a distal element or fixation element) to contact the ventricular side of a native leaflet to be grasped. With the arm positioned underneath to stabilize the native leaflet in a beating heart, a second gripping element (also known as a proximal element) can be lowered or moved into contact with the atrial side of the native leaflet to capture the leaflet therebetween. Once each opposing leaflet is captured by a respective arm and gripper element, the fixation device can be closed by moving the arms toward a center of the fixation device such that the leaflets are brought into coaptation, which results in a reduction in valvular regurgitation during ventricular systole. Furthermore, a covering can be provided on the arms and/or gripper elements to facilitate tissue ingrowth with the captured leaflets. Such fixation devices can be delivered to the mitral valve using a delivery system. There is also evidence that the MitraClip device can be useful in tricuspid valve repair.
[0039] Additional details of exemplary fixation devices and delivery systems in accordance with the disclosed subject matter are set forth below. Furthermore, various patents and published applications disclose additional details of such fixation devices and delivery systems and related operations, for example, U.S. Pat. No. 7,226,467 to Lucatero et al., U.S. Pat. No. 7,563,267 to Goldfarb et al., U.S. Pat. No. 7,655,015 to Goldfarb et al., U.S. Pat. No. 7,736,388 to Goldfarb et al., U.S. Pat. No. 7,811,296 to Goldfarb et al., U.S. Pat. No. 8,057,493 to Goldfarb et al., U.S. Pat. No. 8,303,608 to Goldfarb et al., U.S. Pat. No. 8,500,761 to Goldfarb et al., U.S. Pat. No. 8,734,505 to Goldfarb et al., U.S. Pat. No. 8,740,920 to Goldfarb et al., U.S. Pat. No. 9,510,829 to Goldfarb et al., U.S. Pat. No. 7,635,329 to Goldfarb et al., U.S. Pat. No. 8,945,177 to Dell et al., U.S. Pat No. 9,011,468 to Ketai et al., U.S. Patent Application Publication No. 2017/0042546 to Goldfarb et al., U.S. Patent Application Publication No. 2018/0146966 to Hernandez et al., U.S. Patent Application Publication No. 2017/0239048 to Goldfarb et al., U.S. Patent Application Publication No. 2018/0325671 to Abunassar et al., the entirety of the contents of each of these patents and published applications is incorporated herein by reference.
[0040] In accordance with the disclosed subject matter, a medical delivery system for accessing a tricuspid valve via an inferior vena cava is provided. The system includes an outer guide catheter, an inner guide catheter, and an interventional catheter. The outer guide catheter includes a proximal end portion, a first deflection portion, a second deflection portion, and a distal end portion each aligned in series along a length of the outer guide catheter. The outer guide catheter also includes a steering assembly comprising a first steering mechanism and a second steering mechanism. The outer guide catheter defines a lumen extending from the proximal end portion to the distal end portion. The inner guide catheter is position coaxially within the lumen of the outer guide catheter, and includes a proximal end portion, a first deflection portion, and a distal end portion each aligned in series along a length of the inner guide catheter. The inner guide catheter also includes a steering assembly consisting essentially of a first steering mechanism. The inner guide catheter defines a lumen extending from the proximal end portion to the distal end portion. The interventional catheter is positioned coaxially within the lumen of the inner guide catheter. The interventional catheter includes a proximal end portion and a distal end portion, and an implantable fixation device coupled to the distal end portion. The first deflection portion of the outer guide catheter is steerable to define a first outer-guide-catheter curve and the second deflection portion of the outer guide catheter is steerable to define a second outer-guide-catheter curve. The first deflection portion of the inner guide catheter is steerable to define a first inner-guide-catheter curve.
[0041] Referring to FIG. 2 for purpose of illustration and not limitation, an exemplary interventional catheter assembly 300 is provided for delivery of a fixation device, such as fixation device 104 (described in greater detail below). That is, the interventional catheter assembly 300 can be used to introduce and position a fixation device 104. The interventional catheter assembly 300 can include an interventional catheter 302, having a proximal end portion 322 and a distal end portion 324, and a handle 304 attached to the proximal end portion 322. A fixation device 104 can be removably coupleable to the distal end portion 324 for delivery to a site within the body, for example, the tricuspid valve. Thus, extending from the distal end portion 324 is actuator rod 64. The actuator rod 64 is connectable with the fixation device 104 and can act to manipulate the fixation device 104, for example, opening and closing the arms. Handle 304 of the interventional catheter assembly 300 is shown, including main body 308, proximal element line handle 312, lock line handle 310, the actuator rod control 314, and the actuator rod handle 316, among other features.
[0042] Referring to FIG. 3 for purpose of illustration and not limitation, medical delivery system 1 including an outer guide catheter 1000 and an inner guide catheter 1020 (e.g., collectively steerable guide system 3) and interventional catheter assembly 300 is provided. The steerable guide system 3 can include one or more steerable catheter components. For example, and not limitation, steerable guide system 3 can include an outer guide catheter 1000, having a proximal end portion 1014 and a distal end portion 1016, and an inner guide catheter 1020, having a proximal end portion 1024 and a distal end portion 1026, wherein the inner guide catheter 1020 is positioned coaxially within the outer guide catheter 1000, as shown. In addition, a hemostatic valve 1090 can be disposed within handle 1056, or external to handle 1056 as shown, to provide leak-free sealing with or without the inner guide catheter 1020 in place. The distal end portions 1016, 1026 of guide catheters 1000, 1020, respectively, are sized to be passable to a body cavity, typically through a body lumen such as a vascular lumen.
[0043] Referring to FIGS. 4A-4C for purpose of illustration and not limitation, outer guide catheter 1000 can include a proximal end portion 1014, a first deflection portion 1015A, a second deflection portion 1015B, and a distal end portion 1016 each aligned in series along a length of the outer guide catheter 1000. The first deflection portion 1015A can be steerable to define a first outer-guide catheter curve 1017A. First outer-guide catheter curve 1017A can have a radius of curvature R.sub.1. The radius of curvature R.sub.1 can be suitable for positioning within the right atrium proximate the tricuspid valve with the outer guide catheter 1000 extending from the vena cava. As such, distal end portion 1016 can be deflected to the appropriate angle by steering the outer guide catheter 1000 at deflection portion 1015A. The second deflection portion 1015B can be steerable to define a second outer-guide catheter curve 1017B. Second outer-guide catheter curve 1017B can have a radius of curvature R.sub.2. The radius of curvature R.sub.2 can be suitable for positioning within the right atrium proximate the tricuspid valve with the outer guide catheter 1000 extending from the vena cava. As such, distal end portion 1016 can be deflected to the appropriate angle by steering the outer guide catheter 1000 at deflection portion 1015B. First outer-guide catheter curve 1017A and second outer-guide catheter curve 1017B can be in the same plane or in different planes. For example, first outer-guide catheter curve 1017A and second outer-guide catheter curve 1017B can exist on planes that are orthogonal to one another. The proximal end portion 1014, first deflection portion 1015A, second deflection portion 1015B, and distal end portion 1016 can each have a respective length that can be suitable for positioning within the right atrium proximate the tricuspid valve with the outer guide catheter 1000 extending from the vena cava.
[0044] Referring to FIGS. 5A-5B for purpose of illustration and not limitation, inner guide catheter 1020 can include a proximal end portion 1024, deflection portion 1025, and distal end portion 1026 each aligned in series along a length of the outer guide catheter. The deflection portion 1025 can be steerable to define an inner guide-catheter curve 1027. The inner-guide catheter curve 1027 can have a radius of curvature R.sub.3. The radius of curvature R.sub.3 can be suitable to align with the tricuspid valve when the inner guide catheter 1020 is extending from the outer guide catheter 1000. As such, distal end portion 1026 can be deflected to an appropriate angle by steering the inner guide catheter 1020 at deflection portion 1025. The inner guide-catheter curve 1027 can be in a plane, for example, the same plane as second outer-guide catheter curve 1017B. For example, the inner guide catheter 1020 and the outer guide catheter 1000 can be provided with markers, intended to manually align the two planes, or can be provide with mating or engaging features (such as keying features, as described in greater detail below) to self-align as desired. When the inner-guide catheter curve 1027 and second outer-guide catheter curve 1017B are in the same plane, both guide catheters 1000, 1020 can be adjusted to achieve proper position relative the tricuspid valve (e.g., alignment relative the valve and height above the valve) such as by compensating for one another, as set forth in greater detail below. The proximal end portion 1024, deflection portion 1025, and distal end portion 1026 can each have a respective length that can be suitable for positioning within the right atrium proximate the tricuspid valve when the inner guide catheter 1020 is extending from the outer guide catheter 1000. When inner guide catheter 1020 includes one deflection portion (i.e., deflection portion 1025), a limited portion of the inner guide catheter 1020 (e.g., distal end portion 1026 and deflection portion 1025) can extend from the outer guide catheter 1000 to be steered within the right atrium. Adding additional deflection portions can require additional portions of the inner guide catheter 1020 to extend from the outer guide catheter 1000. However, to achieve a more acute delivery angle (for example, the inner guide catheter curve 1027) it can be beneficial to maintain a small profile and omit extraneous catheter features for the inner guide catheter 1020. Therefore, inner guide catheter 1020 can include one deflection portion (i.e., deflection portion 1025).
[0045] The curvatures can be formed in catheters 1000, 1020 by precurving, steering or any suitable means. For example, guide catheters 1000, 1020 can be curved by a combination of precurving and steering. Precurving involves preforming or setting a specific curvature in the catheter prior to usage, such as by heat setting a polymer or by utilizing a shape-memory alloy. Since the catheters are generally flexible, steering can be used to straighten the catheter throughout the deflection portions 1015A, 1015B, 1025. Once the catheter is positioned in the anatomy, the steering can be adjusted and the catheter can relax or bias back toward the precurved setting.
[0046] Steering assemblies can be used to steer guide catheters 1000, 1020. The steering assemblies can include one or more steering mechanisms, such as cables or pull wires within the wall of the guide catheters 1000, 1020. For example, a steering mechanism can be provided for each curve portion, such that the outer guide catheter 1000 can include a first steering mechanism to steer the first outer-guide catheter curve 1017A and a second steering mechanism to steer the second outer-guide catheter curve 1017B. The inner guide catheter 1020 can include a first steering mechanism to steer the inner-guide catheter curve 1027. To achieve a more acute delivery angle (for example, the inner guide catheter curve 1027) it can be beneficial to maintain a small profile and omit extraneous catheter features for the inner guide catheter 1020. Therefore inner guide catheter 1020 can consist essentially of a single steering mechanism (i.e., the first steering mechanism).
[0047] Referring to FIG. 6A for purpose of illustration and not limitation, the outer guide catheter 1000 can include one or more pull wires 1111, 1112 slidably disposed in lumens within the wall of the catheter 1000 and extending to the distal end portion 1016. By applying tension to the pull wire 1111 in the proximal direction, the distal end portion 1016 curves in the direction of the pull wire 1111 as illustrated by arrow 1113. Likewise, by applying tension to pull wire 1112 in the proximal direction, the distal end portion 1016 curves in the direction of pull wire 1112 as illustrated by arrow 1114. Diametrically opposing placement of pull wires 1111, 1112 within the walls of guide catheter 10000 allows the distal end portion 1016 to be steered in opposite directions 1113, 1114. This can provide a means of correcting or adjusting a curvature. For example, if tension is applied to one pull wire to create a curvature, the curvature can be lessened by applying tension to the diametrically opposite pull wire. Referring to FIG. 6B for purpose of illustration and not limitation, an additional set of opposing pull wires 1111' and 1112' can extend within the wall of guide catheter 1000 to steer guide catheter 1000 toward arrows 1113', 1114', respectively. This combination of pull wires 1111, 1112, 1111', 1112' can allow guide catheter 1000 to be curved along first outer-guide catheter curve 1017A and second outer-guide catheter curve 1017B. For example, pull wires 1111, 1112 can be a first steering mechanism and can be used to steer along first outer-guide catheter curve 1017A and pull wires 1111', 1112' can be a second steering mechanism and can be used to steer along second outer-guide catheter curve 1017B. As another example and not by way of limitation, guide catheter 1000 can include two pull wires, for example pull wire 1111 which can be a first steering mechanism and can be used to steer along first outer-guide catheter curve 1017A and pull wire 1111' which can be a second steering mechanism and can be used to steer along second outer-guide catheter curve 1017B. Inner guide catheter 1020, which can be steerable at deflection portion 1025, can include one pull wire 1121 (not shown), which can be a first steering mechanism, or one set of opposing pull wires 1121, 1122 (not shown), which can be a first steering mechanism, to steer along inner guide-catheter curve 1027.
[0048] In accordance with the disclosed subject matter, pull wires 1111, 1112, 1111', 1112' and associated lumens can be placed in any arrangement, singly or in pairs, symmetrically or nonsymmetrically, and any number of pull wires can be present. This can allow curvature in any direction and about various axis. The pull wires 1111, 1112, 1111', 1112' can be fixed at any location along the length of the catheter by any suitable method, such as by gluing, tying, soldering, or potting. When tension is applied to the pull wire, the curvature is formed from the point of attachment of the pull wire toward the proximal direction. Therefore, curvatures can be formed throughout the length of the catheter depending upon the locations of the points of attachment of the pull wires. The pull wires can be attached near the distal end of the catheter, the distal end of the first deflection portion 1015A, the distal end of the second deflection portion 1015B, or the distal end of the deflection portion 1025, for example, using tip ring 280, illustrated in FIG. 7. As shown, the pull wire 1111 can pass through an orifice 286 in the tip ring 280, form a loop shape, and pass back through the orifice 286 and travel back through the catheter wall (not shown). The loop formed can be captured by a portion (not shown) of the tip ring 280. In accordance with the disclosed subject matter, catheter 1000 can include two or more tip rings 280 located at different locations along the length of catheter 1000. Referring to FIG. 8 for example, and not by way of limitation, catheter 1000A includes two tip rings 280A, 280B located at different locations along the length of catheter 1000A. Pull wire 1111A passes through an orifice in tip ring 280A, forms a loop shape, and passes back through the orifice to travel back through the catheter wall. Pull wire 1111A' extends through tip ring 280A to tip ring 280B, passes through an orifice in tip ring 280B, forms a loop shape, and passes back through the orifice to travel back through the catheter wall. As noted above, such a configuration can cause the curvature formed by pull wire 1111A to have a different location than the curvature formed by pull wire 1111A'.
[0049] Additionally or alternatively, precurvature of the catheter can focus the location of the curvature. For example, when the catheter is precurved at a deflection portion 1015A, 1015B, 1025, the pull wires can be used to straighten the deflection portion 1015A, 1015B, 1025 or allow the deflection portion to relax toward the predefined curve. In addition, the lumens which house the pull wires can be straight or curved.
[0050] The outer guide catheter 1000 and inner guide catheter 1020 can have similar or different construction which can include any suitable material or combination of materials to create the above described curvatures. For example, when the guide catheter 1000, 1020 is precurved in addition to being steerable, the guide catheter 1000, 1020 can include a polymer or copolymer which is able to be set in a desired curve, such as by heat setting. Likewise, the guide catheter 1000, 1020 can include a shape-memory alloy.
[0051] Additionally or alternatively, the guide catheter 1000, 1020 can include one or more of a variety of materials, either along the length of the guide catheter 1000, 1020, or in various segments (e.g., 1014, 1015A, 1015B, 1016). Example materials can include polyurethane, Pebax, nylon, polyester, polyethylene, polyimide, polyethylenetelephthalate (PET), or polyetheretherketone (PEEK). In addition, the walls of the guide catheter 1000, 1020 can include multiple layers of materials and can be reinforced with a variety of structures, such as metal braids or coils. Such reinforcements can be along the length of the guide catheter 1000, 1020, or in various segments (e.g., 1014, 1015A, 1015B, 1016).
[0052] In accordance with the disclosed subject matter, one or more of outer guide catheter 1000, inner guide catheter 1020, and interventional catheter 302 can be combined as a catheter assembly. For example, outer guide catheter 1000 and inner guide catheter 1020 can be combined as a catheter assembly. As another example, inner guide catheter 1020 and interventional catheter 302 can be combined as a catheter assembly. As another example, outer guide catheter 1000, inner guide catheter 1020, and interventional catheter 302 can be combined as a catheter assembly.
[0053] Referring to FIGS. 9A-9C for purpose of illustration and not limitation, outer guide catheter 1000 and inner guide catheter 1020 can include a keying feature. The keying feature can be used to maintain rotational relationship between the guide catheters 1000, 1020 to assist in steering capabilities. For example, inner guide catheter 1020 can include one or more protrusions 1400 which can extend radially outwardly. FIG. 9A illustrates four protrusions 1400, equally spaced around the exterior of the inner guide catheter 1020. Likewise, outer guide catheter 1000 can include corresponding notches 1402, which can align with the protrusions 1400. FIG. 9A illustrates four notches 1402 equally spaced around the central lumen 1018. Thus, inner guide catheter 1020 is able to be translated within outer guide catheter 1000, however rotation of inner guide catheter 1020 is prevented by the keying features, i.e., the interlocking protrusions 1400 and notches 1402. Such keying can help maintain a known correlation of position between the inner guide catheter 1020 and outer guide catheter 1000. Although the protrusions and notches are illustrated on the inner guide catheter 1020, and outer guide catheter 1000, respectively, the protrusions and/or notches can be on either the inner guide catheter 1020 and outer guide catheter 1000, which corresponding protrusions or notches on the other.
[0054] FIG. 9B illustrates a cross-sectional view of outer guide catheter 1000 of FIG. 9A. The catheter includes a notched layer 1404 along the inner surface of the central lumen 1018. The notched layer 1404 can include notches 1402 in any size, shape, arrangement and number. Optionally, the notched layer 1404 can include lumens 1406, for passage of pull wires 1111, 1112, 1111', 1112'. However, lumens 1406 can alternatively or additionally have other uses. Notched layer 1404 can be incorporated into the wall of outer guide catheter 10000, such as by extrusion, or can be a separate layer positioned within the outer guide catheter 1000. Notched layer 1404 can extend the entire length of outer guide catheter 1000, the entire length of one or more segments 1014, 1015A, 1015B, 1016, or along a portion of one or more segments 1014, 1015A, 1015B, 1016, including a small strip at a designated location along the length of outer guide catheter 1000.
[0055] FIG. 9C illustrates a cross-sectional view of the inner guide catheter 1020 of FIG. 9A. The inner guide catheter 1020 includes protrusions 1400 along the outer surface of the inner guide catheter 1020. The protrusions 1400 can be of any size, shape, arrangement and number. Protrusions can be incorporated into the wall of inner guide catheter 1020, such as by extrusion, or can be included in a separate cylindrical layer on the outer surface of the inner guide catheter 1020. Alternatively, the protrusions 1400 can be individually adhered to the outer surface of guide catheter 1020. Protrusions can extend the entire length of inner guide catheter 1020, the entire length of one or more segments 1024, 1025, 1026, or along a portion of one or more segments 1024, 1025, 1026, including a small strip at a designated location along the length of inner guide catheter 1020.
[0056] In accordance with the disclosed subject matter, outer guide catheter 1000 and inner guide catheter 1020 can be provided without keying features.
[0057] Referring again to FIGS. 2 and 3 for purpose of illustration and not limitation, manipulation of the guide catheters 1000, 1020 can be achieved with the use of handles 1056, 1057 attached to the proximal end portions 1014, 1024 of catheters 1000, 1020, respectively. As shown, handle 1056 is attached to the proximal end portion 1014 of outer guide catheter 1000 and handle 1057 is attached to the proximal end portion 1024 of inner guide catheter 1020. Inner guide catheter 1020 is inserted through handle 1056 and is positioned coaxially within outer guide catheter 1000. The interventional catheter 302 can be inserted though handle 1057 and can be positioned coaxially within inner guide catheter 1020 and outer guide catheter 1000.
[0058] Handle 1056 can include two steering knobs 1300A, 1300B emerging from a handle housing 1302 for manipulation by the user. Steering knob 1300A can be disposed on the side of housing 1302 and steering knob 1300B can be disposed on a face of the housing 1302. Steering knob 1300A can be coupled to pull wires 1111, 1112, which can be arranged to steer the second deflection portion 1015B of outer guide catheter 1000. Steering knob 1300B can be coupled to pull wires 1111', 1112', which can be arranged to steer the first deflection portion 1015A of outer guide catheter 1000. Although the steering knobs are described as steering particular deflection portions, the steering knobs can steer any deflection portion. Handle 1057 can include one steering knob 1300C emerging from a handle housing 1302A for manipulation by the user. Steering knob 1300C can be disposed on a face of the housing 1302A. Steering knob 1300C can be coupled to pull wires 1121, 1122, which can be arranged to steer the deflection portion 1025 of inner guide catheter 1020. Although the steering knobs are described in particular locations, placement can be based on a variety of factors, including type of steering mechanism, size and shape of handle, type and arrangement of parts within handle, and ergonomics, among others. Furthermore, while control of the pull wires is illustrated with steering knobs, any control mechanisms can be used, including, for example, sliders, triggers or actuatable handles.
[0059] Referring to FIG. 10 for purpose of illustration and not limitation, FIG. 10 provides a top-down, cut-away view of the tricuspid valve. FIG. 10 also shows the axis that will be used while describing positioning the fixation device 104 relative to the tricuspid valve. Particularly, the aortic-posterior axis includes the aortic direction, which is toward the anterior leaflet of the tricuspid valve (and the aorta) and the posterior direction, which is toward the posterior leaflet of the tricuspid valve. The septal-lateral axis includes the septal direction, which is toward the septal leaflet of the tricuspid valve and the lateral direction, which is toward the aortic-posterior commissure. In addition to being properly aligned along the aortic-posterior axis and septal-lateral axis relative to the tricuspid valve, the fixation device 104 can be positioned at the proper height relative to the tricuspid valve. As used herein, gaining height will refer to moving away from the tricuspid valve (up out of the page) and losing height will refer to moving toward the tricuspid valve (down into the page).
[0060] In operation, the medical delivery system 1 can be used to properly position the fixation device 104 relative to the tricuspid valve. To properly position the fixation device 104, steering knob 1300A, 1300B, and 1300C can be used. Additionally, all or a portion of the delivery system 1 can be advanced, and all or a portion of the delivery system 1 can be rotated. For example, positioning can be controlled by the following actions.
TABLE-US-00001 Device Axial Height Maneuver movement Effect Advance entire Toward aortic direction May gain height delivery system 1 Retract entire Toward posterior direction May lose height delivery system 1 Steering knob 1300B Toward septal direction May gain height clockwise (CW) Steering knob 1300B Toward lateral direction May lose height counter clock wise (CCW) Steering knob 1300A CW Toward posterior/ Lose height septal direction Steering knob 1300A CCW Toward aortic/ Gain height septal direction Steering knob 1300C CW Toward posterior/ Lose height septal direction Steering knob 1300C CCW Toward aortic/ Gain height septal direction Rotate handle 300 CW Toward septal direction May gain height Rotate handle 300 CCW Toward lateral direction May lose height
Positioning of the fixation device 104 can be achieved with iterative adjustments of the delivery system 1 using translation (advance/retract), torque (rotating handle 300), and knob adjustments (as described above). Steering knobs 1300A, 1300C, and translation of delivery system 1 can be used as the primary movements for successful positioning. Because steering knobs 1300A and 1300C control steering through the second outer-guide catheter curve 1017B and the inner-guide catheter curve 1027, respectively, which can be co-planar, steering knobs 1300A and 1300C can be adjusted to maintain proper height and alignment, and can compensate for each other. Once the fixation device 104 is properly positioned relative to the tricuspid valve, the leaflets can be grasped, as set forth below, and the fixation device 104 can be released for implantation.
[0061] Referring to FIGS. 11-14 for purpose illustration and not limitation, an exemplary fixation device 104 for fixation of native leaflets of a heart valve is disclosed herein. The fixation device 104 as embodied herein can include a central assembly 171. The central assembly 171 can include various central components for operation and release of the fixation device 104 for example, a coupling member 174 as described in the disclosures of the patents and applications incorporated by reference herein. The fixation device 104 as depicted can include at least one arm 108 moveably coupled to the central assembly 171. As shown, the fixation device 104 can further include a second arm 110 moveably coupled to the central assembly 171.
[0062] With reference to FIG. 12, and further in accordance with the disclosed subject matter, each arm 108, 110 can be rotatable about a respective axis point 148, 150 between closed, open and inverted positions, as well as any position therebetween. Furthermore, the arms 108, 110 can be selected from a range of suitable lengths, wherein the appropriate length can be selected by the physician or health care provided, for example after inspection of a patient. For purpose of comparison, a first length of each arm 108, 110 is depicted in FIG. 12 in solid lines, and a second longer length of each arm of the disclosed subject matter is depicted in dashed lines. The arms in solid lines can be an entirely separate arm with a different length as compared to the arm in dashed lines.
[0063] As depicted herein in FIGS. 13A-13C, various positions of the fixation device 104 are depicted for purpose of illustration and not limitation. Elongated arms are illustrated in dashed lines for comparison to shorter arms (in solid lines). In FIG. 13A, the fixation device 104 is in the closed position, wherein the arms are positioned axially in alignment, e.g., vertically or nearly vertically as shown. FIGS. 13B and 13C illustrate the arms positioned with an angle A between each other. In FIG. 13B, angle A is about 10 degrees, and in FIG. 13C, angle A is about 60 degrees. As disclosed herein, the fixation device 104 is in the closed position when angle A is about 30 or less degrees. Although not depicted, the arms can continue to open until angle A exceeds 180 degrees, e.g., inverted.
[0064] The fixation device 104 can further include at least one gripping element 116 moveable relative to the at least one arm 108 to capture native leaflet therebetween. In accordance with the disclosed subject matter, each arm can be configured to define or have a trough aligned along the longitudinal axis. The trough can have a width sized greater than a width of the gripper element so as to receive the gripper element therein.
[0065] The fixation device 104 can further include a second gripping element 118 moveable relative to the second arm 110 to capture a second native leaflet therebetween. Further, in accordance with the disclosed subject matter, the at least one gripping element 116, 118 can have at least one friction element 152 along a length thereof. As embodied herein, each gripping element 116, 118 can include a plurality of friction elements 152, which can be disposed in rows. For example, each gripping element 116 and 118 can have a least four rows of friction elements 152. The friction elements 152 can allow for improved tissue engagement during leaflet capture. This gripping element design can increase the assurance that single device leaflet detachment will not occur during or after a procedure. To adjust the fixation device 104 after an initial leaflet capture, the arms can be opened, the gripping element can be raised vertically, and tissue can disengage from the fixation device 104, facilitating re-grasp and capture.
[0066] As further embodied herein, each gripping element 116, 118 can be biased toward each respective arm 108, 110. Prior to leaflet capture, each gripping element 116, 118 can be moved inwardly toward a longitudinal center of the device (e.g., away from each respective arm 108, 110) and held with the aid of one or more gripper element lines (not shown), which can be in the form of sutures, wire, nitinol wires, rods, cables, polymeric lines, or other suitable structures. The sutures can be operatively connected with the gripping elements 116, 118 in a variety of ways, such as by being threaded though loops disposed on gripping elements 116, 118.
[0067] Fixation device 104 can further include two link members or legs 168, and as embodied herein, each leg 168 has a first end rotatably joined with one of the arms 108, 110 and a second end rotatably joined with a base 170. The base 170 can be operatively connected with a stud 176 which can be operatively attached to an actuator rod 64 of the delivery system (see FIG. 9). In some embodiments, the stud 176 can be threaded such that the actuator rod 64 can attach to the stud 176 by a screw-type action. Further, the connection point between the stud 176 and the actuator rod 64 can be disposed within the coupling member 174. However, the actuator rod 64 and stud 176 can be operatively connected by any mechanism which is releasable to allow the fixation device 104 to be detached. The stud 176 can be axially extendable and retractable to move the base and therefore the legs 168, which can rotate the arms 108, 110 between closed, open and inverted positions. Immobilization of the stud, such as by a locking mechanism, can hold the legs 168 in place and therefore lock the arms 108, 110 in a desired position. Further details are disclosed in the patents and published applications incorporated by reference herein.
[0068] As previously noted, a native leaflet can be captured between each arm and respective gripping element. Each arm can then be moved toward its closed position. In this matter, adjacent leaflets can further be captured between the arms in the closed position. For example, and for illustration only, FIGS. 14A and 14B show the fixation device 104 depicted with arms 108, 110 at an angle A of about 10 to 30 degrees with two leaflets captured therebetween, wherein each leaflet is captured between an arm and a respective gripping element (gripping elements not shown). As illustrated in FIG. 14B, a contact patch area 222 depicted in dashed lines and is defined by the area of tissue captured between the arms. The contact patch area 222 can depict a tissue-to-tissue contact patch area defined by area of a leaflet in contact with a counterpart leaflet. As previously noted, FIG. 14B depicts the contact patch area 222 when the fixation device 104 is oriented at angle A of about 10 to 30 degrees.
[0069] FIG. 15 illustrates an exemplary method 10000 for repairing a tricuspid valve in accordance with the disclosed subject matter. The method can begin at step 10100, where the method includes providing a medical delivery system for accessing the tricuspid valve. The medical delivery system includes an outer guide catheter having a proximal end portion, a first deflection portion, a second deflection portion, and a distal end portion each aligned in series along a length of the outer guide catheter, and having a steering assembly comprising a first steering mechanism and a second steering mechanism, the outer guide catheter defining a lumen extending from the proximal end portion to the distal end portion, an inner guide catheter positioned coaxially within the lumen of the outer guide catheter, the inner guide catheter having a proximal end portion, a first deflection portion, and a distal end portion each aligned in series along a length of the inner guide catheter, and having a steering assembly consisting essentially of a first steering mechanism, and the inner guide catheter defining a lumen extending from the proximal end portion to the distal end portion, and an interventional catheter positioned coaxially within the lumen of the inner guide catheter, the interventional catheter having a proximal end portion and a distal end portion, and having an implantable fixation device coupled to the distal end portion At step 10200 the method includes delivering the outer guide catheter to a right atrium via an inferior vena cava. At step 10300 the method includes actuating the first steering mechanism of the outer guide catheter to steer the first deflection portion of the outer guide catheter such that the distal end portion of the outer guide catheter moves within the right atrium relative the tricuspid valve. At step 10400 the method includes advancing the inner guide catheter longitudinally relative the outer guide catheter such that the first deflection portion of the inner guide catheter extends distally from the distal end portion of the outer guide catheter. At step 10500 the method includes actuating the first steering mechanism of the inner guide catheter to steer the first deflection portion of the inner guide catheter such that the distal end portion of the inner guide catheter moves within the right atrium relative the tricuspid valve. At step 10600 the method includes aligning the implantable fixation device with the tricuspid valve by operating the first and second steering mechanism of the outer guide catheter and the first steering mechanism of the inner guide catheter. At step 10700 the method includes deploying the implantable fixation device to repair the tricuspid valve. In accordance with the disclosed subject matter, the method can repeat one or more steps of the method of FIG. 15, where appropriate. Although this disclosure describes and illustrates particular steps of the method of FIG. 15 as occurring in a particular order, this disclosure contemplates any suitable steps of the method of FIG. 15 occurring in any suitable order. Moreover, although this disclosure describes and illustrates an example method repairing a tricuspid valve including the particular steps of the method of FIG. 15, this disclosure contemplates any suitable method for repairing a tricuspid valve including any suitable steps, which can include all, some, or none of the steps of the method of FIG. 15, where appropriate. Furthermore, although this disclosure describes and illustrates particular components, devices, or systems carrying out particular steps of the method of FIG. 15, this disclosure contemplates any suitable combination of any suitable components, devices, or systems carrying out any suitable steps of the method of FIG. 15.
[0070] While the embodiments disclosed herein utilize a push-to-open, pull-to-close mechanism for opening and closing arms it should be understood that other suitable mechanisms can be used, such as a pull-to-open, push-to-close mechanism. A closure bias can be included, for example using a compliant mechanism such as a linear spring, helical spring, or leaf spring. Other actuation elements can be used for deployment of the gripper elements.
[0071] While the disclosed subject matter is described herein in terms of certain preferred embodiments for purpose of illustration and not limitation, those skilled in the art will recognize that various modifications and improvements can be made to the disclosed subject matter without departing from the scope thereof. Moreover, although individual features of one embodiment of the disclosed subject matter can be discussed herein or shown in the drawings of one embodiment and not in other embodiments, it should be readily apparent that individual features of one embodiment can be combined with one or more features of another embodiment or features from a plurality of embodiments.
[0072] In addition to the specific embodiments claimed below, the disclosed subject matter is also directed to other embodiments having any other possible combination of the dependent features claimed below and those disclosed above. As such, the particular features presented in the dependent claims and disclosed above can be combined with each other in other possible combinations. Thus, the foregoing description of specific embodiments of the disclosed subject matter has been presented for purposes of illustration and description. It is not intended to be exhaustive or to limit the disclosed subject matter to those embodiments disclosed.
[0073] It will be apparent to those skilled in the art that various modifications and variations can be made in the method and system of the disclosed subject matter without departing from the spirit or scope of the disclosed subject matter. Thus, it is intended that the disclosed subject matter include modifications and variations that are within the scope of the appended claims and their equivalents.
* * * * *
D00000
D00001
D00002
D00003
D00004
D00005
D00006
D00007
D00008
D00009
D00010
D00011
D00012

D00013
D00014

D00015

XML
uspto.report is an independent third-party trademark research tool that is not affiliated, endorsed, or sponsored by the United States Patent and Trademark Office (USPTO) or any other governmental organization. The information provided by uspto.report is based on publicly available data at the time of writing and is intended for informational purposes only.
While we strive to provide accurate and up-to-date information, we do not guarantee the accuracy, completeness, reliability, or suitability of the information displayed on this site. The use of this site is at your own risk. Any reliance you place on such information is therefore strictly at your own risk.
All official trademark data, including owner information, should be verified by visiting the official USPTO website at www.uspto.gov. This site is not intended to replace professional legal advice and should not be used as a substitute for consulting with a legal professional who is knowledgeable about trademark law.