Negative Pressure Wound Closure Device
Dunn; Raymond
U.S. patent application number 16/539801 was filed with the patent office on 2020-02-06 for negative pressure wound closure device. The applicant listed for this patent is University of Massachusetts. Invention is credited to Raymond Dunn.
| Application Number | 20200038023 16/539801 |
| Document ID | / |
| Family ID | 46603322 |
| Filed Date | 2020-02-06 |








View All Diagrams
| United States Patent Application | 20200038023 |
| Kind Code | A1 |
| Dunn; Raymond | February 6, 2020 |
NEGATIVE PRESSURE WOUND CLOSURE DEVICE
Abstract
The present invention relates to a negative pressure wound closure system and methods for using such a system. Preferred embodiments of the invention facilitate closure of the wound by preferentially contracting to provide for movement of the tissue. Preferred embodiments can utilize tissue grasping elements to apply a wound closing force to the tissue.
| Inventors: | Dunn; Raymond; (Shrewsbury, MA) | ||||||||||
| Applicant: |
|
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Family ID: | 46603322 | ||||||||||
| Appl. No.: | 16/539801 | ||||||||||
| Filed: | August 13, 2019 |
Related U.S. Patent Documents
| Application Number | Filing Date | Patent Number | ||
|---|---|---|---|---|
| 15083675 | Mar 29, 2016 | 10405861 | ||
| 16539801 | ||||
| 14581685 | Dec 23, 2014 | 9301742 | ||
| 15083675 | ||||
| 13365615 | Feb 3, 2012 | 9226737 | ||
| 14581685 | ||||
| 61439525 | Feb 4, 2011 | |||
| Current U.S. Class: | 1/1 |
| Current CPC Class: | A61M 1/0088 20130101; A61F 2013/00536 20130101; A61F 2013/0054 20130101; A61B 17/0057 20130101; A61F 13/00068 20130101; A61B 2017/081 20130101; A61F 2013/00174 20130101; A61M 1/008 20130101; A61B 2017/00654 20130101; A61B 17/08 20130101; A61F 2013/00548 20130101; A61F 2013/00544 20130101; A61B 2017/00561 20130101 |
| International Class: | A61B 17/08 20060101 A61B017/08; A61M 1/00 20060101 A61M001/00; A61B 17/00 20060101 A61B017/00; A61F 13/00 20060101 A61F013/00 |
Claims
1-75. (canceled)
76. A negative pressure wound closure device, comprising: a porous foam wound filler material that is sized and shaped to fit within a wound opening between wound margins,. wherein the porous foam wound filler material has a pore size and a pore density, and wherein the porous foam wound filler material is structured to preferentially contract along at least a first x-direction and inhibit contraction along a second y-direction upon application of a negative pressure to the wound opening to cause the wound margins to move along the first x-direction towards closure of the wound.
77. The negative pressure wound closure device of claim 76 further comprising a tissue grasping surface extending over an outer peripheral surface of the wound filler material and comprising a plurality of outward-projecting tissue anchors that contact tissue at a margin of the wound opening and displace the tissue at the wound margin upon application of the negative pressure to the wound filler material to facilitate closure of the wound.
78. The negative pressure wound closure device of claim 76, further comprising: a negative pressure source that is coupled to the porous foam wound filler material to apply a closure force to the wound opening; and a surface layer below the porous foam wound filler material that is configured to manage fluid within the wound and not to generate granulation.
79. The negative pressure wound closure device of claim 77, wherein the plurality of tissue anchors are integrally formed in the wound filler material.
80. The negative pressure wound closure device of claim 77, wherein the tissue grasping surface comprises a film that is provided over a surface of the wound filler material, the plurality of tissue anchors projecting outward from the film.
81. The negative pressure wound closure device of claim 80, wherein the film comprises a mesh material and includes a second plurality of inward facing anchors that secure the film to the wound filler material.
82. The negative pressure wound closure device of claim 76, wherein the wound filler material further comprises a stabilizing structure to enable collapse in at least the first x-direction and inhibit collapse in at least the second y-direction, the stabilizing structure including different regions in the porous foam wound filler material having different pore sizes or pore densities or a combination thereof.
83. The negative pressure wound closure device of claim 82, wherein the stabilizing structure comprises one or more regions of rigid material surrounded by regions of compressible material.
84. The negative pressure wound closure device of claim 82, wherein the wound filler material has length, width and height dimensions, and the stabilizing structure inhibits collapse in the height dimension.
85. The negative pressure wound closure device of claim 82, wherein the stabilizing structure compresses the wound filler material in at least the first x-direction to effect reapproximation of the wound.
86. The negative pressure wound closure device of claim 82, wherein the stabilizing structure substantially restricts the collapse of the wound filler material to a direction perpendicular to a plane defined by the wound margins.
87. The negative pressure wound closure device of claims 82, wherein the stabilizing structure comprises an endoskeleton made from rigid material.
88. The negative pressure wound closure device of claim 82 wherein the stabilizing structure comprises a plurality of connected articulating elements.
89. The negative pressure wound closure device of claim 76 wherein the porous foam wound filler material has an oval shape sized to fit within an abdominal wound opening and positioned over a surface layer such that the device contracts over the surface layer.
90. The negative pressure wound closure device of claim 89 wherein the surface layer comprises a porous material to manage fluid within the wound such that the porous foam wound filler material slides over the surface layer during contraction.
91. The negative pressure wound closure device of claim 76 wherein the porous foam wound filler material has regions of rigid material and regions of compressible material wherein the porous foam wound filler material has variable pore sizes and/or pore density.
92. The negative pressure wound closure device of claim 76 further comprising a plurality of stabilizer elements extending within the wound filler in a z-direction.
93. The negative pressure wound closure device of claim 92 wherein the plurality of stabilizer elements comprise ribs, flexures or rods.
94. The negative pressure wound closure device of claim 92 wherein the stabilizer elements comprise a rigid or semi-rigid material.
95. The negative pressure wound closure device of claim 92 wherein the stabilizer elements are separated by a flexible material.
96. The negative pressure wound closure device of claim 76 wherein the porous foam wound filler material comprises a smooth bottom surface that slides during contraction in the first x-direction.
97. The negative pressure wound closure device of claim 76 wherein the porous foam wound filler material has cleavage lines to provide for removal of one or more sections.
98. A method for treating a wound, comprising: placing into a wound opening a porous wound filler material that is sized and shaped to fit within the wound opening between wound margins, wherein the porous wound filler material has a pore size and a pore density; and applying a negative pressure to the wound opening to cause the porous wound filler material to preferentially contract-along at least a first x-direction and inhibit contraction along a second y-direction to cause the wound margins to move along the first x-direction towards closure of the wound.
99. The method of claim 98, wherein the placing of the porous wound filler material further comprises using a plurality of stabilizer elements extending within the wound filler material in a z-direction to inhibit contraction of the porous wound filler materials in the z-direction.
100. The method of claim 99, wherein the plurality of stabilizer elements comprise ribs, flexures or rods.
101. The method of claim 100, wherein the stabilizer elements comprise a rigid or semi-rigid material.
102. The method of claim 100, wherein the stabilizer elements are separated by a flexible material.
103. The method of claim 98, wherein the porous wound filler material comprises a smooth bottom surface that slides during contraction in the first x-direction.
104. The method of claim 98, wherein the porous wound filler has cleavage lines to provide removal of one or more sections.
105. The method of claim 98, wherein the porous wound filler material comprises a foam.
106. The method of claim 98, wherein the porous wound filler material comprises a mesh.
107. The method of claim 98, wherein the porous wound filler material further comprises a mesh that extends around an oval shaped structure that contracts in the first x-direction.
Description
CROSS REFERENCE TO RELATED APPLICATION
[0001] This application is a continuation of U.S. application Ser. No. 15/083,675 filed Mar. 29, 2016, now U.S. Pat. No. ______ , which is a continuation of application Ser. No. 14/581,685, filed on Dec. 23, 2014, now U.S. Pat. No. 9,301,742, which is a divisional of application Ser. No. 13/365,615, filed on Feb. 3, 2012, now U.S. Pat. No. 9,226,737 and also claims the priority to U.S. Application No. 61/439,525, filed Feb. 4, 2011. The entire contents of the above application being incorporated herein by reference.
BACKGROUND OF THE INVENTION
[0002] A number of techniques have been developed for treatment of wounds, including wounds resulting from accident and wounds resulting from surgery. Often, wounds are closed using sutures or staples. However, inserting these mechanical closure techniques requires making additional punctures or wounds to the skin, which can result in tissue injury and in the case of excess swelling, possible ischemia and tissue loss. Also, mechanical wound closures such as staples and sutures can cause highly-localized stresses at the insertion points that can impede and damage the normal wound healing processes of the skin.
[0003] In recent years, there has been increased interest in using negative pressure devices for the treatment of wounds. Negative pressure wound treatment utilizes devices that remove wound fluids by applying negative pressure suction to the wound. It is believed that such negative pressures promote wound healing by facilitating the formation of granulation tissue at the wound site and assisting the body's normal inflammatory process while simultaneously removing excess fluid, which may contain adverse cytokines bacteria. However, further improvements in negative pressure wound therapy are needed to fully realize the benefits of treatment.
SUMMARY OF THE INVENTION
[0004] The present invention relates to a negative pressure wound closure device that specifically exerts force at the edges of the wound to facilitate closure of the wound. The device operates to reduce the need for repetitive replacement of wound filler material currently employed and can advance the rate of healing. The device simultaneously uses negative pressure to remove wound fluids.
[0005] In one embodiment, a negative pressure wound closure device includes a wound filler material that is sized and shaped to fit within a wound opening and which contracts along at least one dimension upon application of a negative pressure to the filler material. The filler material is thus configured to preferentially contract in at least one direction and inhibit contractions in one or more additional directions. Prior negative pressure devices did not assist in wound closure, but were used to drain fluids. By providing for the controlled movement of tissue during the healing process in conjunction with the drainage of fluids from wounds as described in connection with the present invention, a substantial improvement in the rate of healing can be realized. Note that depending on the size of the wound, increased negative pressure can be used.
[0006] In another preferred embodiment, a tissue grasping surface extends over an outer peripheral surface of the wound filler material and includes a plurality of tissue anchors that engage the tissue at the wound margin. Upon application of negative pressure, the tissue at the wound margin is displaced to facilitate closure of the wound. A negative pressure source, such as a vacuum pump, is coupled to the wound filler material to provide the negative pressure.
[0007] The wound filler material generally comprises a porous material, such as a foam. For embodiments employing tissue anchors, these can be integrally formed in the filler material. In other embodiments, the tissue anchors are provided on a separate covering or film that is secured to the filler material.
[0008] In preferred embodiments, the filler material includes a stabilizing structure that enables the material to collapse in at least one first direction and inhibits collapse in at least one second direction. The stabilizing structure can include regions of relatively rigid material surrounded by regions of relatively compressible material. In preferred embodiments, the stabilizing structure is an endoskeleton formed of rigid and/or semi-rigid materials.
[0009] In certain embodiments, the stabilizing structure inhibits the filler material from collapsing along its height dimension, while enabling the filler material to collapse within the plane defined by the wound margins. This is useful in the case of abdominal surgery, for example, in which the surgical incision is along a straight line to form an oval shaped wound. This generally oval shaped wound can extend through muscle and fatty tissue having variable mechanical properties. Wound healing is better served through the use of an oval shaped structure adapted to preferentially collapse towards the original line of incision. In preferred embodiments, the stabilizing structure promotes collapse of the filler material in a manner to effect reapproximation of the wound tissue. Fasciotomy wounds, or other wound dehiscences, or any open wound can be successfully treated using embodiments of the present invention.
[0010] The wound closure device can be used to treat wounds in the mediastinum, for pressure ulcers, for wounds in the extremities (arms or legs) etc. The wound closure device can also be used to treat wounds of different shapes, such as circular, square, rectangular or irregularly shaped wounds. A plurality of wound closure elements can be shaped to fit within a wound and can attach together to preferentially close the wound in a desired direction. The different elements can comprise different materials or have different characteristics, such as pore size and/or anchor size and distribution to form a composite structure.
[0011] In one embodiment, an endoskeleton stabilizing structure includes a plurality of spaced-apart rigid members forming a cross-hatched configuration. The endoskeleton enables the filler material to collapse along its width dimension and elongate to a smaller degree along its length dimension. In certain embodiments, a plurality of rigid members extend along the height of the filler material and inhibit collapse of the material in its height dimension, for example. According to certain embodiments, the endoskeleton comprises a network of interconnected rigid members that can articulate with respect to one another during collapse of the filler material. The endoskeleton can include truss supports to inhibit tilting motion of the filler material. In some embodiments, the tissue anchors can be integrally formed in the endoskeleton.
[0012] In certain embodiments, the wound filler material includes a smooth bottom surface having micropores to allow the passage of fluid from the wound through the bottom surface and into the device for removal. The micropores can have variable pore size and/or pore density to direct the distribution of vacuum force from the negative pressure source. In some embodiments, the wound filler material can have variable internal pore sizes and/or pore density to direct the distribution of vacuum force.
[0013] In one embodiment, a negative pressure wound treatment component for managing and/or removing fluid is coupled to the wound filler material. A single negative pressure source can be used for wound closure and fluid management/drainage. A sliding surface is provided at the interface between the wound closure and fluid management components.
[0014] In yet another embodiment, the filler material includes removable portions to adjust the size of the wound closure device. The filler material can be provided with pre-determined cleavage lines for tearing or cutting away portions of the material. In certain embodiments, sets of tissue anchors are embedded in the filler material, and become exposed by removing excess portions of the material.
[0015] According to another embodiment, the tissue anchors are provided with a variable force profile. The force profile can vary based on the depth of tissue or the type of tissue engaged.
[0016] In some embodiments, the force profile of the tissue grasping surface varies around the perimeter of the wound closure device. The force profile is varied, for instance, by varying one or more of the length of the tissue anchors, the shape of the anchors, the materials of the anchors and the density of the anchors.
[0017] The present invention also relates to methods of closing a wound using a wound closure device as described above. For example, a linear incision in the skin overlying the abdomen provides access to a surgical site such as the gastrointestinal system of the human or animal body. Following completion, the wound must be treated by negative pressure therapy to facilitate recovery. Thus, a wound closure device in accordance with preferred embodiments of the invention is inserted for wound closure treatment.
[0018] By using the negative pressure wound closure device of the invention, patients with large or severe wounds are able to be discharged or engage in rehabilative physical therapy, changed at home and then brought back to have their wounds simply stitched closed. By improving wound closure treatment and thereby reducing cost, there is an opportunity for these devices to be a significant part of the instruments used for wound care.
BRIEF DESCRIPTION OF THE DRAWINGS
[0019] Other features and advantages of the present invention will be apparent from the following detailed description of the invention, taken in conjunction with the accompanying drawings of which:
[0020] FIG. 1A is a perspective schematic view of a negative pressure wound closure device.
[0021] FIG. 1B is a cross-section view of the tissue grasping surface of the wound closure device.
[0022] FIG. 1C is a side view of one embodiment of the tissue grasping surface.
[0023] FIG. 1D is a top view of the wound closure device showing x-y stabilizers in phantom.
[0024] FIG. 1E is a cross-section view of filler material showing x-y stabilizers and z-stabilizers.
[0025] FIG. 1F is a bottom view of the wound closure device showing a smooth bottom surface and micropores for removing fluid from the wound site.
[0026] FIG. 1G is an elevation view of a peripheral stabilizer element.
[0027] FIGS. 2A and 2B are perspective and side views, respectively, of a supporting endoskeleton.
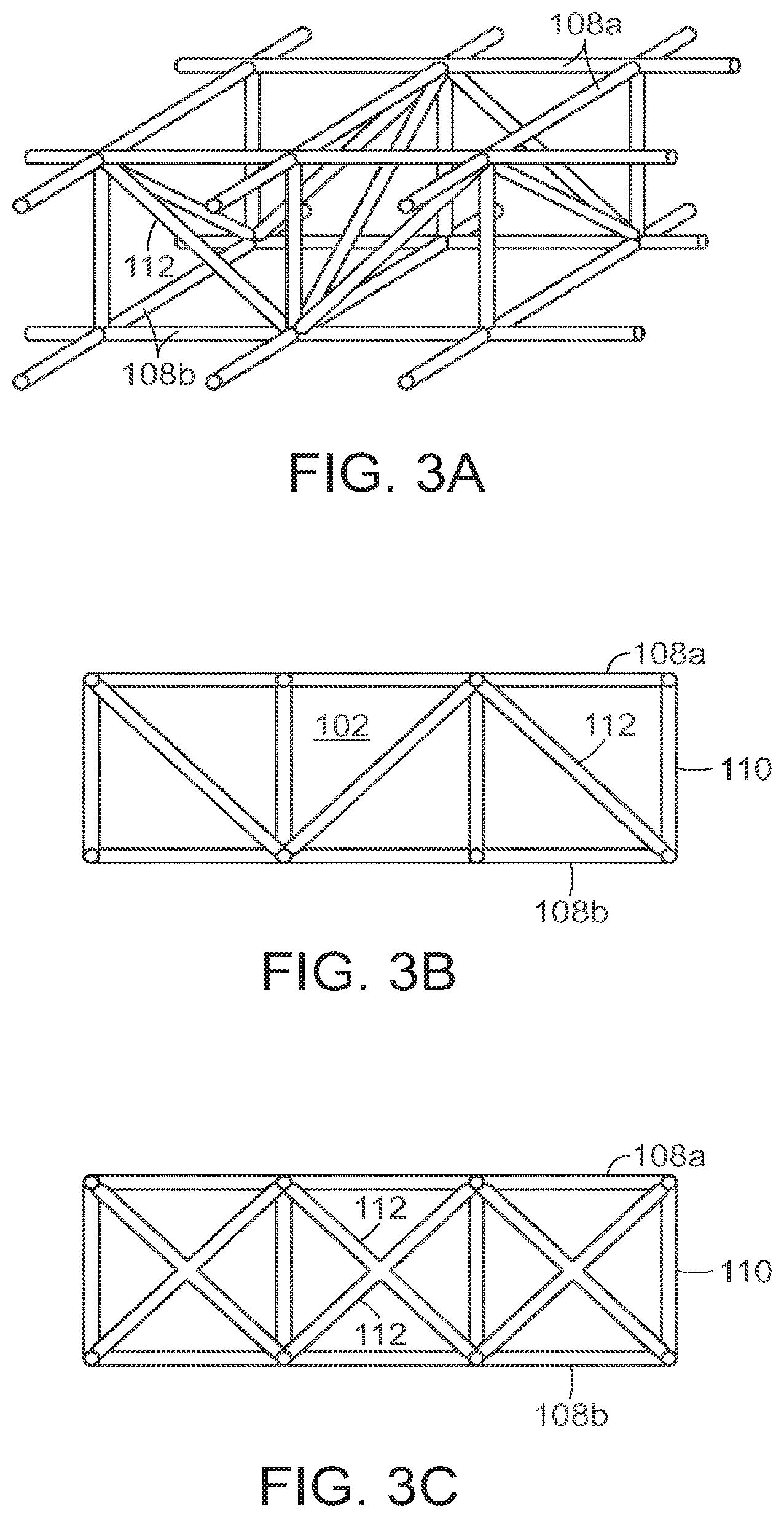
[0028] FIGS. 3A and 3B are perspective and side views, respectively, of a supporting endoskeleton with support trusses.
[0029] FIG. 3C is a side view of a supporting endoskeleton with x-shaped support trusses.
[0030] FIGS. 4A-C illustrate a wound closure device of the invention closing a wound.
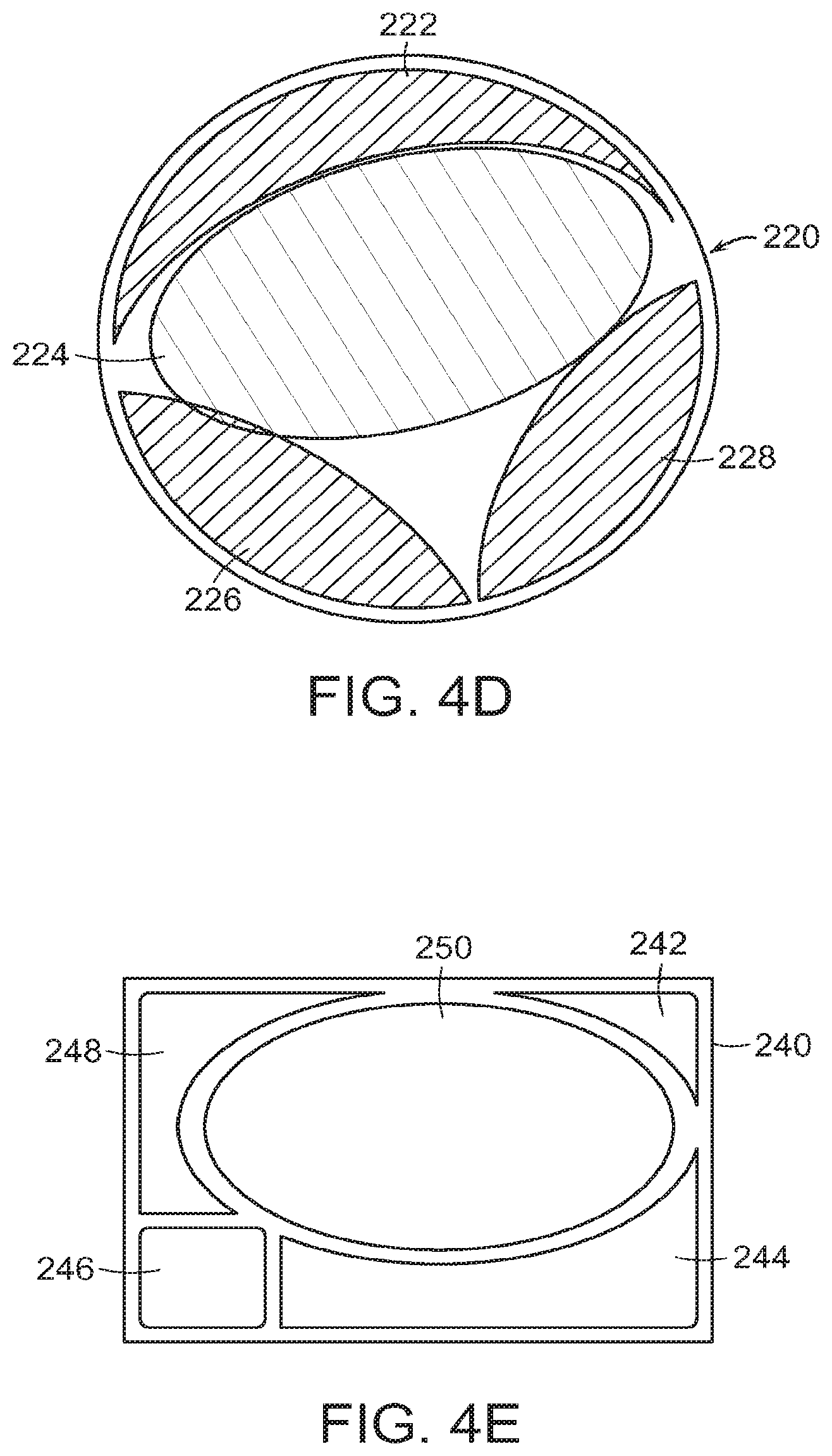
[0031] FIGS. 4D-4E illustrate the use of a plurality of wound closure elements used for wounds of different shapes.
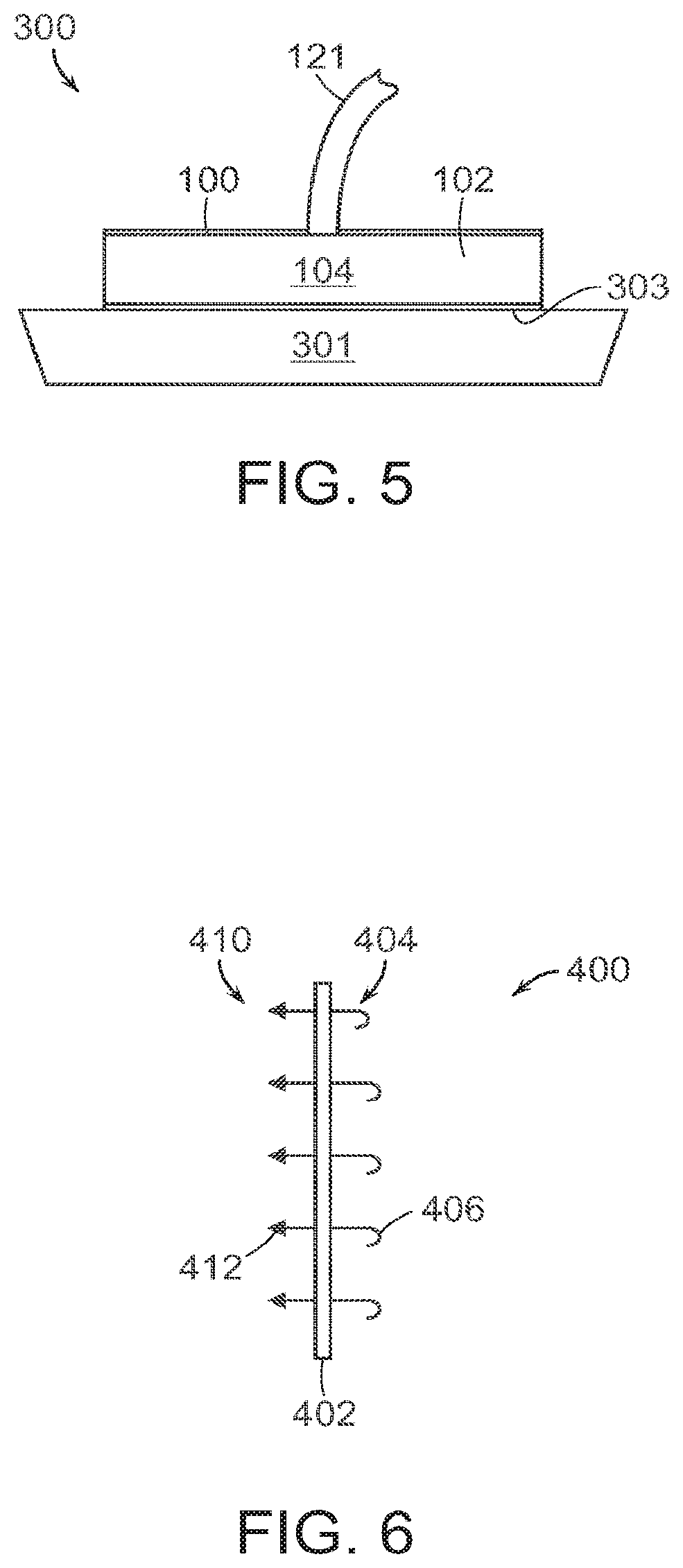
[0032] FIG. 5 illustrates a two-stage negative pressure wound treatment and negative pressure wound closure (NPWT/NPWC) device.
[0033] FIG. 6 illustrates an enlarged view of a preferred embodiment of the tissue anchor system in accordance with the invention.
[0034] FIG. 7 illustrates an embodiment of a wound filler material having a tear-away or cut-away design for accommodating different wound sizes, with tissue anchors embedded within the filler material at pre-determined cleavage points.
[0035] FIG. 8A is a side view of a tissue grasping surface, illustrating different tissue anchors for different types of tissue (T.sub.1, T.sub.2) and the respective force profiles for the anchors, including the maximum force applied during vacuum closure (F.sub.1) and the force required to remove the anchors from the tissue (F.sub.2) without damaging the tissue.
[0036] FIG. 8B illustrates different designs for a tissue anchor of the invention.
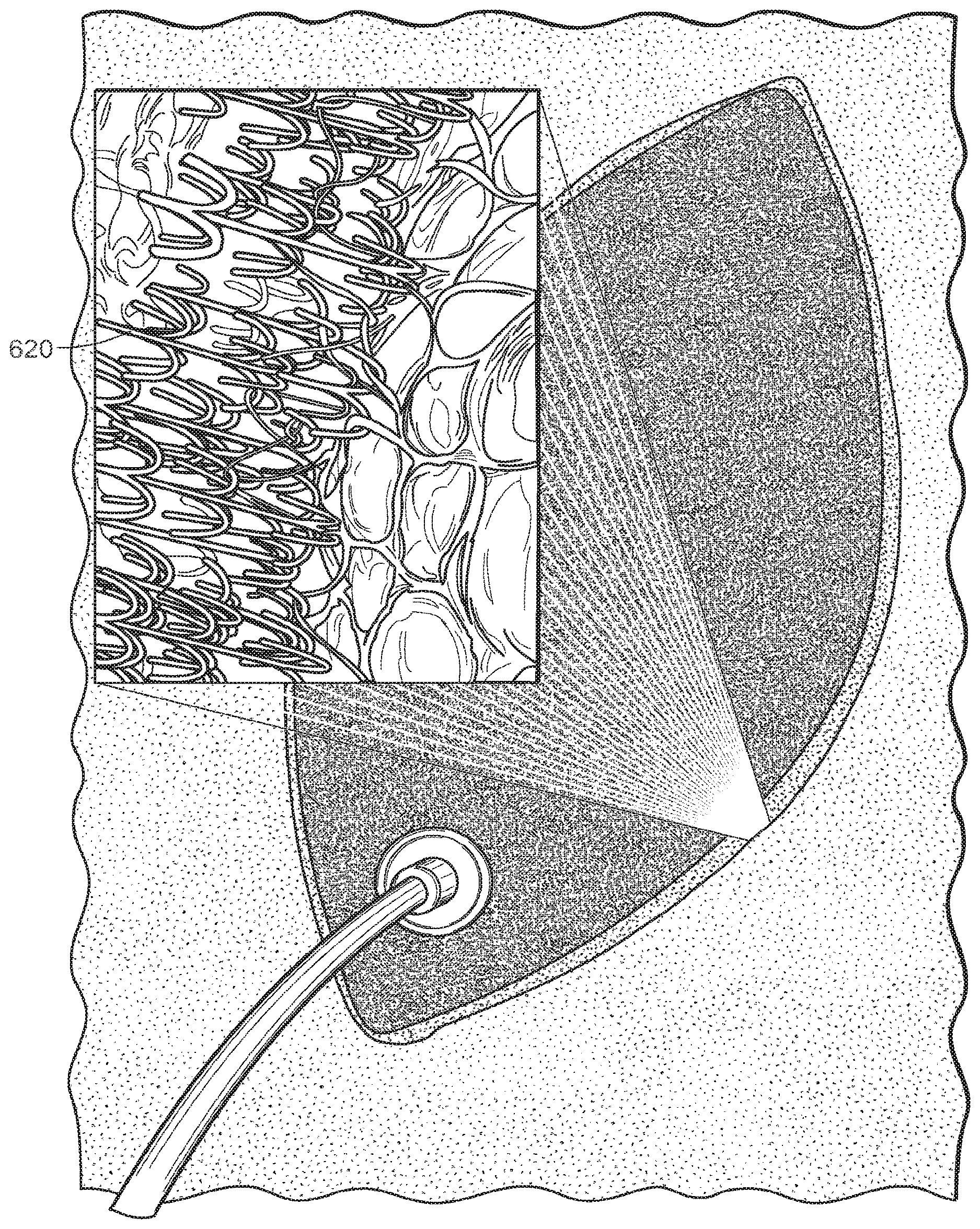
[0037] FIG. 8C illustrates an enlarged view of tissue anchor elements on the peripheral surface of an oval shaped wound closure device.
[0038] FIG. 9A is a schematic illustration of a wound closure device positioned within a wound showing the different force profile around the margin of the wound according to one embodiment.
[0039] FIG. 9B illustrates the wound closure device of FIG. 9A after a period of wound closure and healing, with the original configuration of the wound and wound closure device indicated in phantom.
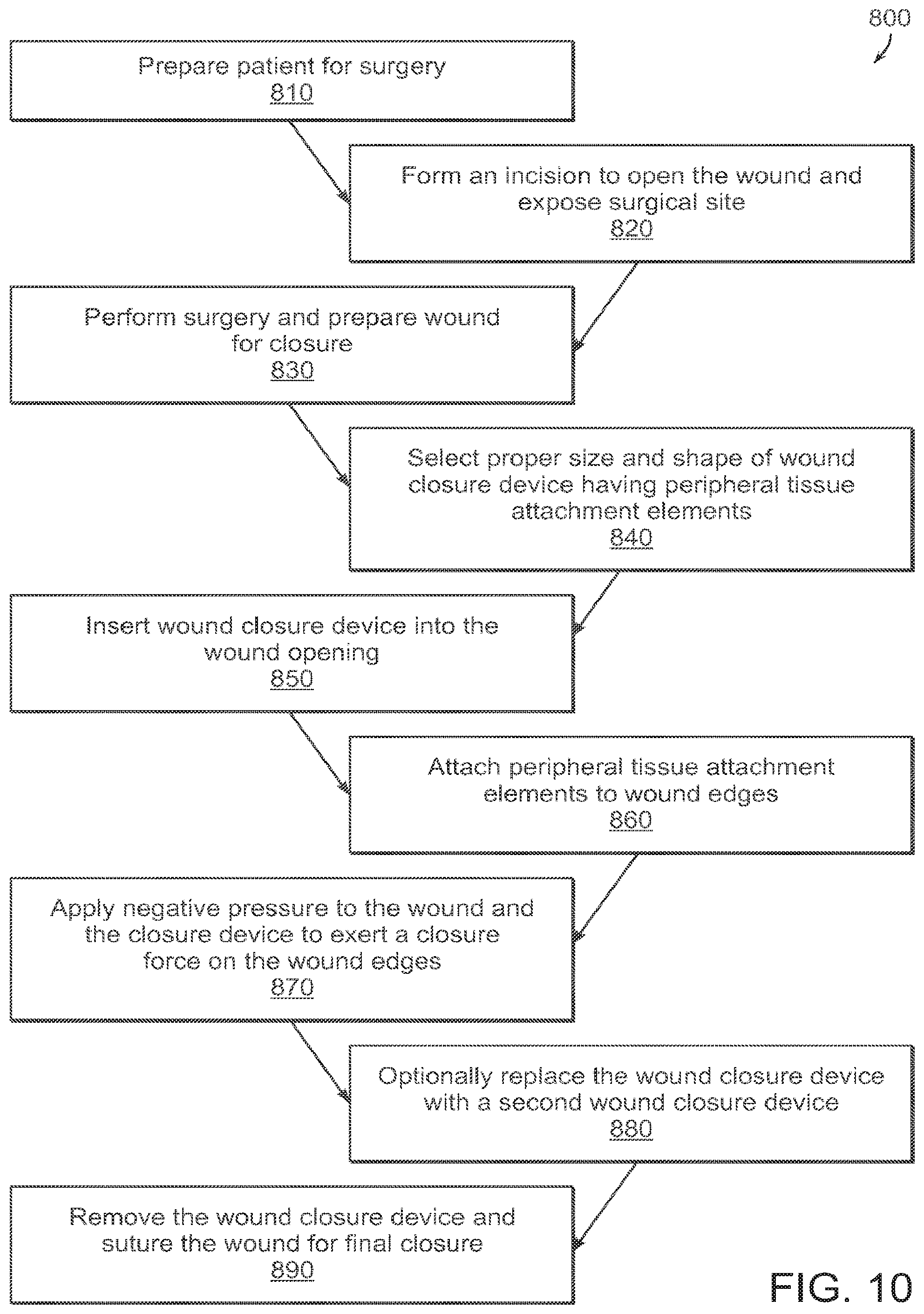
[0040] FIG. 10 schematically illustrates a process of using a wound closure device in accordance with the invention.
DETAILED DESCRIPTION OF THE INVENTION
[0041] FIGS. 1A-1F illustrate an embodiment of a wound closure device 100 of the present invention. The device 100 includes a wound filler material 102 that is sized and shaped to fit within a wound opening of a human or animal patient. In preferred embodiments, the filler material 102 is a porous, biocompatible material, such as an open cell polyurethane foam. The filler material 102 is also preferentially collapsible, meaning that its size can be reduced along at least one dimension (e.g., length, width, height) by applying a negative pressure to the filler material 102, while at the same time inhibiting contractions or contracting at a slower rate in another direction.
[0042] Extending over at least one surface of the filler material 102, and preferably extending over an outer perimeter surface of the filler material 102 is a tissue grasping surface 104. In one embodiment, the tissue grasping surface 104 is a flexible covering, such as a mesh film, that is secured to the outer perimeter surface of the filler material 102 and can expand and contract with the expansion and contraction of the filler material 102. In one embodiment, the tissue grasping surface 102 is a mesh film or a composite polyester mesh film, such as the Parietex.TM. mesh from Covidien (Mansfield, MA). The tissue grasping surface 104 includes a plurality of outward-facing tissue anchor elements 106, which in the preferred embodiment are a plurality of closely-spaced barbs, hooks or tissue grasping elements, which can be integrally formed in the mesh film.
[0043] FIG. 1B is an edge view of the device 100 showing the tissue grasping elements 106 projecting from the tissue grasping surface 104 on the periphery of the wound filler material 102. FIG. 1C is a side view of one embodiment, in which the tissue grasping surface 104 is formed from a flexible material, in particular, a mesh material. The grasping elements 106 project out from the page in FIG. 1C. The flexible, mesh material of the tissue grasping surface 104 allows the surface to expand and contract as necessary with the expansion and contraction of the underlying wound filler material 102.
[0044] In other embodiments, the tissue grasping surface 104 with anchor elements 106 can be integrally formed in the filler material 102. The tissue grasping surface and/or anchor elements can also be formed using a resorbable material.
[0045] The tissue anchor elements 106 are preferably provided over an entire outer perimeter surface of the filler material 102. When the filler material 102 is placed within a wound, the anchor elements 106 become buried within the tissue at the wound margins and secure the device 100 within the wound opening. The tissue anchor elements 106 are preferably spread out over the entire surface of the wound margin to provide sufficient strength in the grasping force. The tissue grasping surface 104 is preferably designed to allow the wound closure device 100 to be easily placed but also easily removed and replaced with a new device 100 or other wound dressing as needed (e.g., 2-7 days later). The grasping surface 104 can be configured to have high grasping strength over at least a portion of its surface, but easily removable by, for example, pulling away at an edge. The tissue grasping surface 104 is preferably designed to be removed from a wound without damaging the surrounding tissue. The anchor elements 106 are preferably designed to accommodate various tissue applications, such as muscle, fat, skin and collagen, and various combinations of these. The anchor elements 106 can also be designed to remain securely attached to particular tissues for a selected time period in certain embodiments.
[0046] In embodiments in which the grasping surface 104 is formed from a covering on the outer peripheral surface of the filler material 102, the grasping surface can be attached to the filler material 102 using any suitable technique, such as with an adhesive or a mechanical fastening system. In a preferred embodiment, the tissue grasping surface 104 includes filler-grasping anchor elements, which can be barbs, that secure the grasping surface to the filler material. As shown in the cross-section view of FIG. 6, for example, the grasping surface 400 comprises a thin mesh or film having two sets of barbs or similar anchor elements, a first set 410 of outwardly-facing tissue-grasping elements 412 that are designed to project into tissue, and a second set 404 of elements 406 that project into the filler material to secure the grasping surface to the filler material.
[0047] Returning to FIGS. 1A-1F, a negative pressure source 120, such as a pump, is coupled to the filler material 102 by a suitable coupling or conduit, such as tube 121. Additional tubes 107 can also be connected through an array of spaced ports 105 in order to spatially distribute the suction force so that the force exerted along the sidewall 104 can be controlled separately from a fluid suction force. The negative pressure source 120 can be activated to apply a negative pressure to the filler material 102. In general, the negative pressure causes a resulting pressure differential which causes the filler material 102 to contract or "collapse." As the filler material 102 contracts, the tissue grasping surface 104 grabs and pulls on the adjacent tissue, which is preferably the tissue around a wound margin, resulting in the displacement of the tissue thereby facilitating the closure of the wound. In a preferred embodiment, the filler material 102 is designed to collapse preferentially in at least one direction. For example, in the embodiment of FIG. 1A, the filler material 102 includes a length and width dimension along the y- and x-axes, respectively, and a height along the z-axis. In order to efficiently transmit the negative pressure to the subcutaneous or other wound margins, it is preferred that the filler material 102 does not collapse centrally in the z-direction (like a pancake), so that the action of the negative pressure works predominantly in the x-y directions, or more particularly, in a two-dimensional plane along the wound margins such as in an open abdomen or fasciotomy. It will be understood that in some embodiments, the plane of the wound margins can be curved, such as when the wound goes around the curve of an abdomen or leg.
[0048] Furthermore, in preferred embodiments the filler material 102 is configured to preferentially collapse in length and/or width (i.e., along the x- and y-axes) to reapproximate the tissue at the wound margins. Note that certain types of wounds can be treated without the anchor elements described herein.
[0049] There are several ways in which the filler material 102 is configured to exhibit preferential collapse characteristics. For example, portions of the filler material 102 can be made from more rigid material than the surrounding material, causing the filler material to preferentially collapse in a particular direction. In one embodiment, the filler material 102 can include a stabilizing endoskeleton made from a suitable rigid material embedded within a "collapsible" filler, such as an open cell foam. Note that the amount of applied negative pressure can be adjustable depending on the size and shape of the wound. Pressures above 125 mm, to as much as 250 mm or more can be used to assist in wound closure. The pressure can be reduced over time as the wound contracts.
[0050] As shown in FIGS. 1D and 1E, for example, the filler material 102 includes a plurality of stabilizer elements 108 (shown in phantom) that enable the collapse of the filler material in certain directions, while inhibiting it in other directions. In this embodiment, the stabilizer elements 108 include a plurality of stabilizing ribs, flexures or rods, made from a suitably rigid or semi-rigid material, such as plastic. The ribbed structure is configured to preferentially collapse along a specific axis to facilitate proper closure of the wound. The internal stabilizer elements 108 in this embodiment form a cross-hatched pattern as seen in FIG. 1D, though it will be understood that other configurations can be utilized. The spacing between the elements in the "open" state can be in a range of 1-2 cm, for example. The stabilizer elements 108 can be provided at different depths within the filler material, as shown in the cross-section view of FIG. 1E, which helps inhibit collapse in the z-direction. In some embodiments, z-axis stabilizer elements 110 can be utilized to inhibit collapse in this direction. In FIG. 1E, the z-axis stabilizer elements 110 are projections that extend vertically from the ribs 108. In other embodiments, separate z-axis stabilizers, such as rods or rib structures, can be employed.
[0051] In certain embodiments, the device 100 can include a peripheral stabilizer element 111 that extends around the outer periphery of the filler material 102, as shown in FIG. 1E. The stabilizer element 111 can include a rib structure that reinforces the filler material 102 in order to prevent collapse in the z-direction, as well as to inhibit tilting of the filler material in the z-y and z-x planes. Thus, preferred embodiments of the filler material preferentially contract in at least a first direction relative to a second direction upon application of a negative pressure. Thus, for example, the width will contract at a faster rate relative to the length, while the height (depth of the wound) does not contract a substantial distance.
[0052] In some embodiments, the tissue grasping anchor elements 106 can be included on the peripheral stabilizer element 111, and project out from the periphery of the filler material 102. This can be as an alterative to, or in addition to, providing the anchor elements 106 on a separate mesh or film. The peripheral stabilizer element 111 is preferably configured to expand and contract as necessary with the expansion and contraction of the wound filler material 102. Thus, in a preferred embodiment, the stabilizer element 111 has sufficient flexibility to contract and expand in the x- and y-directions (i.e., around the periphery of the filler material 102), but has adequate rigidity along the z-direction (i.e. along the height of the filler) to inhibit collapse or tilting in this direction.
[0053] An embodiment of a peripheral stabilizer element 111 is shown in elevation view in FIG. 1G. The stabilizer element 111 includes a plurality of stabilizing rods 113, oriented to inhibit collapse in the z-direction. The rods 113 are separated by a flexible material 114 that allows the stabilizer element 111 to expand and contract around the wound margin with the expansion and contraction of the underlying filler material. In this embodiment, the tissue anchor elements 106 are formed in the peripheral stabilizer element 111 and project out from the page.
[0054] One embodiment of an endoskeleton for a wound filler material of the invention is shown in FIGS. 2A and 2B. The endoskeleton includes a first set of x-y stabilizer elements 108a and a second set of x-y stabilizer elements 108b that are connected by a plurality of z-axis stabilizer elements 110.
[0055] During collapse of the filler material 102, the respective x-y stabilizer elements 108a, 108b are collapsible in the x-y directions, but the z-axis stabilizer elements 110 inhibit collapse in the z-direction. In preferred embodiments, the stabilizer elements can articulate with respect to one another during collapse. The joints 109 in the structure can be hinged or have a reduced thickness to accommodate the flexing of the system. The flexures between the joints may also flex to accommodate the desired compression along the first, or lateral, axis 117 (see FIG. 4B). Some expansion can occur along the second, or longitudinal, axis 119 as the device compresses. The frame material can have a shape memory characteristic, which in combination with the suction force, 25 defines the force level applied to the tissue.
[0056] In another embodiment, shown in FIGS. 3A and 3B, the endoskeleton includes truss stabilizers 112 to inhibit tilting of the filler material 102 during collapse. The truss stabilizers 112 keep the upper 108a and lower 108b x-y stabilizers aligned with one another as the filler material 102 collapses. In some embodiments, the truss stabilizers 112 can be rigid in certain directions and relatively less rigid in other directions (for example, the truss stabilizer can be bowed) to promote collapse in certain directions. FIG. 3C illustrates an alternative embodiment having truss stabilizers 112 in an "x"-shaped pattern.
[0057] The stabilizing endoskeleton in certain embodiments can be made, in whole or in part, from a shape memory material. Various shape memory materials can be used which return from a deformed state (temporary shape) to their original (permanent) shape. This change in shape can be induced by an external stimulus or trigger.
[0058] In one embodiment, the original or "permanent" shape of the endoskeleton is the "collapsed" configuration of the wound closure device, or the shape that will bring about wound reapproximation. When the wound closure device is initially inserted in the wound opening, the endoskeleton is in a deformed or temporary state and embedded within the filler material. The endoskeleton can preferentially revert to its original or "collapsed" state or, alternatively, cause the device to expand to engage the tissue. The "collapse" force of the shape memory endoskeleton can be in addition to or an alternative to the vacuum force induced by the negative pressure source. In certain embodiments, the application of a negative pressure to the wound closure device, which can cause the endoskeleton to revert to its original state.
[0059] FIG. 1F shows the bottom of the wound closure device 100 according to one embodiment. The device 100 in this embodiment includes a smooth bottom surface 115. This material can be biocompatible film to be used with, such as, provided in conjunction with the Renasys.RTM. system available from Smith & Nephew. A preferred embodiment can also be used with a gauge as also provided in the Renasys.RTM. system. The bottom surface 115 provides a low-friction interface between the wound closure device 100 and the underlying tissue. In the case of an abdominal wound, for example, the underlying tissue can include internal organs, such as the intestines. The smooth bottom surface 115 enables the filler material 102 to contract and expand freely without interference from the underlying tissue, and without damaging the underlying tissue. In a preferred embodiment, the bottom surface 115 includes micropores 116 (shown with size exaggerated in FIG. 1F for purposes of illustration) that allow the passage of fluid through the bottom surface 115 and into the device 100 for removal from the wound site. The wound closure device can also be inserted over a separate layer of material so that the device with contract on top of the sliding layer.
[0060] In some embodiments, the micropores 116 can have different sizes in different regions and/or can have different pore densities in different regions in order to direct different force levels of the vacuum source to different regions of the device 100. Similarly, the filler material 102 can be engineered with different internal pore sizes and/or pore densities to direct the distribution of forces from the vacuum source to different areas of the device 100.
[0061] FIGS. 4A-4C illustrate the use of the present device 100 to close a wound 200. The wound 200 includes a wound opening 201 and a wound margin 203, as shown in FIG. 4A. In FIG. 4B, a wound closure device 100 is placed within the wound opening 201 so that the tissue grasping surface 104 is contacting the wound margin 203. In certain embodiments, the wound closure device 100 can be formed by trimming or tearing the filler material 102 to the proper size, and then attaching the tissue grasping elements 106 around the periphery of the filler material 102. In one embodiment, the grasping elements 106 are attached by attaching a two-sided barbed mesh to the filler material 102, where the outward-facing prongs are designed for grasping tissue and the inward-facing prongs are designed to secure the mesh to the filler material 102. A tube 121 connects the filler material 102 to the negative pressure source. The area of the wound 200, including the filler material 102, can be covered by a sealing drape 205.
[0062] In the embodiment of FIG. 4B, the filler material 102 includes a plurality of internal stabilizer elements 108 (shown in phantom) that provide the filler material 102 with a preferential collapse characteristic. The stabilizer elements 108 help control the collapse of the filler material 102, and the resulting displacement of the tissue around the wound margin 203, in the x- and y-directions. Additional stabilizer elements can be provided to control or inhibit collapse along the z-direction. As described above in connection with FIGS. 1D, the stabilizer elements 108 in this embodiment include a crosshatched configuration.
[0063] FIG. 4C illustrates the wound 200 following the application of a negative pressure to the wound closure device 100. The tissue anchor elements 106 grab the tissue margins 203 and cause displacement of the tissue margins 203 as the filler material 102 collapses. As seen in the FIG. 4C, the filler material 102 collapses in the x- and y-directions in such a manner as to reapproximate the tissue at the wound margin 203. In the embodiment of FIG. 4B and 4C, the crosshatched configuration of the stabilizer elements 108 help control the direction of tissue displacement during collapse. The largest amount of tissue displacement in this embodiment is in the central region of the wound 200, where the opening 201 is widest, and this displacement is primarily inward along the x-direction. Away from the central region (e.g., at the top and bottom of the wound as shown in FIGS. 4A and 4B), where the wound margins are closer together, less displacement in the x-direction is needed to reapproximate the tissue. In general, the inward collapse of the filler material along the y-direction is undesirable. In fact, during tissue reapproximation, the wound 200 will tend to elongate in y-direction as the wound margins close in the x-direction. In preferred embodiments, the internal stabilizer elements 108 promote the collapse of the filler material in a manner that provides wound reapproximation. In the embodiment of FIGS. 4-C, for example, during filler collapse the crosshatched stabilizer elements 108 straighten out relative to one another, similar to an accordion gate. The largest displacement is in the central region of the filler 102, along the x-direction. The stabilizers 102 generally inhibit inward collapse along the y-direction. As the stabilizers 108 straighten out, they can also facilitate elongation of the wound in the y-direction to allow proper tissue reapproximation. Shown in FIGS. 4D-4E are different shaped wounds 220, 240 in which a plurality of wound closure elements are used in combination to fill the wound. In FIG. 4D, elements 222, 224, 226 and 228 have different shapes that are cut or trimmed to size so as to substantially fill the wound that in this example, is circular in shape. When negative pressure is applied, the elements work together to close the wound in a desired direction. FIG. 4E illustrates a rectangular wound 240 using closure elements 242, 244, 246, 248 and 250 to fill the wound 240. The tissue anchors of each closure element can also attach to the adjoining closure element(s). With suction applied to the central elements 224, 250, the adjoining elements are drawn towards the central elements to close the wound.
[0064] The wound closure device 200 can remain in this configuration for a period of several days or weeks to facilitate closing and healing of the wound 200. After a period of healing, the device 100 can be removed and optionally replaced with a smaller device. After the wound has been sufficiently closed using the present device, it can be stitched closed.
[0065] FIG. 5 illustrates a two-stage negative pressure wound treatment and negative pressure wound closure (NPWT/NPWC) device 300. The device includes a negative pressure drainage/fluid management component 301, as is known in the art, that connects with an overlying negative pressure wound closure device 100. The wound closure device 100 includes a collapsible wound filler material 102 and a tissue grasping surface 104, substantially as described above. A tube 121 connects the device 300 to a single pump for applying a negative pressure to the wound closure and wound treatment components. The device 300 can include interchangeable parts depending on the need of a specific wound application. In one embodiment, the device 300 is used for abdominal wounds, and can also be used for mediastinum and fasciotomy wounds.
[0066] In a preferred embodiment, the filler material 102 is able to "slide" within the total NPWT/NPWC device 300. The filler material 102 includes a sliding surface 303 at the interface between the wound closure and fluid management components. The sliding surface can comprise a treated surface or a separate layer of material. The sliding surface 303 facilitates the free contraction of the wound closure component, without interference from the fluid management component. The underlying fluid management component 301 can be specifically configured to manage fluid only and to not generate granulation, as this can slow down or inhibit the "slide."
[0067] FIG. 6 illustrates an enlarged view of a preferred embodiment of the tissue anchor system 400 in accordance with the invention. One side of the material 402 has a first group of anchor elements 404 that are adapted to grasp the filler material. The first anchor elements 404 can be shaped to grasp the filter material such as with a distal hooked shape 406. As material 402 must attach to the filter with a certain grasping strength in order to apply a sufficient pulling force on the tissue, a specified force level F, must be applied to remove the hooks from the filler material that exceeds the pulling force being applied to the tissue. Similarly, as the tissue to be grasped by the material 402 has different structural characteristics then the filler material, a second group of anchor elements 410 adapted to grasp tissue can have a different shape and grasping force then the first anchor elements. In this embodiment, barbs 412 will bilateral prongs 414 that tend to collapse upon insertion in tissue and yet expand when pulled in an opposite direction such that a certain pulling force can be applied to tissue. However, the prongs or cone shape anchor element has a release force such that the barbs can be manually pulled from the tissue without causing injury.
[0068] FIG. 7 illustrates an embodiment a wound filler material 500 having a tear-away or cut-away design for accommodating different wound sizes. The filler material 500 includes natural cleavage lines 501, 503, 505 that allow the size of the material to be adjusted to fit the wound to be closed. The material 500 is designed to be torn or cut at the cleavage lines to remove one or more portions 502a, 502b, 502c of the material and adjust the size of the material. Sets of tissue anchors 506a, 506b, 506c, 506d are embedded within the filler material at pre-determined cleavage points, and become exposed as the respective outer portions 502a, 502b, 502c are removed. The tissue anchors 506a, 506b, 506c, 506d can be associated with a stabilizing endoskeleton structure, such as described above in connection with FIGS. 1-4. In some embodiments, the stabilizing endoskeleton structure can include pre-defined cleavage points to remove portions of the stabilizer structure as the size of the filler material 500 is adjusted.
[0069] FIG. 8A is a side view of a tissue grasping surface, illustrating different tissue anchors 601, 602, 603, 604 for different types of tissue (T.sub.1, T.sub.2). Also illustrated is an example of the respective force profiles for the anchors, including the maximum force applied to the tissue during vacuum closure (F.sub.1) and the force required to remove the anchors from the tissue (F.sub.2) without damaging the tissue. In one embodiment, the characteristics of the tissue anchors vary to provide different force profiles across the interface between the wound closure device and the surrounding tissue. For example, for the upper tissue layer(s), T.sub.1, the anchor 601 is designed to attach to collagen material, such as in the dermis. The anchor 601 has a different force profile (F.sub.1 and F.sub.2) on the upper tissue layer(s), T.sub.1, as shown in FIG. 8A. At the lower tissue layers T.sub.2, the anchors 602, 603, 604 are designed to attach to fatty tissue of subcutaneous layer. Generally, a smaller force profile is needed to secure the anchors to this tissue.
[0070] The characteristics of the anchors, and their resulting force profiles, can vary by a number of parameters, such as the length of the anchor, the shape of the anchor, the structure of grasping features, the material(s) used for the anchor, the relative flexibility/rigidity of the anchors, and the spacing/density of the anchors. In FIG. 8A for example, anchor 601 is significantly longer than anchors 602, 603, which in turn are longer than anchors 604. FIG. 8A also illustrates varying the density of anchors, such as shown in 602, 603 and 604. FIG. 8B illustrates three examples of different types of grasping features, including a barbed configuration 605, a staggered hook configuration 606, and a staggered barbed configuration 607. Other suitable grasping features can be utilized such as the anchor elements 620 shown in the enlarged perspective view of FIG. 8C. The anchoring process can be augmented by suturing the filler material or supporting endoskeleton to the tissue. The force profile can also be varied by controlling the vacuum force distribution in the filler material, such as by varying the pore size and/or pore density of the filler.
[0071] The wound closure device of the invention can be provided in kits for closing different types of wounds (e.g., abdominal, fasciotomy, etc.). The tissue grasping surface can be optimized for different types of tissue such as collagen, fatty tissue and muscle, depending on the structure of the tissue at the wound site.
[0072] In certain embodiments, the force profile of the wound closure device is variable around the periphery of the wound. An exemplary embodiment is illustrated in FIG. 9A, which shows the force profile (f.sub.1) exerted on the wound margins at a plurality of locations on the periphery of the wound. In this embodiment, the largest f.sub.1 is at the central region of the wound filler 102, where the wound opening is widest and the wound closure force is entirely or nearly entirely in the x-direction. Moving towards the top and bottom regions of the wound, the closure force (f.sub.1) is much smaller. One reason for this is because the wound opening is much smaller in these regions, and a much smaller force is needed to reapproximate the tissue. Also, the inward force exerted in these regions includes components in both the x- and y-directions. Thus, a smaller force profile is preferable to avoid the inward collapse of the tissue in the y-direction. As illustrated in FIG. 9B, as the wound closes and heals from an initial state (indicated by dotted lines) to a later state (indicated by solid lines), it becomes elongated in the y-direction. Thus, the displacement of tissue anchors 701a and 701b is exclusively in the x-direction and in the direction of the closure force (f.sub.1), while the displacement of tissue anchors 703a, 703b is both inwards in the x-direction (in the direction of the closure force) and outwards in the y-direction (opposite the direction of the closure force). Thus, a smaller f.sub.1 is preferable in these regions to provide more "play" between the anchor elements and the surrounding tissue. Alternatively, the wound closure device is configured so that it does not elongate, but rather does not change its length along the long axis 720.
[0073] The variation in the force profile around the periphery of the wound closure device can be achieved in a variety of ways, such as varying the spacing/density of the tissue anchors, the types of anchors, length of anchors, etc. For example, in FIGS. 9A and 9B, anchors 701a, 701b are longer and penetrate deeper into the tissue compared to anchors 703a, 703b. The force profile can also be varied by controlling the vacuum force distribution in the filler material, such as by varying the pore size and/or pore density of the filler.
[0074] On one embodiment, a method of fabricating a wound closure device of the invention includes forming a stabilizing endoskeleton of rigid or semi-rigid material and forming a collapsible filler material over the endoskeleton. The stabilizing endoskeleton can be formed using a molding process, and can be molded as an integral unit or in one or more components that are then assembled to form the endoskeleton. Different components of the endoskeleton can have different thicknesses and/or degrees of rigidity to provide varying levels of rigidity and flexibility along different directions. The endoskeleton can be assembled by joining components, such as by using a suitable adhesive or other joining process. In certain embodiments, at least some of the components can be assembled to provide articulating joints. In preferred embodiments, the filler material is formed by mixing together appropriate metered amounts of constituent substances, (e.g., isocyanates, polyols, catalysts, surfactants, blowing agents and the like in the case of polyurethane foam), dispensing the reacting mixture into a mold, and then curing and demolding the material. Optionally, the material can then be cut or trimmed to the finished shape. In preferred embodiments, the endoskeleton support structure is assembled and placed into the mold, and the filler material is molded around the endoskeleton. An example of a biodegradable foam product suitable for the present wound closure device, and methods of fabricating such a foam, is described in U.S. Published Application No. 2009/0093550 to Rolfes et al., the entire contents of which are incorporated herein by reference.
[0075] A method of performing a surgical procedure 800 using a wound closure device in accordance with preferred embodiments of the invention as illustrated in FIG. 10. After preparation 800 of the patient for surgery, an incision is made 820 to expose the surgical site, typically in the abdomen. After the procedure is performed, the wound is prepared 830 for closure. The proper size and shape of the wound closure device is selected 840 with the peripheral tissue attachment members positioned around the circumference or outer wall surface of the device. The device is inserted 850 into the wound and the tissue attachment elements are inserted 860 into the tissue. Negative pressure is then applied 870 to exert a closure force on the wound edges. Depending on the particular application, large wounds may require placement 880 of a smaller second closure after removal of the first larger device. Finally, the device is removed 890 and the wound is closed, typically by suturing.
[0076] While the invention has been described in connection with specific methods and apparatus, those skilled in the art will recognize other equivalents to the specific embodiments herein. It is to be understood that the description is by way of example and not as a limitation to the scope of the invention and these equivalents are intended to be encompassed by the claims set forth below.
* * * * *
D00000
D00001
D00002
D00003
D00004
D00005
D00006
D00007
D00008
D00009
D00010
D00011
D00012

D00013
XML
uspto.report is an independent third-party trademark research tool that is not affiliated, endorsed, or sponsored by the United States Patent and Trademark Office (USPTO) or any other governmental organization. The information provided by uspto.report is based on publicly available data at the time of writing and is intended for informational purposes only.
While we strive to provide accurate and up-to-date information, we do not guarantee the accuracy, completeness, reliability, or suitability of the information displayed on this site. The use of this site is at your own risk. Any reliance you place on such information is therefore strictly at your own risk.
All official trademark data, including owner information, should be verified by visiting the official USPTO website at www.uspto.gov. This site is not intended to replace professional legal advice and should not be used as a substitute for consulting with a legal professional who is knowledgeable about trademark law.