Compositions And Methods For Treating Myelofibrosis
Jayan; Arvind ; et al.
U.S. patent application number 16/549043 was filed with the patent office on 2019-12-19 for compositions and methods for treating myelofibrosis. The applicant listed for this patent is Impact Biomedicines, Inc.. Invention is credited to Janice Cacace, Arvind Jayan.
| Application Number | 20190381041 16/549043 |
| Document ID | / |
| Family ID | 46024747 |
| Filed Date | 2019-12-19 |










View All Diagrams
| United States Patent Application | 20190381041 |
| Kind Code | A1 |
| Jayan; Arvind ; et al. | December 19, 2019 |
COMPOSITIONS AND METHODS FOR TREATING MYELOFIBROSIS
Abstract
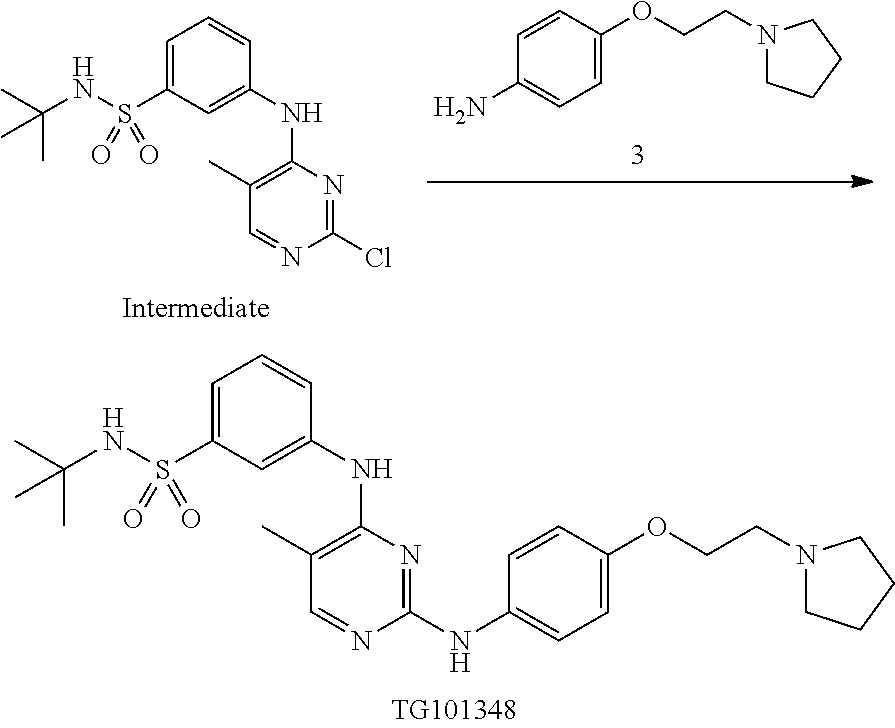
Provided herein are compositions and methods for treating myelofibrosis in a subject. The methods comprise administering to the subject an effective amount of compound which is which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutical salt thereof or a hydrate thereof.
| Inventors: | Jayan; Arvind; (La Jolla, CA) ; Cacace; Janice; (Miami, FL) | ||||||||||
| Applicant: |
|
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Family ID: | 46024747 | ||||||||||
| Appl. No.: | 16/549043 | ||||||||||
| Filed: | August 23, 2019 |
Related U.S. Patent Documents
| Application Number | Filing Date | Patent Number | ||
|---|---|---|---|---|
| 13888096 | May 6, 2013 | 10391094 | ||
| 16549043 | ||||
| PCT/US2011/059643 | Nov 7, 2011 | |||
| 13888096 | ||||
| 61410924 | Nov 7, 2010 | |||
| Current U.S. Class: | 1/1 |
| Current CPC Class: | A61P 19/08 20180101; A61P 35/00 20180101; A61P 7/00 20180101; A61K 9/4866 20130101; A61K 31/506 20130101; A61K 9/48 20130101 |
| International Class: | A61K 31/506 20060101 A61K031/506; A61K 9/48 20060101 A61K009/48 |
Claims
1-69. (canceled)
70. A unit dosage form for ingestion to the stomach, the unit dosage form comprising: (i) a compound: ##STR00006## or a pharmaceutically acceptable salt or hydrate thereof; (ii) a microcrystalline cellulose, wherein the weight ratio of the compound to the microcrystalline cellulose is about 1:1.5 to about 1:9; and (iii) about 0.5% to about 5% w/w of sodium stearyl fumarate.
71. The unit dosage form of claim 70, wherein the weight ratio of the compound to the microcrystalline cellulose is about 1:1.5 to about 1:2.
72. The unit dosage form of claim 70, wherein the microcrystalline cellulose is silicified microcrystalline cellulose.
73. The unit dosage form of claim 70, wherein the unit dosage form comprises about 0.5% to about 2% w/w of sodium stearyl fumarate.
74. The unit dosage form of claim 73, wherein the unit dosage form comprises about 1% w/w of sodium stearyl fumarate.
75. The unit dosage form of claim 70, wherein the compound is in the form of a dihydrochloride monohydrate: ##STR00007## and the weight ratio of ##STR00008## to the microcrystalline cellulose is about 1:1.5 to about 1:9.
76. The unit dosage form of claim 71, wherein the compound is in the form of a dihydrochloride monohydrate: ##STR00009## and the weight ratio of ##STR00010## to the microcrystalline cellulose is about 1:1.5 to about 1:2.
77. The unit dosage form of claim 72, wherein the compound is in the form of a dihydrochloride monohydrate: ##STR00011## and the weight ratio of ##STR00012## to the microcrystalline cellulose is about 1:1.5 to about 1:9.
78. The unit dosage form of claim 73, wherein the compound is in the form of a dihydrochloride monohydrate: ##STR00013## and the weight ratio of ##STR00014## to the microcrystalline cellulose is about 1:1.5 to about 1:9.
79. The unit dosage form of claim 74, wherein the compound is in the form of a dihydrochloride monohydrate: ##STR00015## and the weight ratio of ##STR00016## to the microcrystalline cellulose is about 1:1.5 to about 1:9.
80. A unit dosage form for ingestion to the stomach, the unit dosage form comprising: (i) a compound: ##STR00017## or a pharmaceutically acceptable salt or hydrate thereof; (ii) a microcrystalline cellulose, wherein the weight ratio of the compound to the microcrystalline cellulose is 1:1.5 to 1:9; and (iii) one or more lubricants.
81. The unit dosage form of claim 80, wherein the one or more lubricants comprises sodium stearyl fumarate.
82. The unit dosage form of claim 80, wherein the weight ratio of the compound to the microcrystalline cellulose is 1:1.5 to 1:2.
83. The unit dosage form of claim 80, wherein the microcrystalline cellulose is silicified microcrystalline cellulose.
84. The unit dosage form of claim 80, wherein the unit dosage form comprises about 0.5% to about 5% w/w of the one or more lubricants.
85. The unit dosage form of claim 84, wherein the unit dosage form comprises about 0.5% to about 2% w/w of the one or more lubricants.
86. The unit dosage form of claim 85, wherein the unit dosage form comprises about 1% w/w of the one or more lubricants.
87. The unit dosage form of claim 80, wherein the compound is in the form of a dihydrochloride monohydrate: ##STR00018## and the weight ratio of ##STR00019## to the microcrystalline cellulose is about 1:1.5 to about 1:9.
88. The unit dosage form of claim 81, wherein the compound is in the form of a dihydrochloride monohydrate: ##STR00020## and the weight ratio of ##STR00021## to the microcrystalline cellulose is about 1:1.5 to about 1:9.
89. The unit dosage form of claim 82, wherein the compound is in the form of a dihydrochloride monohydrate: ##STR00022## and the weight ratio of ##STR00023## to the microcrystalline cellulose is about 1:1.5 to about 1:2.
90. The unit dosage form of claim 83, wherein the compound is in the form of a dihydrochloride monohydrate: ##STR00024## and the weight ratio of ##STR00025## to the microcrystalline cellulose is about 1:1.5 to about 1:9.
91. The unit dosage form of claim 84, wherein the compound is in the form of a dihydrochloride monohydrate: ##STR00026## and the weight ratio of ##STR00027## to the microcrystalline cellulose is about 1:1.5 to about 1:9.
92. The unit dosage form of claim 85, wherein the compound is in the form of a dihydrochloride monohydrate: ##STR00028## and the weight ratio of ##STR00029## to the microcrystalline cellulose is about 1:1.5 to about 1:9.
93. The unit dosage form of claim 86, wherein the compound is in the form of a dihydrochloride monohydrate: ##STR00030## and the weight ratio of ##STR00031## to the microcrystalline cellulose is about 1:1.5 to about 1:9.
94. A unit dosage form for ingestion to the stomach, the unit dosage form comprising: (i) a compound: ##STR00032## or a pharmaceutically acceptable salt or hydrate thereof; (ii) one or more fillers and/or diluents; and (iii) about 0.5% to about 5% w/w of sodium stearyl fumarate.
95. The unit dosage form of claim 94, wherein the one or more fillers and/or diluents comprises a microcrystalline cellulose.
96. The unit dosage form of claim 95, wherein the microcrystalline cellulose is silicified microcrystalline cellulose.
97. The unit dosage form of claim 94, wherein the compound is in the form of a dihydrochloride monohydrate: ##STR00033##
98. The unit dosage form of claim 95, wherein the compound is in the form of a dihydrochloride monohydrate: ##STR00034##
99. The unit dosage form of claim 96, wherein the compound is in the form of a dihydrochloride monohydrate: ##STR00035##
100. A unit dosage form for ingestion to the stomach, the unit dosage form comprising: (i) a compound: ##STR00036## or a pharmaceutically acceptable salt or hydrate thereof; (ii) one or more fillers and/or diluents, wherein the ratio of the weight of the compound to the total weight of the one or more fillers and/or diluents is about 1:1.5 to about 1:9; and (iii) about 0.5% to about 5% w/w of a lubricant.
101. The unit dosage form of claim 100, wherein the compound is in the form of a dihydrochloride monohydrate: ##STR00037## and the ratio of the weight of ##STR00038## to the total weight of the one or more fillers and/or diluents is about 1:1.5 to about 1:9.
102. The unit dosage form of claim 100, wherein the ratio of the weight of the compound to the total weight of the one or more fillers and/or diluents is about 1:1.5 to about 1:2.
103. The unit dosage form of claim 100, wherein the unit dosage form comprises about 0.5% to about 2% w/w of the lubricant.
104. The unit dosage form of claim 103, wherein the unit dosage form comprises about 1% w/w of the lubricant.
Description
CROSS-REFERENCE TO RELATED APPLICATIONS
[0001] This application claims the priority benefit of U.S. provisional application Ser. No. 61/410,924, filed Nov. 7, 2010, which is incorporated herein by reference in its entirety.
TECHNICAL FIELD
[0002] Provided herein are compositions and methods for treating myelofibrosis. The compositions and methods provided herein relate to treatment of myelofibrosis with compounds that inhibit JAK2 or a pharmaceutically acceptable salt thereof or a hydrate thereof.
BACKGROUND
[0003] Myelofibrosis ("MF") is a rare disease mainly affecting people of older age. MF is a BCR-A BLI-negative myeloproliferative neoplasm ("MPN") that presents de novo (primary) or may be preceded by polycythemia vera ("PV") or essential thrombocythemia ("ET"). Clinical features include progressive anemia, marked splenomegaly, constitutional symptoms (e.g. fatigue, night sweats, bone pain, pruritus, and cough) and weight loss (Tefferi A, N Engl J Med 342:1255-1265, 2000). Median survival ranges from less than 2 years to over 15 years based on currently identified prognostic factors (Cervantes F et al., Blood 113:2895-2901, 2009; Hussein K et al. Blood 115:496-499, 2010; Patnaik M M et al., Eur J Haematol 84:105-108, 2010). Mutations involving JAK2 (James C et al., Nature 434:1144-1148, 2005; Scott L M et al., N Engl J Med 356:459-468, 2007), MPL (Pikman Y el al., PLoS Med 3:e270, 2006), TET2 (Delhommeau F et al., N Engl J Med 360:2289-2301, 2009), ASXL1 (Carbuccia N et al., Leukemia 23:2183-2186, 2009), IDH1/IDH2 (Green A et al., N Engl J Med 362:369-370, 2010; Tefferi A et al., Leukemia 24:1302-1309, 2010), CBL (Grand F H et al., Blood 113:6182-6192, 2009), IKZFI (Jager R et al., Leukemia 24:1290-1298, 2010), LINK (Oh S T et al., Blood 116:988-992, 2010), or EZH2 (Ernst T et al., Nat Genet 42:722-726) have been described in patients with MPN, including those with MF. Some mutations occur at high frequency in MF (e.g. JAK2 mutations in .about.50% patients), and either directly (e.g. JAK2 or MPL mutations) or indirectly (e.g. LNK or CBL mutations) induce JAK-STAT hyperactivation.
[0004] The currently available treatments are not effective in reversing the process of MF, be it primary or secondary disease. The only potential for cure of the disease to date is bone marrow transplantation. However, most patients are not suitable bone marrow transplant candidates because of the older median age at diagnosis, in which transplant-related morbidity and mortality tends to be high. Thus management options of MF are currently inadequate to meet the needs of all patients. The main options for active intervention include cyto-reductive therapy, e.g. with hydroxyurea, treatment of anemia with androgens, erythropoietin and splenectomy. These options have not been shown to improve survival and are largely seen as palliative (Cervantes F., Myclofibrosis: Biology and treatment options, European Journal of Haematology, 2007, 79 (suppl.68) 13-17). Therefore, there is a need to provide additional therapy options for MF patients.
SUMMARY OF THE INVENTION
[0005] Provided herein are capsules suitable for oral administration. In some embodiments, the capsule comprises an admixture of (i) a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]- amino}pyrimidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, (ii) a microcrystalline cellulose, and (iii) sodium stearyl fumarate, wherein the admixture is contained in the capsule.
[0006] In some embodiments, the capsule contains about 10 mg to about 680 mg of the compound, wherein the specified weight is the free base moiety weight of the compound. In some embodiments, the capsule contains about 10 mg to about 500 mg of the compound. In some embodiments, the capsule contains about any of 10 mg, 40 mg, 100 mg, 200 mg, 300 mg, 400 mg, 500 mg, or 600 mg of the compound. In some embodiments, the weight ratio of the compound to microcrystalline cellulose in the capsule is between about 1:1.5 to 1:15, wherein the weight for the compound in the weight ratio is the free base moiety weight of the compound. In some embodiments, the weight ratio of the compound to sodium stearyl fumarate in the capsule is between about 5:1 to about 50:1, and wherein the weight for the compound in the weight ratio is the free base moiety weight of the compound. In some embodiments, the microcrystalline cellulose is silicified microcrystalline cellulose. In some embodiments, the silicified microcrystalline cellulose is a combination of 98% microcrystalline cellulose and 2% colloidal silicon dioxide.
[0007] Also provided herein are unit dosage forms comprising an admixture of (i) a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, (ii) a microcrystalline cellulose, and (iii) sodium stearyl fumarate. In some embodiments, the unit dosage forms are for treatment of myelofibrosis such as treatment of myelofibrosis according to a method described herein.
[0008] In some embodiments, the unit dosage form comprises an admixture of (i) about 10 mg to about 680 mg (or about 10 mg to about 500 mg) of a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, wherein the specified weight is the free base moiety weight of the compound, (ii) a microcrystalline cellulose, and (iii) sodium stearyl fumarate. In some embodiments, the unit dosage form is in the form of a capsule, and the admixture is contained in the capsule. In some embodiments, the compound in the admixture is about 10 mg to about 500 mg, wherein the specified weight is the free base moiety weight of the compound. In some embodiments, the admixture comprises (i) about 10 mg (or about any of 40 mg, 100 mg, 200 mg, 300 mg. 400 mg, or 500 mg) of the compound, (ii) a microcrystalline cellulose, and (iii) sodium stearyl fumarate, wherein the specified weight is the free base moiety weight of the compound. In some embodiments, the compound is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide dihydrochloride monohydrate. In some embodiments, the weight ratio of the compound to microcrystalline cellulose in the capsule is between about 1:1.5 to 1:15, wherein the weight for the compound in the weight ratio is the free base moiety weight of the compound. In some embodiments, the weight ratio of the compound to sodium stearyl fumarate in the capsule is between about 5:1 to about 50:1, and wherein the weight for the compound in the weight ratio is the free base moiety weight of the compound. In some embodiments, the microcrystalline cellulose is silicified microcrystalline cellulose. In some embodiments, the silicified microcrystalline cellulose is a combination of 98% microcrystalline cellulose and 2% colloidal silicon dioxide.
[0009] In some embodiments, sodium stearyl fumarate is about 1% w/w of capsule fill weight. In some embodiments, the weight ratio of the compound to microcrystalline cellulose such as silicified microcrystalline cellulose is about 40:60 to about 10:90 (e.g., about 40:60 or about 1:1.5, or about 10:90 or about 1:9).
[0010] In some embodiments, the compound is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide dihydrochloride monohydrate. In some embodiments, the unit dosage form or capsule contains an admixture of about 12 mg of N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide dihydrochloride monohydrate, about 122 mg of silicified microcrystalline cellulose, and about 1 mg of sodium stearyl fumarate. In some embodiments, the unit dosage form or capsule contains an admixture of about 47 mg of N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide dihydrochloride monohydrate, about 448 mg of silicilfed microcrystalline cellulose, and about 5 mg of sodium stearyl fumarate. In some embodiments, the unit dosage form or capsule contains an admixture of about 117 mg of N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide dihydrochloride monohydrate. In some embodiments, the unit dosage form or capsule contains an admixture of about 235 mg of N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide dihydrochloride monohydrate, about 357 mg of silicified microcrystalline cellulose, and about 6.00 mg of sodium stearyl fumarate. In some embodiments, the capsule is a hard gelatin capsule.
[0011] Also provided herein are methods of preparing a capsule drug product comprising a) blending a lubricant with a compound that is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof to generate granules and b) mixing the granules of a) with an excipient. In some embodiments, the lubricant is sodium stearyl fumarate. In some embodiments, the excipient is microcrystalline cellulose such as silicified microcrystalline cellulose. In some embodiments, sodium stearyl fumarate is about 1% w/w of capsule fill weight. In some embodiments, the weight ratio of the compound to silicified microcrystalline cellulose is about 1:1.5 to about 1:9. In some embodiments, the weight ratio of the compound to silicified microcrystalline cellulose is about 1:1.5. In some embodiments, the weight ratio of the compound to silicified microcrystalline cellulose is about 1:9. In some embodiments, the capsule is a hard gelatin capsule.
[0012] Also provided herein are methods of treating myelofibrosis in a subject, comprising orally administering a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, and wherein the compound is in an admixture of (i) the compound, (ii) an excipient (e.g., a microcrystalline cellulose), and (iii) a lubricant (e.g., sodium stearyl fumarate). Any of the unit dosage forms or capsules described herein may be used. In some embodiments, there is provided a method of treating myelofibrosis in a subject comprising orally administering a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, and wherein the compound is in a capsule containing an admixture of (i) the compound, (ii) a microcrystalline cellulose (e.g., silicified microcrystalline cellulose), and (iii) sodium stearyl fumarate.
[0013] Also provided herein are methods of treating myelofibrosis in a subject, comprising administering to the subject an effective amount of a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, wherein the subject is negative for the valine 617 to phenylalanine mutation of human Janus Kinase 2 (JAK2) or negative for the mutation corresponding to the valine 617 to phenylalanine mutation of human JAK2.
[0014] Also provided herein are methods of treating myelofibrosis in a subject, comprising administering to the subject an effective amount of a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, wherein the subject has previously received another myelofibrosis therapy. In some embodiments, the previous therapy is a treatment with a JAK2 inhibitor which is not N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof. In some embodiments, the previous therapy comprises administration of INCB018424 (ruxolitinib). In some embodiments, the subject is unresponsive to the previous therapy. In some embodiments, the previous therapy is a treatment with N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof. In some embodiments, the previous therapy has been discontinued upon indication of elevated levels of amylase, lipase, aspartate aminotransferase ("AST"), alanine aminotransferase ("ALT"), and/or creatinine. In some embodiments, the previous therapy has been discontinued upon indication of a hematologic condition selected from the group consisting of anemia, thrombocytopenia, and neutropenia.
[0015] Also provided herein are methods of ameliorating bone marrow cellularity or bone marrow fibrosis associated with myelofibrosis in a subject, comprising administering to the subject an effective amount of a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof.
[0016] Also provided herein are methods of improving pruritus associated with myelofibrosis in a subject, comprising administering to the subject an effective amount of a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof.
[0017] Also provided herein are methods of monitoring treatment of myelofibrosis in a subject, comprising (a) administering to a subject an effective amount of a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof; (b) monitoring a non-hematologic parameter selected from the group consisting of amylase level, lipase level, aspartate aminotransferase (AST) level, alanine aminotransferase (ALT) level, and creatinine level in the subject; and (c) determining if the subject should continue or discontinue with the treatment. Also provided herein are methods of monitoring treatment of myelofibrosis to a subject, comprising administering to the subject an effective amount of a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]- amino}pyrimidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, and discontinuing the treatment upon indication of elevated levels of one or more enzymes or molecules selected from the group consisting of amylase, lipase, aspartate aminotransferase (AST), alanine aminotransferase (ALT), and creatinine in the serum of the subject without prior dose reduction. In some embodiments, the one or more of the elevated levels are Grade 4 events.
[0018] Also provided herein are methods of monitoring a treatment of myelofibrosis to a subject, comprising (a) administering to the subject an effective amount of a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof; (b) monitoring a hematologic parameter selected from the group consisting of anemia, thrombocytopenia, and neutropenia in the serum of the subject; and (c) determining if the subject should continue or discontinue with the treatment. Also provided herein are methods of monitoring treatment of myelofibrosis to a subject, comprising administering to the subject an effective amount of a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]- amino}pyrimidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, and discontinuing the treatment upon indication of one or more hematologic conditions selected from the group consisting of anemia, thrombocytopenia, and neutropenia without prior dose reduction. In some embodiments, the one or more hematologic conditions are grade 4 events.
[0019] In some embodiments of the methods of monitoring treatment provided herein, the methods further comprise administering to the subject an effective amount of a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof after the subject has been discontinued with the treatment for at least 2 weeks. In some embodiments, the subject has been discontinued with the treatment for at least 3 weeks. In some embodiments, the subject has been discontinued with the treatment for at least 4 weeks. In some embodiments, the treatment has been discontinued without prior dose reduction.
[0020] In some embodiments, the compound is administered to the human subject at a dose of about 240 mg per day to about 680 mg per day, and wherein the specified weight is the free base moiety weight of the compound. In some embodiments, the compound is administered at a dose of about 300 mg per day to about 500 mg per day (e.g., about 300 mg per day to about 400 mg per day, or about 400 mg per day to about 500 mg per day), and wherein the specified weight is the free base moiety weight of the compound. In some embodiments, the compound is administered at a dose of about any of 240 mg per day, 250 mg per day, 300 mg per day, 350 mg per day, 400 mg per day, 450 mg per day, 500 mg per day, 550 mg per day, 600 mg per day, 650 mg per day, or 680 mg per day, and wherein the specified weight is the free base moiety weight of the compound. In some embodiments, the compound is administered daily and/or orally. In some embodiments, the compound is administered over a period of at least 1 cycle, at least 2 cycles, at least 3 cycles, at least 4 cycles, at least 5 cycles, or at least 6 cycles (e.g., at least 7 cycles, at least 8 cycles, at least 9 cycles, at least 10 cycles, at least 11 cycles, at least 12 cycles, at least 15 cycles, at least 18 cycles, or at least 24 cycles) of a 28-day treatment cycle. In some embodiments, the compound is in a capsule and administered orally. In some embodiments, the compound is in a unit dosage form. Any of the capsules or unit dosage forms described herein may be administered. In some embodiments of the methods provided herein, the compound is in an admixture of (i) a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}- pyrimidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, (ii) a microcrystalline cellulose, and (iii) sodium stearyl fumarate. In some embodiments, the weight ratio of the compound to microcrystalline cellulose in the admixture is between about 1:1.5 to 1:15, and wherein the weight for the compound is the free base moiety weight of the compound. In some embodiments, the weight ratio of the compound to sodium stearyl fumarate in the admixture is between about 5:1 to about 50:1, and wherein the weight for the compound is the free base moiety weight of the compound. In some embodiments, the compound is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide dihydrochloride monohydrate. In some embodiments, the microcrystalline cellulose is silicified microcrystalline cellulose. In some embodiments, the subject is a human.
[0021] In some embodiments of the compositions and methods provided herein, the subject has primary myelofibrosis. In some embodiments of the compositions and methods provided herein, the subject has post polycythemia vera myelofibrosis. In some embodiments of the compositions and methods provided herein, the subject has post essential thrombocythemia myelofibrosis. In some embodiments, the subject has high risk myelofibrosis. In some embodiments, the subject has intermediate risk myelofibrosis (such as intermediate risk level 2). In some embodiments of the compositions and methods provided herein, the subject is positive for the valine 617 to phenylalanine mutation of human Janus Kinase 2 (JAK2) or positive for the mutation corresponding to the valine 617 to phenylalanine mutation of human JAK2. In some embodiments of the compositions and methods provided herein, the subject is negative for the valine 617 to phenylalanine mutation of human Janus Kinase 2 (JAK2) or negative for the mutation corresponding to the valine 617 to phenylalanine mutation of human JAK2. In some embodiments of the compositions and methods provided herein, the subject has palpable splenomegaly. In some embodiments, the subject with myelofibrosis has spleen of at least 5 cm below costal margin as measured by palpation. In some embodiments of the compositions and methods provided herein, the subject is transfusion dependent. In some embodiments of the compositions and methods provided herein, the subject is not transfusion dependent.
[0022] In some embodiments of the methods provided herein, upon administration of the compound to a human subject, the Cmax of the compound is achieved within about 2 to about 4 hours post-dose. In some embodiments, upon administration of the compound to a human subject, the elimination half life of the compound is about 16 to about 34 hours. In some embodiments, the mean AUC of the compound increases more than proportionally with increasing doses ranging from about 30 mg to about 800 mg per day. In some embodiments, the accumulation of the compound is about 1.25 to about 4.0 fold at steady state when the compound is dosed once daily. In some embodiments, the compound is in an admixture of (i) a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, (ii) microcrystalline cellulose, and (iii) sodium stearyl fumarate. In some embodiments, the weight ratio of the compound to microcrystalline cellulose in the admixture is between about 1:1.5 to 1:15, and wherein the weight for the compound is the free base moiety weight of the compound. In some embodiments, the weight ratio of the compound to sodium stearyl fumarate in the admixture is between about 5:1 to about 50:1, and wherein the weight for the compound is the free base moiety weight of the compound. In some embodiments, the compound is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide dihydrochloride monohydrate. In some embodiments, the microcrystalline cellulose is silicified microcrystalline cellulose.
[0023] Also provided herein are articles of manufacture or kits comprising (a) any one of the capsules provided herein, and (b) a package insert or a label indicating that the capsule is useful for treating myelofibrosis in a subject. Also provided herein are articles of manufacture or kits comprising (a) any one of the unit dosage forms provided herein, and (b) a package insert or a label indicating that the capsule is useful for treating myelofibrosis in a subject. In some embodiments, there is provided an article of manufacture or kit comprising (a) an admixture of (i) a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, (ii) microcrystalline cellulose, and (iii) sodium stearyl fumarate, and (b) a package insert or a label indicating that the admixture is useful for treating myelofibrosis in a subject.
[0024] Also provided herein are articles of manufacture or kits comprising (a) a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutical salt thereof or a hydrate thereof, and (b) a package insert or a label indicating that the compound can be used for treating myelofibrosis in a subject, wherein the subject is negative for the valine 617 to phenylalanine mutation of human Janus Kinase 2 (JAK2) or negative for the mutation corresponding to the valine 617 to phenylalanine mutation of human JAK2.
[0025] Also provided herein are articles of manufacture or kits comprising (a) a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutical salt thereof or a hydrate thereof, and (b) a package insert or a label indicating that the compound can be used for treating myelofibrosis in a subject, wherein the subject has previously received another myelofibrosis therapy. In some embodiments, the previous therapy is a treatment with a JAK2 inhibitor which is not N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof.
[0026] Also provided herein are articles of manufacture or kits comprising (a) a compound which is N-ter-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyri- midin-4-yl)amino]benzenesulfonamide or a pharmaceutical salt thereof or a hydrate thereof, and (b) a package insert or a label indicating that the compound can be used for ameliorating bone marrow cellularity and/or bone marrow fibrosis.
[0027] Also provided herein are articles of manufacture or kits comprising (a) a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutical salt thereof or a hydrate thereof, and (b) a package insert or a label indicating that the compound can be used for improving pruritus associated with myelofibrosis.
[0028] Also provided herein are articles of manufacture or kits comprising a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutical salt thereof or a hydrate thereof, and a package insert or a label indicating that the compound can be used for treating myelofibrosis in a subject, and that subject should discontinue the treatment upon indication of elevated levels of one or more enzymes or molecules selected from the group consisting of: amylase, lipase, aspartate aminotransferase (AST), alanine aminotransferase (ALT), and creatinine in the serum of the subject, and/or upon indication of one or more hematologic condition selected from the group consisting of anemia, thrombocytopenia, and neutropenia. In some embodiments, the package insert or the label further indicates that the compound can be discontinued without prior dose reduction. In some embodiments, the one or more of the elevated levels of the enzymes or molecules are Grade 4 events. In some embodiments, the one or more of the hematologic conditions are Grade 4 events.
[0029] In some embodiments, the package insert or the label is in a position which is visible to prospective purchasers. In some embodiments, the compound is in a unit dosage form or capsule form.
[0030] In some embodiments, the package insert or the label indicates that, upon administration of the admixture to a human subject, the Cmax of the compound is achieved within about 2 to about 4 hours post-dose. In some embodiments, the package insert or the label indicates that, upon administration of the compound to a human subject, the elimination half life of the compound is about 16 to about 34 hours. In some embodiments, the package insert or the label indicates that the mean AUC of the compound increases more than proportionally with increasing doses ranging from about 30 mg to about 800 mg per day. In some embodiments, the package insert or the label indicates that the accumulation of the compound is about 1.25 to about 4.0 fold at steady state when the compound is dosed once daily. In some embodiments, the compound is in an admixture of (i) a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, (ii) a microcrystalline cellulose, and (iii) sodium stearyl fumarate. In some embodiments, the weight ratio of the compound to microcrystalline cellulose in the admixture is between about 1:1.5 to 1:15, and wherein the weight for the compound is the free base moiety weight of the compound. In some embodiments, the weight ratio of the compound to sodium stearyl fumarate in the admixture is between about 5:1 to about 50:1, and wherein the weight for the compound is the free base moiety weight of the compound. In some embodiments, the compound is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide dihydrochloride monohydrate. In some embodiments, the microcrystalline cellulose is silicified microcrystalline cellulose.
[0031] In some embodiments, there is provided use of a compound in the manufacture of a medicament for treating myelofibrosis in a subject, wherein the compound is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof. In some embodiments, the compound is in an admixture of (i) the compound, (ii) an excipient (e.g., microcrystalline cellulose such as silicified microcrystalline cellulose), and (iii) a lubricant (e.g., sodium stearyl fumarate). In some embodiments, the compound is administered orally. In some embodiments, the use is according to a method described herein.
[0032] In some embodiments, there is provided use of a compound in the manufacture of a medicament for treating myelofibrosis in a subject, wherein the compound is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, wherein the subject is negative for the valine 617 to phenylalanine mutation of human Janus Kinase 2 (JAK2) or negative for the mutation corresponding to the valine 617 to phenylalanine mutation of human JAK2. In some embodiments, there is provided use of a compound in the manufacture of a medicament for treating myelofibrosis in a subject, wherein the compound is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, wherein the subject has previously received another myelofibrosis therapy. In some embodiments, the previous therapy comprises a JAK2 inhibitor which is not N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzensulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof. In some embodiments, the use is according to a method described herein.
[0033] In some embodiments, there is provided a compound for treating myelofibrosis in a subject, wherein the compound is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof. In some embodiments, the compound is in an admixture of (i) the compound, (ii) an excipient (e.g., microcrystalline cellulose such as silicified microcrystalline cellulose), and (iii) a lubricant (e.g., sodium stearyl fumarate). In some embodiments, the compound is administered orally. In some embodiments, the treatment is according to a method described herein.
[0034] In some embodiments, there is provided a compound for treating myelofibrosis in a subject, wherein the compound is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, wherein the subject is negative for the valine 617 to phenylalanine mutation of human Janus Kinase 2 (JAK2) or negative for the mutation corresponding to the valine 617 to phenylalanine mutation of human JAK2. In some embodiments, there is provided a compound for treating myelofibrosis in a subject, wherein the compound is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, wherein the subject has previously received another myelofibrosis therapy. In some embodiments, the previous therapy comprises a JAK2 inhibitor which is not N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof. In some embodiments, the treatment is according to a method described herein.
[0035] It is to be understood that one, some, or all of the properties of the various embodiments described herein may be combined to form other embodiments of the compositions and methods provided herein. These and other aspects of the compositions and methods provided herein will become apparent to one of skill in the art.
BRIEF DESCRIPTION OF THE FIGURES
[0036] FIG. 1 shows decrease in palpable spleen size by cycle for patients treated with TG101348 680 mg/day (starting dose) (N=37). Doses for cycle 1 were 520-800 mg/day and doses for cycles 2-6 were 360-680 mg/day. For cycle 6 .gtoreq.50% subjects, there was 22-47% increase in 3 subjects with drug held for .about.2-3 weeks immediately prior to measurement.
[0037] FIG. 2 shows WBC count in subjects treated with TG101348. The baseline WBC count was >1.times.10.sup.9/L. The doses at follow-up ranged from 360 to 680 mg/day. Last follow-up visit ranged from 8 to 24 weeks (median 24 weeks). "ULN" means upper limit of normal.
[0038] FIG. 3 shows platelet count in subjects treated with TG101348. The baseline platelet count >450.times.10.sup.9/L. The doses at follow-up ranged from 360 to 680 mg/day. Last follow-up visit ranged from 12 to 24 weeks (median 24 weeks). "ULN" means upper limit of normal.
[0039] FIG. 4 shows the percentages of subjects with worsened, unchanged, improved or resolved constitutional symptoms (fatigue, early satiety, cough, night sweats, and pruritus) in subjects treated with TG101348. Last visit ranged from 4 to 24 weeks (median 20 weeks). The data here reflected changes from symptoms present at baseline. 18 subjects reported new onset of .gtoreq.1 symptom during the study; of these, symptoms for 12 subjects were resolved by last follow-up visit. Severity was rated by subjects on a scale of 1-10: 0=absent; 1-3=mild; 4-7=moderate; 8-10=severe. Improved=downgrade to absent or to mild or moderate from more severe rating at baseline.
[0040] FIG. 5 shows the cytokine levels (IL-6. IL-8, IL-2 and TNF-.alpha.) in subjects treated with TG101348. The values shown are median values.
[0041] FIG. 6 shows the change in V617F allele burden from baseline as a proportion of baseline in subjects with baseline >20% (N=22) treated with TG101348. The figure shows the subset of JAK2V617F positive subjects in the overall population (N=48). The doses at follow-up were 360 to 680 mg/day. Last follow-up visit ranged from 20 to 72 weeks (median 24 weeks).
[0042] FIG. 7 shows the bone marrow cellularity at baseline (60% cellularity) and after 18 cycles of TG101348 treatment (5-10% cellularity) in a 76-year-old male subject with V617F negative PMF. The starting dose was 30 mg/day and the dose at follow-up was 520 mg/day.
[0043] FIG. 8 shows the bone marrow fibrosis at baseline (3+) and after 18 cycles of TG101348 treatment (0) in a 56-year-old male subject with V617F negative PMF. The starting dose was 240 mg/day and the dose at follow-up was 440 mg/day.
[0044] FIG. 9 shows various measurements of a subject with JAK2 V617F-positive PMF treated with TG101348 (starting dose at 680 mg/day).
[0045] FIGS. 10A-10G show distribution of TG1101348 doses at the end of each cycle for subjects who initiated dosing at 30 mg/day, 60 mg/day, 120 mg/day, 240 mg/day, 360 mg/day, 520 mg/day, and 800 mg/day, respectively, (n=25).
[0046] FIG. 11 shows distribution of TO 101348 doses at the end of each cycle for subjects who initiated dosing at 680 mg/day (n=34).
[0047] FIG. 12A shows plot of mean plasma TG101348 concentrations versus time on a semi-log scale (Cycle 1, Day 1). FIG. 12B shows plot of mean plasma TG101348 concentrations versus time on a semi-log scale (Cycle 1, Day 28).
[0048] FIG. 13 shows splenomegaly response to TG101348 therapy. This figure shows decrease in palpable spleen size from baseline by cycle for subjects in the maximum tolerated dose cohort (n=37). The proportion of subjects with >50% and 100% decrease in palpable splenomegaly is shown. For subjects who completed 6 cycles of treatment, 90% had a >25% reduction in palpable spleen size, 66% had a >50% reduction, and in 31% the spleen became non palpable.
[0049] FIGS. 14A-14C show effects of TG101348 on symptoms of myelofibrosis. (A): Proportion of subjects in maximum tolerated dose cohort with complete resolution of early satiety by cycle from a baseline symptom score of "mild" (score=1-3), "moderate" (score=4-7), or "severe" (score=8-10). Twenty-seven (79%) and 19 (56%) patients were evaluable for improvement in early satiety at the end of 1 and 6 cycles, respectively. After 2 cycles of treatment, 56% reported complete resolution of this symptom with durable benefit. (H): Proportion of subjects in maximum tolerated dose cohort with complete resolution of fatigue by cycle from a baseline symptom score of "mild" (score=1-3), or improvement in or complete resolution of fatigue from a baseline score of "moderate" (score=4-7) or "severe" (score=8-10). Twenty-four (71%) and 16 (47%) patients were evaluable for improvement in fatigue at the end of 1 and 6 cycles, respectively. After 6 cycles, 63% reported improvement and 25% had complete resolution of this symptom. (C): Proportion of subjects in maximum tolerated dose cohort with complete resolution of night sweats by cycle from a baseline symptom score of "mild" (score=1-3), "moderate" (score=4-7), or "severe" (score=8-10). Fourteen (40%) and 9 (26%) patients were evaluable for improvement in night sweats at the end of 1 and 6 cycles, respectively. After 1 cycle, 64% of subjects had complete resolution of this symptom; after 6 cycles, this proportion had increased to 89%.
[0050] FIG. 15 shows response of leukocytosis to TG101348 therapy. Changes in white blood cell (WBC) count after 6 cycles for subjects who entered the study with leukocytosis (WBC count >11.times.10.sup.9/L). Following 6 cycles, 16 subjects across doses (57%) and 13 subjects in the MTD cohort (72%) achieved a normal WBC count, with durable benefit.
[0051] FIGS. 16A-16D show effect of TG101348 therapy on JAK2V617F allele burden. Box plot representation of JAK2V617F allele burden data for all mutation-positive subjects (n=51; figures A and B) and for the subgroup with baseline allele burden >20% (n=23; FIGS. 16C and 16D). The y-axis represents the JAK2V617F allele burden from 1.0 (100%) to 0.0 (0%). The change in JAK2V617F allele burden per cycle of treatment (up to end of cycle 12; i.e. C13D1) as compared to pre-study baseline is shown for the 2 groups (FIGS. 16A and 16C); the change at the end of cycle 6 (i.e. C7D1) and cycle 12 is shown in FIGS. 16B and 16D. A significant decrease in JAK2V617F allele burden as compared to pre-study baseline was observed at the end of cycle 6 for the mutation-positive group (FIG. 16B; p=-0.04) and the subgroup with baseline allele burden >20% (FIG. 16D; p=0.002); a similar significant decrease was seen at the end of cycle 12 for the former (FIG. 16B; p=0.01) and latter (FIG. 16D; p-0.002) groups. The Wilcoxon matched-pair signed-rank test was used to compare the median JAK2V617F allele burden for the comparisons.
[0052] FIG. 17 shows absolute changes in pro-inflammatory cytokine levels from baseline at cycle 6: IL-6 (A), TNF-.alpha. (B), IL-8 (C), and IL-2 (D). Absolute differences in IL-6 (-4719 pg/mL) and IL-2 (-1827 pg/mL) are omitted from FIGS. 17A and 17D, respectively, for 1 subject (101-039) because they skewed presentation of data for other subjects.
[0053] FIG. 18 shows a plot of mean plasma TG101348 concentrations versus time on a linear plot after once daily oral doses (Cycle 1: Day 28).
DETAILED DESCRIPTION
I. Definitions
[0054] As used herein, "treatment" or "treating" is an approach for obtaining beneficial or desired results including clinical results. Beneficial or desired clinical results can include, but are not limited to, one or more of the following: decreasing symptoms resulting from the disease, increasing the quality of life of those suffering from the disease, decreasing the dose of other medications required to treat the disease, delaying the progression of the disease, and/or prolonging survival of individuals. In some embodiments, for the treatment of myelofibrosis, beneficial clinical results include one or more of reduction of splenomegaly, improvement in constitutional symptoms (such as early satiety, fatigue, night sweats, cough, and pruritus), reduction of leukocytosis, reduction of thrombocytosis, decrease of JAK2V617F allele burden, reduction of bone marrow fibrosis, and/or reduction of bone marrow cellularity.
[0055] As used herein, "delaying development of a disease" means to defer, hinder, slow, retard, stabilize, and/or postpone development of the disease (such as myelofibrosis) or symptoms of the disease, and can include "progression free survival". This delay can be of varying lengths of time, depending on the history of the disease and/or individual being treated. As is evident to one skilled in the art, a sufficient or significant delay can, in effect, encompass prevention, in that the individual does not develop the disease.
[0056] As used herein, an "effective dosage" or "effective amount" of drug, compound, or pharmaceutical composition is an amount sufficient to effect beneficial or desired results. For prophylactic use, beneficial or desired results can include, for example, one or more results such as eliminating or reducing the risk, lessening the severity, or delaying the onset of the disease, including biochemical, histological and/or behavioral symptoms of the disease, its complications and intermediate pathological phenotypes presenting during development of the disease. For therapeutic use, beneficial or desired results can include, include, for example one or more clinical results such as decreasing one or more symptoms and pathological conditions resulting from or associated with the disease, increasing the quality of life of those suffering from the disease, decreasing the dose of other medications required to treat the disease, enhancing effect of another medication such as via targeting, delaying the progression of the disease, and/or prolonging survival. In the case of myelofibrosis, an effective amount of a drug may have the effect in reducing one or more of splenomegaly, improving constitutional symptoms (such as early satiety, fatigue, night sweats, cough, and pruritus), reducing leukocytosis, reducing thrombocytosis, decreasing JAK2V617F allele burden, reducing bone marrow fibrosis, and/or reducing bone marrow cellularity. An effective dosage can be administered in one or more administrations. An effective dosage of drug, compound, or pharmaceutical composition can be, for example, an amount sufficient to accomplish prophylactic or therapeutic treatment either directly or indirectly. As is understood in the clinical context, an effective dosage of a drug, compound, or pharmaceutical composition may or may not be achieved in conjunction with another drug, compound, or pharmaceutical composition. Thus, an "effective dosage" may be considered in the context of administering one or more therapeutic agents, and a single agent may be considered to be given in an effective amount if, in conjunction with one or more other agents, a desirable result may be or is achieved.
[0057] As used herein, "ameliorating" bone marrow cellularity or bone marrow fibrosis refers to reducing the level of bone marrow cellularity or bone marrow fibrosis in a subject compared to the level of bone marrow cellularity or bone marrow fibrosis prior to commencing treatment with the compound provided herein. The reduction of bone marrow cellularity or bone marrow fibrosis can be at least by 5, 10, 20, 30, 40, 50, 60, 70, 80, or 90%.
[0058] As used herein, "in conjunction with" refers to administration of one treatment modality in addition to another treatment modality. As such, "in conjunction with" can refer to administration of one treatment modality before, during or after administration of the other treatment modality to the individual.
[0059] As used herein, a "patient" or a "subject" refers to a mammal including a human, a dog, a horse, a cow or a cat, etc.
[0060] The term "pharmaceutically acceptable" refers to the fact that the carrier, diluent or excipient must be compatible with the other ingredients of the formulation and can be administered to a subject.
[0061] As used herein, "pharmaceutically acceptable salts" refer to derivatives of the disclosed compounds wherein the parent compound is modified by making acid or base salts thereof.
[0062] As used herein and in the appended claims, the singular forms "a," "an," and "the" include plural reference unless the context clearly indicates otherwise.
[0063] Reference to "about" a value or parameter herein includes (and describes) embodiments that are directed to that value or parameter per se. For example, description referring to "about X" includes description of "X."
[0064] It is understood that aspects and variations of the compositions and methods provided herein can include "consisting" and/or "consisting essentially of" aspects and variations.
II. Compounds and Pharmaceutical Compositions
[0065] Provided herein is a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof. Also provided herein are pharmaceutical compositions comprising N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzensulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, and a pharmaceutically acceptable excipient or carrier. The compound and the pharmaceutical compositions described herein can be used for treating or delaying development of myelofibrosis in a subject. N-tert-Butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide has the following chemical structure:
##STR00001##
[0066] The compound provided herein may be formulated into therapeutic compositions as natural or salt forms. Pharmaceutically acceptable non-toxic salts include the base addition salts (formed with free carboxyl or other anionic groups) which may be derived from inorganic bases such as, for example, sodium hydroxide, potassium hydroxide, ammonium hydroxide, calcium hydroxide, or ferric hydroxide, and such organic bases as isopropylamine, trimethylamine, 2-ethylamino-ethanol, histidine, procaine, and the like. Such salts may also be formed as acid addition salts with any free cationic groups and will generally be formed with inorganic acids such as, for example, hydrochloric acid, sulfuric acid, or phosphoric acid, or organic acids such as acetic acid, citric acid, p-toluenesulfonic acid, methanesulfonic acid, oxalic acid, tartaric acid, mandelic acid, and the like.
[0067] Salts of the compounds provided herein can include amine salts formed by the protonation of an amino group with inorganic acids such as hydrochloric acid, hydrohromic acid, hydroiodic acid, sulfuric acid, phosphoric acid, and the like. Salts of the compounds provided herein can also include amine salts formed by the protonation of an amino group with suitable organic acids, such as p-toluenesulfonic acid, acetic acid, methanesulfonic acid and the like. Additional excipients which are contemplated for use in the practice of the compositions and methods provided herein are those available to those of ordinary skills in the art, for example, those found in the United States Pharmacopeia Vol. XXII and National Formulary Vol. XVII, U.S. Pharmacopeia Convention, Inc., Rockville, Md. (1989), the relevant contents of which are incorporated herein by reference.
[0068] In addition, the compounds provided herein can include polymorphs. The compound described herein may be in alternative forms. For example, the compound described herein may include a hydrate form. As used herein, "hydrate" refers to a compound provided herein which is associated with water in the molecular form, i.e., in which the H--OH bond is not split, and may be represented, for example, by the formula R.H.sub.2O, where R is a compound provided herein. A given compound may form more than one hydrate including, for example, monohydrates (R.H.sub.2O) or polyhydrates (R.nH.sub.2O wherein n is an integer greater than 1) including, for example, dihydrates (R.2H.sub.2O), trihydrates (R.3H.sub.2O), and the like, or fractional hydrates, such as, for example, R.n/2H.sub.2O, R.n/3H.sub.2O, R.n/4H.sub.2O and the like wherein n is an integer.
[0069] The compounds described herein may also include acid salt hydrate forms. As used herein, "acid salt hydrate" refers to a complex that may be formed through association of a compound having one or more base moieties with at least one compound having one or more acid moieties or through association of a compound having one or more acid moieties with at least one compound having one or more base moieties, said complex being further associated with water molecules so as to form a hydrate, wherein said hydrate is as previously defined and R represents the complex herein described above.
[0070] In some embodiments, the compound is N-tert-butyl-3-[(5-methyl-2-{([4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}py- rimidin-4-yl)amino]benzenesulfonamide dihydrochloride monohydrate and has the following chemical structure:
##STR00002##
[0071] The pharmaceutical compositions for the administration of the compound described herein, either alone or in combination with other therapeutic agents, may conveniently be presented in dosage unit form and may be prepared by any of the methods well known in the art of pharmacy and methods described in Examples 4, 5 and 6. Such methods can include bringing the active ingredient into association with the carrier which constitutes one or more accessory ingredients. In general, the pharmaceutical compositions are prepared by uniformly and intimately bringing the active ingredient into association with a liquid carrier or a finely divided solid carrier or both, and then, if necessary, shaping the product into the desired formulation. In the pharmaceutical composition the active object compound is included in an amount sufficient to produce the desired effect upon the process or condition of diseases. The pharmaceutical compositions containing the active ingredient may be in a form suitable for oral use, for example, as hard or soft capsules. The suitable capsule shell may be hard gelatin or hydroxypropylmethyl cellulose ("HPMC").
[0072] Provided herein are formulations comprising (i) a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, (ii) one or more excipients, and (iii) one or more lubricants. The formulations may be in capsule form and administered orally. The formulations may be in unit dosage form. In some embodiments, the excipient is lactose (such as Fast-Flo), mannitol (such as Parteck M200), microcrystalline cellulose ("MCC") (such as Avicel PII102), MCC (such as ProSolv 90 IID). In some embodiments, the lubricant is magnesium stearate, sodium stearyl fumarate (such as Pruv), or sodium laurel fumarate. In some embodiments, the microcrystalline cellulose is silicified microcrystalline cellulose. In some embodiments, the capsule is hard gelatin capsule.
[0073] In some embodiments, there is provided a capsule suitable for oral administration comprising an admixture of (i) a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, (ii) an excipient (e.g., microcrystalline cellulose such as silicified microcrystalline cellulose), and (iii) a lubricant (e.g., sodium stearyl fumarate), wherein the admixture is contained in the capsule. Methods known in the art and described herein may be used for making the capsules. See, e.g., Example 3. Microcrystalline cellulose may be used as a filler and/or diluent in the capsules provided herein. Sodium stearyl fumarate may be used as a lubricant in the capsules provided herein. In some embodiments, the microcrystalline cellulose is silicified microcrystalline cellulose. For example, silicified microcrystalline cellulose may be composed of microcrystalline cellulose and colloidal silicon dioxide particles. In some embodiments, the silicified microcrystalline cellulose is a combination of 98% microcrystalline cellulose and 2% colloidal silicon dioxide.
[0074] In some embodiments, the capsule contains about 10 mg to about 680 mg of the compound, wherein the specified weight is the free base moiety weight of the compound. In some embodiments, the capsule contains about 10 mg to about 650 mg (or about 10 mg to about 550 mg or about 10 mg to about 500 mg), wherein the specified weight is the free base moiety weight of the compound. In some embodiments, the capsule contains about 100 mg to about 600 mg (or about 200 mg to about 550 mg or about 300 mg to about 500 mg), wherein the specified weight is the free base moiety weight of the compound. In some embodiments, the capsule contains about 10 mg, about 20 mg, about 40 mg, about 100 mg, about 150 mg, about 200 mg, about 250 mg, about 300 mg, about 350 mg, about 400 mg, about 450 mg, about 500 mg, about 550 mg, about 600 mg, or about 650 mg of the compound, wherein the specified weight is the free base moiety weight of the compound. In some embodiments, the capsule is a hard gelatin capsule. In some embodiments, the compound is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide dihydrochloride monohydrate.
[0075] In some embodiments, the weight ratio of the compound to excipient (e.g., microcrystalline cellulose such as silicified microcrystalline cellulose) in the capsule is between about 1:1.5 to about 1:15 (e.g., between about 1:5 to about 1:10, between about 1:5 to about 1:12, or between about 1:10 to about 1:15), wherein the weight of the compound is the free base moiety weight of the compound. In some embodiments, the weight ratio of the compound to lubricant (e.g., sodium stearyl fumarate) in the capsule is between about 5:1 to about 50:1 (e.g., between about 5:1 to about 10:1, between about 5:1 to about 25:1, between about 5:1 to about 40:1, between about 7:1 to about 34:1, or between about 8:1 to about 34:1), wherein the weight of the compound is the free base moiety weight of the compound.
[0076] In some embodiments, the capsule contains about 5% to about 50% (e.g., about 5% to about 10% or about 5% to about 35%) compound of the total fill weight of the capsule, wherein the weight of the compound is the free base moiety weight of the compound. In some embodiments, the capsule contains about 40% to about 95% (e.g., about 50% to about 90% or about 60% to about 90%) excipient (e.g., microcrystalline cellulose such as silicified microcrystalline cellulose) of the total fill weight of the capsule. In some embodiments, the capsule contains about 0.2% to about 5% (e.g., about 0.2% to about 2% or about 0.5% to about 1.5%, or about 0.5%, about 1%, or about 1.5%) lubricant (e.g., sodium stearyl fumarate) of the total fill weight of the capsule.
[0077] Also provided herein are unit dosage forms comprising an admixture of (i) a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, (ii) an excipient (such as microcrystalline cellulose), and (iii) a lubricant (such as sodium stearyl fumarate). Any one of the capsules described herein may be used in a unit dosage form. In some embodiments, the unit dosage form is for treating myelofibrosis. In some embodiments, the treatment is according to a method described herein.
[0078] In some embodiments, the unit dosage form comprises an admixture of (i) about 10 mg to about 680 mg (or about 10 mg to about 500 mg) of a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, wherein the specified weight is the free base moiety weight of the compound, (ii) a microcrystalline cellulose, and (iii) sodium stearyl fumarate. In some embodiments, the compound in the admixture is about 10 mg to about 500 mg, wherein the specified weight is the free base moiety weight of the compound.
[0079] In some embodiments, the unit dosage form is in the form of a capsule, and the admixture is contained in the capsule. In some embodiments, the unit dosage form comprises about 10 mg, about 20 mg, about 40 mg, about 100 mg, about 150 mg, about 200 mg, about 250 mg, about 300 mg, about 350 mg, about 400 mg, about 450 mg, about 500 mg, about 550 mg, about 600 mg, or about 650 mg of the compound, wherein the specified weight is the free base moiety weight of the compound. In some embodiments, the compound is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide dihydrochloride monohydrate. In some embodiments, the admixture comprises (i) about 10 mg (or about any of 40 mg, 100 mg, 200 mg, 300 mg, 400 mg, or 500 mg) of the compound, (ii) a microcrystalline cellulose, and (iii) sodium stearyl fumarate, wherein the specified weight is the free base moiety weight of the compound. In some embodiments, the compound is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide dihydrochloride monohydrate.
[0080] In some embodiments, the weight ratio of the compound to excipient (e.g., microcrystalline cellulose such as silicified microcrystalline cellulose) in the unit dosage form is between about 1:1.5 to about 1:15 (e.g., between about 1:5 to about 1:10, between about 1:5 to about 1:12, or between about 1:10 to about 1:15), wherein the weight of the compound is the free base moiety weight of the compound. In some embodiments, the weight ratio of the compound to lubricant (e.g., sodium stearyl fumarate) in the unit dosage form is between about 5:1 to about 50:1 (e.g., between about 5:1 to about 10:1, between about 5:1 to about 25:1, between about 5:1 to about 40:1, between about 7:1 to about 34:1, or between about 8:1 to about 34:1), wherein the weight of the compound is the free base moiety weight of the compound. In some embodiments, the microcrystalline cellulose is silicified microcrystalline cellulose. In some embodiments, the silicified microcrystalline cellulose is a combination of 98% microcrystalline cellulose and 2% colloidal silicon dioxide.
[0081] In some embodiments, the lubricant (e.g., sodium stearyl fumarate) is about 0.1% to about 10%, about 0.5% to about 5%, about 0.5% to about 3%, about 0.5% to about 2%, about 0.75% to about 1.5% of the capsule fill weight. In some embodiments, the lubricant (e.g., sodium stearyl fumarate) is at least about any one of 0.1%, 0.25%, 0.5%, 0.75%, 1%, 1.25%, 1.5%, 1.75%. 2%, 2.5%, 3%, 3.5%, 4%, 4.5%, or 5% of the capsule fill weight. In some embodiments, the lubricant (e.g., sodium stearyl fumarate) is about any one of 0.1%, 0.25%, 0.5%, 0.75%, 1%, 1.25%, 1.5%, 1.75%, 2%, 2.5%, 3%, 3.5%, 4%, 4.5%, or 5% of the capsule fill weight.
[0082] In some embodiments, the weight ratio of a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof to an excipient (e.g., microcrystalline cellulose such as silicified microcrystalline cellulose) in a capsule or unit dosage form is about 40:60 to about 10:90. In some embodiments, the weight ratio of the compound to an excipient (e.g., microcrystalline cellulose such as silicified microcrystalline cellulose) in a capsule ot unit dosage form is about any one of 95:5, 90:10, 85:15, 80:20, 75:25, 70:30, 65:35, 60:40, 55:45, 50:50, 45:55, 40:60, 35:65, 30:70, 25:75, 20:80, 15:85, 10:90, or 5:95. In some embodiments, the weight ratio of the compound to an excipient (e.g., microcrystalline such as silicified microcrystalline cellulose) is about 1:1.5 to about 1:9.5, such as about any of 1:1.5, 1:2, 1:2.5, 1:3, 1:3.5, 1:4, 1:4.5, 1:5, 1:5.5, 1:6, 1:6.5, 1:7, 1:7.5, 1:8, 1:8.5, 1:9, or 1:9.5. In some embodiments, the compound is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}- pyrimidin-4-yl)amino]benzenesulfonamide dihydrochloride monohydrate.
[0083] In some embodiments, the capsule contains about 5% to about 50% (e.g., about 5% to about 10% or about 5% to about 35%) compound of the total weight of the admixture, wherein the weight of the compound is the free base moiety weight of the compound. In some embodiments, the capsule contains about 40% to about 95% (e.g., about 50% to about 90% or about 60% to about 90%) microcrystalline cellulose (such as silicified microcrystalline cellulose) of the total weight of the admixture. In some embodiments, the capsule contains about 0.2% to about 5% (e.g., about 0.2% to about 2% or about 0.5% to about 1.5%, or about 0.5%, about 1%, or about 1.5%) sodium stearyl fumarate of the total weight of the admixture.
[0084] In some embodiments, the capsule or unit dosage form contains an admixture of about 12 mg of N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide dihydrochloride monohydrate, about 122 mg of silicified microcrystalline cellulose, and about 1 mg of sodium stearyl fumarate. In some embodiments, the capsule or unit dosage form contains an admixture of about 47 mg of N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide dihydrochloride monohydrate, about 448 mg of silicified microcrystalline cellulose, and about 5 mg of sodium stearyl fumarate. In some embodiments, the capsule or unit dosage form contains an admixture of about 117 mg of N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide dihydrochloride monohydrate. In some embodiments, the capsule or unit dosage form contains an admixture of about 235 mg of N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide dihydrochloride monohydrate, about 357 mg of silicified microcrystalline cellulose, and about 6.00 mg of sodium stearyl fumarate.
[0085] Also provided herein are oral solution formulations comprising a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof.
[0086] In some embodiments, the oral solution formulation further comprises methylcellulose. In some embodiments, the oral solution formulation further comprises methylcellulose and Tween 80. In some embodiments, the oral solution formulation comprises the compound at about 1 mg/ml to about 25 mg/ml, about 2 mg/ml to about 20 mg/ml, about 3 mg/ml to about 15 mg/ml, about 5 mg/ml to about 10 mg/ml. In some embodiments, the oral solution formulation comprises the compound at about any one of 2 mg/ml, 3 mg/ml, 4 mg/ml, 5 mg/ml, 6 mg/ml, 6.25 mg/ml, 6.5 mg/ml, 7 mg/ml, 8 mg/ml, 9 mg/ml, 10 mg/ml, or 12.5 mg/ml, or 15 mg/ml. In some embodiments, the oral solution formulation comprises about 0.1% to about 5%, 0.2% to about 3%, about 0.25% to about 2%, about 0.25% to about 1%, or about 0.5% by weight of methylcellulose. In some embodiments, the oral solution formulation comprises about 0.01% to about 0.5%, 0.02% to about 0.3%, about 0.025% to about 0.2%, about 0.025% to about 0.1%, or about 0.05% by weight of Tween 80.
[0087] In some embodiments, the capsule does not comprise an absorption enhancer. In some embodiments, the capsule comprises an absorption enhancer (e.g., Vitamin E TPGS, Gelucire 44/14. Pluronic F127, or glyceryl monostearate).
[0088] A capsule or unit dosage form provided may comprise one or more of the following properties: (1) upon administration to a subject such as human subject, the Cmax of the compound is achieved within about 2 to about 4 hours post-dose; (2) upon administration to a human subject, the elimination half life of the compound is about 16 to about 34 hours; (3) the mean AUC of the compound increases more than proportionally with increasing doses ranging from about 30 mg to about 800 mg per day; (4) the accumulation of the compound is about 1.25 to about 4.0 fold at steady state when the compound is dosed once daily.
[0089] Also provided are methods of preparing a capsule drug product comprising a) blending a lubricant with a compound that is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof to generate granules and b) mixing the granules of a) with an excipient. In some embodiments, the lubricant is sodium stearyl fumarate. In some embodiments, the excipient is microcrystalline cellulose such as silicified microcrystalline cellulose. Such method may be used to prepare a capsule or unit dosage form described herein. The weight (such as weight ratio or weight percentage) and components regarding the compound, excipient, and/or lubricant may be according to any described herein.
III. Methods of Treatment and Prevention of Myelofibrosis
[0090] Provided herein are methods for treating, delaying development, and/or preventing myelofibrosis in a subject comprising administering to the subject an effective amount of a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof (e.g., N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide dihydrochloride monohydrate). In some embodiments, the subject has myelofibrosis. In some embodiments, the subject is at risk of developing myelofibrosis. In some embodiments, the subject is a human subject. Any one of the formulations described herein such as capsule or unit dosage forms described herein may be used to treat a subject with myelofibrosis. In some embodiments, the compound is in an admixture of (i) a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, (ii) an excipient (such as microcrystalline cellulose), and (iii) a lubricant (such as sodium stearyl fumarate).
[0091] Myclofibrosis that may be treated by the compounds described herein includes primary myelofibrosis (MF) and secondary myelofibrosis (e.g., myelofibrosis arising from antecedent polycythemia vera (post-PV MF) or essential thrombocythemia (post-ET MF)). Myelofibrosis that may be treated by the compounds described herein also includes myelofibrosis of high risk, intermediate risk such as intermediate risk level 2. Methods for diagnosing various types of myelofibrosis are known in the art. See, e.g., Cervantes et al., Blood 2009. In some embodiments, the subject with myelofibrosis has spleen of at least 5 cm below costal margin as measured by palpation.
[0092] In some embodiments, the subject has a point mutation from valine 617 to phenylalanine in the Janus kinase 2 (JAK2 kinase) (JAK2V617F) if the subject is a human, or a point mutation corresponding to the valine 617 to phenylalanine in the Janus kinase 2 (JAK2 kinase) if the subject is not a human. In some embodiments, the subject is negative for the valine 617 to phenylalanine mutation of JAK2 if the subject is a human, or negative for a mutation corresponding to the valine 617 to phenylalanine in the Janus kinase 2 (JAK2 kinase) if the subject is not a human. Whether a subject is positive or negative for JAK2V617F can be determined by a polymerase chain reaction ("PCR") analysis using genomic DNA from bone marrow cells or blood cells (e.g., whole blood leukocytes). The PCR analysis can be an allele-specific PCR (e.g., allele-specific quantitative PCR) or PCR sequencing. See Kittur J et al., Cancer 2007, 109(11):2279-84 and McLornan D et al., Ulster Med J. 2006, 75(2):112-9, each of which is expressly incorporated herein by reference.
[0093] In some embodiments, the subject treated with the methods described herein has previously received another myelofibrosis therapy or treatment. In some embodiments, the subject is a non-responder to the other myelofibrosis therapy or has a relapse after receiving the other myelofibrosis therapy. The previous therapy may be a JAK2 inhibitor (e.g. INCB018424 (also known as ruxolitinib, available from Incyte), CEP-701 (lestaurtinib, available from Cephalon), or XL019 (available from Exelixis)) (See Verstovsek S., Hematology Am Soc Hematol Educ Program. 2009:636-42) or a non-JAK2 inhibitor (such as hydroxyurea). In some embodiments, the subject has received ruxolitinib treatment for primary myelofibrosis, post-polycythemia vera myelofibrosis (Post-PV MF), post-essential thrombocythemia myelofibrosis (Post-ET MF), polycythemia vera, or essential thrombocythemia for at least 14 days and discontinued the treatment for at least 30 days. In some embodiments, the previous therapy is a treatment with a compound described herein and the previous therapy has been discontinued upon indication of one or more elevated levels of amylase, lipase, aspartate aminotransferase (AST), alanine aminotransferase (ALT), and/or creatinine in the serum from the subject, and/or upon indication of a hematologic condition selected from the group consisting of anemia, thrombocytopenia, and neutropenia. In some embodiments, the dose of the compound in the second treatment is the same or lower than the dose in the previous therapy.
[0094] The subject may be treated orally and/or daily. The subject (such as a human) may be treated by administering at a dose of about 240 mg per day to about 680 mg per day (or about 300 mg per day to about 500 mg per day), wherein the specified weight is the free base moiety weight of the compound. In some embodiment, the compound is administered at a dose of about any of 240 mg/day, 250 mg/day, 300 mg/day. 350 my/day, 400 mg/day, 450 mg/day, 500 mg/day, 550 mg/day, 600 mg/day, 650 mg/day, or 680 mg/day. The compound may be in a capsule and/or a unit dosage form described herein. In some embodiments, the compound administered is in an admixture with a microcrystalline cellulose and sodium stearyl fumarate, and the admixture is in a capsule. In some embodiments, the compound is administered orally.
[0095] Also provided herein are methods for ameliorating one or more symptoms associated with myelofibrosis. For example, the treatment using the compound described herein is effective in reducing spleen size, ameliorating constitutional symptoms (such as early satiety, fatigue, night sweats, cough, and pruritus), reducing leukocytosis, reducing thrombocytosis, decreasing JAK2V617F allele burden, reducing bone marrow fibrosis, improving pruritus, improving cachexia, and/or reducing bone marrow cellularity. The reduction, decrease, amelioration, or improvement can be at least by 5, 10, 20, 30, 40, 50, 60, 70, 80, or 90% compared to the level prior to commencing treatment with the compound provided herein. In some embodiment, the spleen becomes non-palpable in the subject after treatment. In some embodiments, the subject has complete resolution of leukocytosis and/or thrombocytosis after treatment. In some embodiments, the subject has complete resolution of pruritus after treatment.
[0096] In some embodiments, the compound is administered to the subject daily for at least 1 cycle, at least 2 cycles, at least 3 cycles, at least 4 cycles, at least 5 cycles, or at least 6 cycles of a 28-day cycle. In some embodiments, the compound is administered to the subject daily for at least 6 cycles of a 28-day cycle, at least 8 cycles of a 28-day cycle, at least 10 cycles of a 28-day cycle, at least 12 cycles of a 28-day cycle, at least 15 cycles of a 28-day cycle, at least 18 cycles of a 28-day cycle, or at least 24 cycles of a 28-day cycle. In some embodiments, the compound is administered to the subject daily for at least one month, at least two month, at least three month, at least four month, at least five month, at least six month, at least eight month, or at least one year. In some embodiments, the compound is administered once a day.
[0097] In some embodiments, upon administration of a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof to a subject such as human subject, the Cmax of the compound is achieved within about 1 to about 5 hours, about 1.5 to about 4.5 hours, about 2 to about 4 hours, or about 2.5 to about 3.5 hours post-dose. In some embodiments, upon administration of the compound to a human subject, the elimination half life of the compound is about 12 to about 40 hours, about 16 to about 34 hours, or about 20 to about 30 hours. In some embodiments, the mean AUC of the compound increases more than proportionally with increasing doses ranging from about 30 mg to about 800 mg per day. In some embodiments, the accumulation of the compound is about 1.1 to about 5 fold, about 1.25 to about 4.0 fold, about 1.5 to about 3.5 fold, about 2 to about 3 fold at steady state when the compound is dosed once daily.
[0098] In some embodiments, the method comprises instructing the subject to ingest the effective amount of the compound on an empty stomach. In some embodiments, the methods further comprise instructing the subject to avoid ingesting agents that are at least moderate inducers or inhibitors of CYP3A4. In some embodiments, the subject does not receive concomitant treatment with or use of drugs to herbal agents known to be at least moderate inhibitors or inducers of CYP3A4. Based on in vitro evaluations, N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide is metabolized by human CYP3A4. Agents that may increase N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide plasma concentrations (i.e., CYP3A4 inhibitors) or decrease N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide plasma concentrations (i.e., CYP3A4 inducers), including herbal agents and foods (e.g. grapefruit/grapefruit juice), should be avoided in subjects being treated as described herein. In addition, in vitro data have indicated that N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide inhibits CYP3A4 in a time-dependent fashion. Agents that are sensitive substrates for metabolism by CYP3A4 should be used with caution as coadmninistration with N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide may result in higher plasma concentrations of the coadministered agent. A list of clinically relevant substrates of CYP3A4 include alfentanil, Cyclosporine, Diergotamine, ethinyl estradiol, ergotamine, fentanyl, pimozide, quinidine, sirolimus, tacrolimus, clarithromycin erythromycin, telithromycin, alprazolam, diazepam, midazolamn, triazolam, indinavir, ritonavir, saquinavir, prokinetic, cisapride, astemizole, chlorpheniramine, amlodipine, diltiazem, felodipine, nifedipine, verapamil, atorvastatin, cerivastatin, lovastatin, simvastatin, aripiprazole, gleevec, halopericol, sildenafil, tamoxifcn, taxanes, trazodonc, and Vincristinc. A list of clinically relevant inducers of CYP3A4 include carbamazepine, phenobarbital, phenytoin, pioglitazone, rifabutin, rifampin, St. John's wort, and troglitazone. A list of clinically relevant inhibitors of CYP3A4 include indinavir, nelfinavir, ritonavir, clarithromycin, itraconazole, ketoconazole, nefazodone, erythromycin, grapefruit juice, verapamil, diltiazem, cimetidine, amniodarone, fluvoxamine, mibefradil, and Troleandomycin. See reference Flockhart et al., http://nedicine.iupui.edu/clinpharnn/ddis/clinicaltable.aspx., 2009.
[0099] Also provided herein are methods of monitoring treatment of myelofibrosis to a subject, comprising (a) administering to the subject an effective amount of a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof; (b) monitoring a hematologic parameter and/or a non-hematologic parameter in the subject; and (c) determining if the subject should continue or discontinue with the treatment. In some embodiments, the hematologic parameter is selected from the group consisting of anemia, thrombocytopenia, and neutropenia. In some embodiments, the non-hematologic parameter is an enzyme or molecule in the blood or serum wherein an elevated level of the enzyme or molecule is indicative of tissue or organ damage. In some embodiments, the serum enzyme or molecule can be, for example, amylase, lipase, aspartate aminotransferase (AST), alanine aminotransferase (ALT), creatinine, alkaline phosphatase, and calcium. Methods of monitoring these parameters are known in the art and are described herein. See Examples 1-3. In some embodiments, the method further comprises administering to the subject an effective amount of the compound described herein after the subject has been discontinued with the treatment for at least 2 week, at least 3 weeks, or at least 4 weeks. In some embodiments, the previous treatment has been discontinued without prior dose reduction.
[0100] Also provided herein are methods of monitoring treatment of myelofibrosis to a subject, comprising administering to the subject an effective amount of a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, and discontinuing the treatment upon indication of elevated levels of one or more enzymes or molecules selected from the group consisting of amylase, lipase, aspartate aminotransferase (AST), alanine aminotransferase (ALT), and creatinine and/or decreased level of calcium in the blood or serum of the subject without prior dose reduction. Also provided herein are methods of monitoring treatment of myelofibrosis to a subject, comprising administering to the subject an effective amount of a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzensulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, and discontinuing the treatment upon indication of one or more hematologic conditions selected from the group consisting of anemia, thrombocytopenia, and neutropenia without prior dose reduction. In some embodiments, the treatment is discontinued when one or more of the parameters (including hematologic and non-hematologic parameters) are grade 3 or 4 events.
[0101] Grade 3 or 4 adverse events for hematologic and non-hematologic parameters are known in the art and shown in the Table below. See, e.g. C Common Terminology Criteria for Adverse Events (CTCAE), Version 4.0, Published: May 28, 2009 (v4.03: Jun. 14, 2010).
TABLE-US-00001 RESPONSE (hematologic and non- hematologic) Definition Grade 3 Grade 4 Hyperlipasemia A finding based on >2.0-5.0 .times. ULN* >5.0 .times. ULN laboratory test results that indicate an increase in the level of lipase in a biological specimen. Serum amylase A finding based on >2.0-5.0 .times. ULN >5.0 .times. ULN laboratory test results that indicate an increase in the levels of amylase in a serum specimen. Alanine A finding based on >5.0-20.0 .times. ULN >20.0 .times. ULN aminotransferase laboratory test results that increased indicate an increase in the level of alanine aminotransferase (ALT or SGPT) in the blood specimen. Aspartate A finding based on >5.0-20.0 .times. ULN >20.0 .times. ULN aminotransferase laboratory test results that increased indicate an increase in the level of aspartate aminotransferase (AST or SGOT) in a blood specimen. Blood creatinine A finding based on >3.0 baseline; >3.0 6.0 .times. ULN >6.0 .times. increased laboratory test results that ULN indicate increased levels of creatinine in a biological specimen. Blood alkaline A finding based on >5.0-20.0 .times. ULN >20.0 .times. ULN phosphatase increased laboratory test results that indicate an increase in the level of alkaline phosphatase in a blood specimen. Hypocalcemia A disorder characterized Corrected serum Corrected serum by laboratory test results calcium of calcium of that indicate a low <7.0-6.0 mg/dL; <6.0 mg/dL; <1.5 mmol/L; concentration of calcium <1.75-1.5 mmol/L; Ionized calcium (corrected for albumin) in Ionized <0.8 mmol/L; the blood. calcium <0.9-0.8 mmol/L; life-threatening hospitalization consequences indicated Anemia A disorder characterized Hgb <8.0 g/dL; <4.9 mmol/L; Life-threatening by a reduction in the <80 g/L; transfusion consequences; amount of hemoglobin in indicated urgent intervention 100 ml of blood. Signs indicated and symptoms of anemia may include pallor of the skin and mucous membranes, shortness of breath, palpitations of the heart, soft systolic murmurs, lethargy, and fatigability. Thrombocytopenia a platelet count below the 25,000 to <50,000/.mu.L below 25,000/.mu.L normal range for the population ([+ or -] 2 standard deviations). In most laboratories, a normal platelet count is between 150,000 to 450,000/.mu.L Neutropenia A finding based on <1000-500/mm3; <1.0-0.5 .times. <500/mm3; <0.5 .times. laboratory test results that 10.sup.9/L 10.sup.9/L indicate a decrease in number of neutrophils in a blood specimen. * "ULN" refers to upper limit of normal.
IV. Articles of Manufactures and Kits
[0102] Also provided herein are articles of manufacture or kits containing a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof. In some embodiments, the article of manufacture or the kit further includes instructions for using the compounds described herein in the methods provided herein. In some embodiments, the article of manufacture or the kit further comprises a label or a package insert providing the instructions. In some embodiments, the compound is in a capsule and/or a unit dosage form described herein.
[0103] In some embodiments, the article of manufacture or kit may further comprise a container. Suitable containers include, for example, bottles, vials (e.g., dual chamber vials), syringes (such as single or dual chamber syringes) and test tubes. The container may be formed from a variety of materials such as glass or plastic, and the container may hold the compound, for example in the formulation to be administered. The article of manufacture or the kit may further comprise a label or a package insert, which is on or associated with the container, may indicate directions for reconstitution and/or use of the compound. In some embodiments, the package insert or the label is in a position which is visible to prospective purchasers.
[0104] The label or package insert may further indicate that the compound is useful or intended for treating or preventing myelofibrosis in a subject. In some embodiments, the package insert or the label indicates that the compound can be used for ameliorating bone marrow cellularity and/or bone marrow fibrosis. In some embodiments, the package insert or the label indicates that the compound can be used for treating myelofibrosis in a subject, wherein the subject is negative for the valine 617 to phenylalanine mutation of human JAK2 (JAK2V617F) or negative for the mutation corresponding to the valine 617 to phenylalanine mutation of human JAK2. In some embodiments, the package insert or the label indicates that the compound can be used for treating myelofibrosis in a subject, and that subject should discontinue the treatment upon indication of elevated levels of one or more of amnylase, lipase, aspartate aminotransferase (AST), alanine aminotransferase (ALT), creatinine, and/or alkaline phosphatase and/or decreased level of calcium in the serum of the subject, and/or upon indication of one or more of anemia, thrombocytopenia, and/or neutropenia. In some embodiments, the package insert or the label further indicates that the compound can be discontinued without prior dose reduction.
[0105] In some embodiments, there is provided a kit or article of manufacture comprising (a) an admixture of (i) a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, (ii) excipient (e.g., microcrystalline cellulose such as silicified microcrystalline cellulose), and (iii) lubricant (e.g., sodium stearyl fumarate), and (b) a package insert or a label indicating that the admixture is useful for treating myelofibrosis in a subject. In some embodiments, there is provided a kit or article of manufacture comprising (a) a compound which is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutical salt thereof or a hydrate thereof, and (b) a package insert or a label indicating that the compound can be used for treating myelofibrosis in a subject, wherein the subject has previously received another myelofibrosis therapy with a JAK2 inhibitor which is not N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof.
[0106] In some embodiments, the package insert or a label indicates that, upon administration of the compound to a human subject, the Cmax of the compound is achieved within about 1 to about 5 hours, about 1.5 to about 4.5 hours, about 2 to about 4 hours, or about 2.5 to about 3.5 hours post-dose. In some embodiments, the package insert or a label indicates that, upon administration of the compound to a human subject, the elimination half life of the compound is about 12 to about 40 hours, about 16 to about 34 hours, or about 20 to about 30 hours. In some embodiments, the mean AUC of the compound increases more than proportionally with increasing doses ranging from about 30 mg to about 800 mg per day. In some embodiments, the accumulation of the compound is about 1.1 to about 5 fold, about 1.25 to about 4.0 fold, about 1.5 to about 3.5 fold, about 2 to about 3 fold at steady state when the compound is dosed once daily.
[0107] In some embodiments, the package insert or the label instructs the subject to ingest the effective amount of the compound on an empty stomach. In some embodiments, the package insert or the label instructs the subject to avoid ingesting agents that are at least moderate inducers or inhibitors of CYP3A4. In some embodiments, the inducer or inhibitor of CYP3A4 is any one of the inducers or inhibitors of CYP3A4 described herein.
[0108] Also provided are uses of a compound in the manufacture of a medicament for treating myelofibrosis in a subject, wherein the compound is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}- pyrimidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof. In some embodiments, the use is according to a method described herein. In some embodiments, the compound is in an admixture of (i) the compound, (ii) an excipient (e.g., microcrystalline cellulose such as silicified microcrystalline cellulose), and (iii) a lubricant (e.g., sodium stearyl fumarate). In some embodiments, the compound is administered orally. In some embodiments, the use is according to a method described herein. In some embodiments, there is provided use of a compound in the manufacture of a medicament for treating myelofibrosis in a subject, wherein the compound is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}- pyrimidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, wherein the subject is negative for the valine 617 to phenylalanine mutation of human Janus Kinase 2 (JAK2) or negative for the mutation corresponding to the valine 617 to phenylalanine mutation of human JAK2. In some embodiments, there is provided use of a compound in the manufacture of a medicament for treating myelofibrosis in a subject, wherein the compound is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, wherein the subject has previously received another myelofibrosis therapy. In some embodiments, the previous therapy comprises a JAK2 inhibitor which is not N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof.
[0109] Also provided is a compound for treating myelofibrosis in a subject, wherein the compound is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof. In some embodiments, the treatment is according to a method described herein. In some embodiments, the compound is in an admixture of (i) the compound, (ii) an excipient (e.g., microcrystalline cellulose such as silicified microcrystalline cellulose), and (iii) a lubricant (e.g., sodium stearyl fumarate). In some embodiments, the compound is administered orally. In some embodiments, the treatment is according to a method described herein. In some embodiments, there is provided a compound for treating myelofibrosis in a subject, wherein the compound is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, wherein the subject is negative for the valine 617 to phenylalanine mutation of human Janus Kinase 2 (JAK2) or negative for the mutation corresponding to the valine 617 to phenylalanine mutation of human JAK2. In some embodiments, there is provided a compound for treating myelofibrosis in a subject, wherein the compound is N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof, wherein the subject has previously received another myelofibrosis therapy. In some embodiments, the previous therapy comprises a JAK2 inhibitor which is not N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide or a pharmaceutically acceptable salt thereof or a hydrate thereof.
[0110] The following are examples of the methods and compositions provided herein. It is understood that various other embodiments may be practiced, given the general description provided above.
EXAMPLES
Example 1 Evaluation of TG101348 in Myelofibrosis
[0111] As used herein, "TG101348" refers to N-tert-butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide dihydrochloride monohydrate. The subjects in this study were administered with capsule form of TG101348 as described in Example 5. TG101348 was evaluated in a Phase I study for the treatment of myelofibrosis. This study was ongoing at the time the data were collected.
[0112] Background:
[0113] TG101348 is a potent, orally bioavailable, JAK2-selective small molecule inhibitor, that was evaluated in a Phase I study for the treatment of myelofibrosis. The dose-limiting toxicity was asymptomatic grade 3 or 4 amylasemia/lipasemia that was reversible, and the maximum tolerated dose ("MTD") was 680 mg. The most frequent non-hematological toxicities were mild nausea, vomiting, and/or diarrhea that were easily controlled or resolved spontaneously. Grade 3/4 neutropenia and thrombocytopenia were observed in 14% and 25% of patients, respectively. TG101348 had activity in reducing spleen size, leukocyte count, and JAK2V617F ("VF") allele burden. This example describes the results with a focus on the data from the dose confirmation cohort who initiated treatment at a dose of 680 mg/day.
[0114] Results:
[0115] Fifty nine patients (median age=66 years; range 43-86) were treated--28 in the dose escalation phase, and 31 in the dose confirmation phase. Overall, 44 patients had PMF, 12 post-PV MF, and 3 post-ET MF; 86% were VF-positive. Median palpable spleen size was 18 cm and 22 patients were red blood cell ("RBC") transfusion-requiring at study enrollment. After a median follow-up of 12 weeks (range <1-76), 18 (31%) patients discontinued treatment due to toxicity (n=7; thromnbocytopenia=3, neutropenia=1), comorbidities (n=5), withdrawal of consent (n=4), or non-compliance/lack of response (1 each). The remaining 41 patients were at the following dose levels when the data in this example were collected: 680 mg (n=14), 520-600 mg (n=16), 360-440 mg (n=10), and 240 mg (n=1). The cumulative drug exposure to the time when the data in this example were collected was 362 patient-months; exposure at or above MTD (680 mg) was 154 patient-months. Forty patients (68%) started treatment at .gtoreq.680 mg.
[0116] Toxicity:
[0117] TG101348 was well tolerated. Of the patients who started at .gtoreq.680 mg, Gr3/4 neutropenia was observed in 15/0% and Gr3/4 thrombocytopenia in 20/10%. Twenty four (60%) patients did not require RBC transfusions at baseline (median hemoglobin ("Hgb")=9.6 g/dL; range 7.4-13.1); of these, 42% and 8% of patients developed Grade 3 ("Gr3") and Grade 4 ("Gr4") anemia, respectively. The majority of patients who started at .gtoreq.680 mg developed mild nausea (1 Gr3), vomiting (1 Gr3), and/or diarrhea (3 Gr3) that were self-limited or easily controlled. Other non-hematological toxicities included Grade 1/2 ("Gr1/2") transaminitis (38%). Gr1/2 serum creatinine elevation (38%), and asymptomatic hyperlipasemia (33%).
[0118] Efficacy:
[0119] Thirty three patients who started at .gtoreq.680 mg completed at least 3 cycles of treatment: at 3 months, reduction in palpable spleen size (baseline median=18 cms; range 6-32) was at least 50% in 22 (67%) patients; the spleen became non-palpable in 9 (27%) patients. All 21 patients with leukocytosis at baseline (WBC range 11 to 203.times.10.sup.9/L) who started at 2680 mg experienced a marked reduction in their WBC count (range 4 to 90); 70% had a normal WBC count at their last follow-up visit. Overall, 48 of the 51 VF-positive patients completed at least 1 cycle and were evaluable for response in VF allele burden; at last available follow-up, the median decrease in granulocyte mutant allele burden was 48%; 21 (44%) patients had a 250% reduction, and in the group who started treatment at >680 mg, 48% have had a 250% reduction. Of those evaluable, there was clinically significant benefit or resolution of constitutional symptoms, including early satiety, fatigue, cough, pruritus, and night sweats.
[0120] Conclusions:
[0121] TG101348 was well tolerated in patients with myelofibrosis. Spleen and leukocyte responses were frequent, observed early, and produced substantial clinical benefit for patients. These responses were associated with significant decrease in VF allele burden and pointed to activity of TG101348 against the malignant clone in myelofibrosis.
Example 2 Evaluation of TG101348 in Myelofibrosis
[0122] The subjects in this study were administered with capsule form of TG101348. TG101348 was evaluated in a Phase I study for the treatment of myelofibrosis. This study is also described in Example 1. This example describes data available at the time of data collection.
[0123] This study was an open-label, multicenter, and dose-escalation study with expanded cohort dose confirmation at MTD. The primary objective of this study was to determine safety/tolerability, DI T, MTD, and pharmacokinetics of TG101348 in subjects with MF. The secondary objective of this study was to evaluate preliminary clinical and pharmacodynamic activity.
[0124] The key eligibility criteria for subjects included: Myelofibrosis (PMF or post-PV/ET MF); High-risk or intermediate-risk with symptomatic splenomegaly/unresponsive to available therapy; ECOG performance status .ltoreq.2; ANC .gtoreq.1.times.10.sup.9/L; Platelet count .gtoreq.250.times.10.sup.9/L; Serum creatinine .ltoreq.2 mg/dL; Total bilirubin .ltoreq.2 mg/dL; AST/ALT .ltoreq.3.times. upper limit of normal.
[0125] The subject disposition for this study is included in Table 1.
TABLE-US-00002 TABLE 1 Subject Disposition MTD* Overall Enrolled 40 59 Included in safety analysis 40 59 Included in drug activity analysis 37 55 Discontinued 11 (28%) 15 (25%) Reasons for discontinuation Adverse event 5 6 Subject withdrew consent 4 6 Investigator discretion 2 3 Median (range) treatment 24 weeks 24 weeks duration (1-24 weeks) (0.3-84 weeks)** *Includes all subjects who initiated treatment at 680 or 800 mg/day. **Includes continued treatment in extension study.
[0126] The demographic and baseline characteristics for the subjects are included in Table 2.
TABLE-US-00003 TABLE 2 Demographic and Baseline Characteristics MTD Overall (n = 40) (N = 59) Age (median; years) 65 (43-85) 64 (43-85) Male 22 (55%) 34 (58%) JAK-2.sup.V617F positive 35 (88%) 51 (86%) PMF 31 (78%) 44 (75%) Post-PV MF 6 (15%) 12 (20%) Post-ET MF 3 (8%) 3 (5%) High risk 20 (50%) 26 (44%) Palpable splenomegaly 39 (98%) 58 (98%) Transfusion dependent 16 (40%) 22 (37%)
[0127] This study was a dose-escalation study with expanded cohort dose confirmation at MTD. Below describes the data with a focus on the dose confirmation cohort who initiated treatment at a dose of 680 mg/day.
[0128] The decrease in palpable spleen size by cycle for subjects treated with TG101348 680 mg/day (starting dose) (N=37) is shown in FIG. 1. The baseline spleen size was: median=18 cm; range=6-32 cm. 49% of subjects achieved clinical improvement based on reduction of palpable splenomegaly (IWG response) (56% of subjects by 12 weeks; 100% of subjects by 20 weeks). There was no relapse or disease progression at the time of data collection.
[0129] The effect of TG101348 on leukocytosis is shown in FIG. 2. The baseline WBC count was >11.times.10.sup.9/L. 73% of subjects had normal WBC counts at their follow-up visit. The effect of TG101348 on thrombocytosis is shown in FIG. 3 (baseline platelet count >450.times.10.sup.9/L). TG101348 was able to reduce platelet counts. The effects of TG101348 on constitutional symptoms (baseline versus last visit) are shown in FIG. 4. TG101348 was able to improve the MF-associated constitutional symptoms. TG101348 had no significant changes on cytokine levels (see FIG. 5, all values shown are medians). FIG. 6 shows the effect of TG101348 on V617F allele burden in subjects with baseline >20% (N=22). FIG. 6 shows that TG101348 was able to decrease JAK2 V617F allele burden in 59% of the subjects with baseline >20%.
[0130] FIG. 7 shows the effects of TG1101348 on bone marrow cellularity in a 76-year-old male with V617F negative PMF. The starting dose was 30 mg/day and the dose at follow-up was 520 mg/day. FIG. 7 shows that TG101348 was able to reduce bone marrow cellularity in this subject from 60% bone marrow cellularity at baseline to 5-10% bone marrow cellularity after 18 cycles. FIG. 8 shows the effect of TG1101348 on bone marrow fibrosis in a 56-year-old male with V617F negative PMF. The starting dose was 240 mg/day and the dose at follow-up was 440 mg/day. FIG. 8 shows that TG101348 was able to reduce bone marrow fibrosis in this subject from 3+ at baseline to 0 after 18 cycles.
[0131] The treatment-emergent grade 3 & 4 hematologic toxicities in MTD Subjects (N=40) is shown in Table 3. The treatment-emergent non-hematologic adverse events (reported for at least 5 subjects) in MTD Subjects (N=40) is shown in Table 4.
TABLE-US-00004 TABLE 3 Treatment-Emergent Grade 3 & 4 Hematologic Toxicities in MTD Subjects (N = 40) Anemia Neutropenia Thrombocytopenia (N = 24)* (N = 40) (N = 40) New Transfusion Grade 3 Grade 4 Grade 3 Grade 4 Requirement on Study.dagger-dbl. 6 (15%) 0 8 (20%) 5 (13%) 16 (67%) *Subjects who were not transfusion dependent at baseline. .dagger-dbl.Transfusion on at least 2 occasions for hemoglobin ("Hb") <10 g/dL.
TABLE-US-00005 TABLE 4 Treatment-Emergent Non-Hematologic Adverse Events in MTD Subjects (N = 40) Event Grade 1 Grade 2 Grade 3 Grade 4 Gastrointestinal disorders Diarrhea 21 (53%) 4 (10%) 5 (13%) 0 Nausea 20 (50%) 6 (15%) 2 (5%) 0 Vomiting 20 (50%) 7 (18%) 1 (3%) 0 Constipation 6 (15%) 1 (3%) 0 0 Abdominal pain 5 (13%) 0 0 0 Other Anorexia 7 (18%) 0 1 (3%) 0 Edema peripheral 7 (18%) 1 (3%) 0 0 Fatigue 2 (5%) 3 (8%) 1 (3%) 0 Contusion 5 (13%) 0 0 0 Headache 4 (10%) 1 (3%) 0 0 Proteinuria 2 (5%) 3 (8%) 0 0
[0132] The grade .gtoreq.2 treatment-emergent non-hematologic laboratory findings in MTD subjects (N=40) is shown in Table 5.
TABLE-US-00006 TABLE 5 Grade .gtoreq. 2 Treatment-Emergent Non-Hematologic Laboratory Findings in MTD Subjects (N = 40) Finding Grade 2 Grade 3 Grade 4 Creatinine increased 11 (28%) 0 0 Hypocalcemia 8 (20%) 3 (8%) 0 AST increased 5 (13%) 1 (3%) 0 ALT increased 8 (20%) 2 (5%) 0 Hyperkalemia 3 (8%) 2 (5%) 1 (3%) Hyperlipasemia 4 (10%) 3 (8%) 2 (5%) Hyperamylasemia 0 1 (3%) 1 (3%)
Laboratory findings were transient and reversible, and resolved spontaneously or following dose interruption and/or reduction.
[0133] FIG. 9 shows various measurements in a subject with JAK2V617F-positive PMF that started at TG101348 680 mg/day. TG101348 was able to reduce the palpable spleen size from 9 cm to 0 cm and led to complete resolution of pruritus in this subject.
[0134] Conclusions:
[0135] TG101348 was generally well tolerated, with manageable, grade 1 gastrointestinal effects, especially at higher doses. The data indicated no long-term toxicities. The expected on-target myelosuppressive effect appeared to be mostly limited to erythropoiesis, which may be attenuated at lower, but still effective, doses. TG101348 had remarkable activity in MF-associated splenomegaly: .about.two-thirds achieved >50% reduction in palpable splenomegaly; .about.30% had complete response. TG101348 had significant anti-myeloproliferation activity with virtually all treated subjects experiencing complete resolution of leukocytosis and thrombocytosis. TG101348 had remarkable activity against MF-associated constitutional symptoms, pruritus and cachexia. TG101348 induced a significant decrease in JAK2V617F allele burden in a substantial proportion of treated subjects. TG101348 had minimal effect on serum levels of proinflammatory cytokines; this was consistent with the absence of immediate adverse cytokine-rebound phenomenon upon study drug discontinuation. Without wishing to be bound by any theory, the activity of TG01348 appeared to be a direct consequence of its JAK2 inhibitory activity and not an indirect effect from non-specific anti-cytokine activity. Furthermore, the preliminary observations showed reduction in BM cellularity and reticulinfibrosis with extended treatment.
Example 3 Evaluation of TG101348 in Myelofibrosis
[0136] The subjects in this study were administered with capsule form of TG101348.
[0137] Study Design:
[0138] The study constituted a Phase 1, dose-escalation trial (M-TG101348-001). This study is also described in Examples 1 and 2. Study eligible patients were >18 years of age with high- or intermediate-risk primary myelofibrosis (PMF), post-PV MF, or post-ET MF (Tefferi A et al., Leukemia 22:14-22, 2008). Additional eligibility criteria and participating centers are listed in Table 6. All patients provided written informed consent. The primary endpoints were determination of safety and tolerability, dose-limiting toxicity ("DLT"), maximum tolerated dose ("MTD") and pharmacokinetic ("PK") behavior of TG101348. The secondary endpoint was assessment of therapeutic activity.
TABLE-US-00007 TABLE 6 Detailed enrollment criteria for MF-TG101348-001 Inclusion Criteria Exclusion Criteria 1. Diagnosis of MF (PMF, post-PV MF, or 1. Any chemotherapy, immunomodulatory post-ET MF) according to the revised WHO drug therapy, immunosuppressive therapy, criteria.* corticosteroids > 10 mg/day prednisone or equivalent, or growth factor treatment within 14 days (28 days in the case of darbepoetin) prior to initiation of TG101348. 2. High-risk MF (defined by Mayo PSS), or 2. Major surgery or radiation therapy within Mayo PSS intermediate-risk MF** 28 days prior to initiation of TG101348. accompanied by symptomatic splenomegaly and/or unresponsive to available therapy. 3. At least 18 years of age. 3. Concomitant treatment with agents known to inhibit or induce CYP3A4, unless approved by the sponsor. 4. Body weight .gtoreq. 50 kg. 4. Known hypersensitivity to any ingredients in the study drug formulation. 5. ECOG performance status .ltoreq. 2. 5. Active infection requiring antibiotics. 6. Within 4 days prior to initiation of 6. Uncontrolled CHF (NYHA Classification 3 TG101348: or 4), angina, MI, CVA, coronary/peripheral ANC .gtoreq. 1 .times. 10.sup.9/L artery bypass graft surgery, TIA, or pulmonary Platelet count .gtoreq. 50 .times. 10.sup.9/L embolism within 3 months prior to initiation of Serum creatinine .ltoreq. 2.0 mg/dL study drug. Total bilirubin .ltoreq. 2.0 mg/dL AST or ALT .ltoreq. 3 times the ULN (unless clinically compatible with hepatic EMH) 7. Life expectancy .gtoreq. 12 weeks. 7. Cardiac dysrhythmias requiring ongoing treatment, bundle branch block on ECG or QRS duration > 120 ms, or prolongation of the QTc (Fridericia) interval to > 450 ms for males or > 470 ms for females. 8. Negative serum pregnancy test result for 8. Pregnant or lactating females. women of childbearing potential. 9. Absence of active malignancy other than 9. Women of childbearing potential, unless MF, with the exception of adequately treated surgically sterile for at least 3 months (i.e., basal cell carcinoma and squamous cell hysterectomy), postmenopausal for at least 12 carcinoma of the skin. months (FSH > 30 U/mL), unless they agree to use effective, dual contraceptive methods (i.e., oral, injectable, or barrier method with male partner using a condom) while on study drug. 10. Provide written informed consent to 10. Men who partner with a woman of participate. childbearing potential, unless they agree to use effective, dual contraceptive methods (i.e., a condom, with female partner using oral, injectable, or barrier method) while on study drug. 11. Willing to comply with scheduled visits, 11. Known HIV- or AIDS-related illness. treatment plans, laboratory assessments, and 12. Clinically active hepatitis B or C. other study-related procedures. 13. Any severe, acute or chronic medical, neurological, or psychiatric condition or laboratory abnormality that may increase the risk associated with study participation or study drug administration, may interfere with the informed consent process and/or with compliance with the requirements of the study, or may interfere with the interpretation of study results and, in the investigator's opinion, would make the patient inappropriate for entry into this study. Abbreviations: AIDS = acquired immunodeficiency syndrome; ALT = alanine aminotransferase; ANC = absolute neutrophil count; AST = aspartate aminotransferase; CHF = congestive heart failure; CVA = cerebrovascular accident; ECG = electrocardiogram; ECOG = Eastern Cooperative Oncology Group; EMH = extramedullary hematopoiesis; FSH = follicle stimulating hormone; HIV = human immunodeficiency virus; MF = myelofibrosis; MI = myocardial infarction; NYHA = New York Heart Association; PSS = prognostic scoring system; TIA = transient ischemic attack; WBC = white blood cell. *Tefferi and Vardiman. Leukemia. 2008 Jan; 22(1): 14-22 **High-risk disease requires two and intermediate-risk disease requires one of the following prognostic factors: hemoglobin < 10 g/dL, WBC count <4 or> 30 .times. 10.sup.9/L, platelet count < 100 .times. 10.sup.9/L, absolute monocyte count .gtoreq. 1 .times. 10.sup.9/L.
[0139] Patients were assigned to one of 8 dose cohorts, ranging from 30 to 800 mg per day, using standard 3+3 cohort design. TG101348 was administered orally once daily, with a treatment plan for continuous daily therapy for 24 weeks (6.times.28-day cycles). Intra-subject dose escalation was permitted after completion of at least 3 cycles of treatment at the starting dose. Once DLT was identified, a dose-confirmation cohort initiated treatment at the MTD. Treatment beyond 6 cycles was allowed on an extension study (MF-TG101348-002; NCT00724334) if deemed beneficial to the patient and if well tolerated.
[0140] Assessment of Toxicity and Response:
[0141] Safety assessments were performed weekly during cycle 1, every other week during cycles 2 and 3, and every 4 weeks thereafter. Toxicity was graded in accordance with the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE) version 3.0.
[0142] Responses were measured every 4 weeks per International Working Group for MPN Research and Treatment (IWG-MRT) criteria (Tefferi A et al., Blood 108:1497-1503, 2006). Assessment of bone marrow histology was performed at baseline and every 24 weeks of therapy. Changes in JAK2V617F allele burden in the granulocyte fraction of peripheral blood were measured as previously described (Kittur J et al., Cancer 109:2279-2284, 2007); the assessments were at baseline and every 4 weeks during the first 6 cycles, and every 6.sup.th cycle of therapy in the extension study.
[0143] Pharmacokinetics:
[0144] The concentration-time curves of TG101348 in plasma were evaluated by a non-compartmental analysis (with the use of WinNonlin.RTM. software, version 5.2).
[0145] Cytokine Assessment:
[0146] Samples for cytokine measurement were collected at baseline and every 4 weeks thereafter. Cytokine levels were measured using multiplexed sandwich ELISAs (Millipore, St. Charles, Mo.).
Results
[0147] Enrollment of Patients:
[0148] A total of 59 subjects were enrolled; 28 in the dose-escalation phase and 31 in the dose-confirmation phase (Table 7). Forty-four subjects had PMF, 12 post-PV MF, and 3 post-ET MF; 86% were JAK2V617F-positive. The median duration of disease was 3.4 years (range 0.06 to 25.8). At study enrollment, the median palpable spleen size was 18 cm below the left costal margin (83% had a palpable spleen size >10 cm), median hemoglobin level was 9.2 g/dL. (range 6.6 to 15.2) and 21 (36%) subjects were red cell transfusion-dependent by IWG-MRT criteria.
TABLE-US-00008 TABLE 7 Demographic and Baseline Subject Characteristics TG101348 Starting Dose (mg/day) MTD All 30 60 120 240 360 520 680 800 Cohort Doses Characteristic n = 4 n = 3 n = 3 n = 3 n = 3 n = 3 n = 34 n = 6 n = 40 n = 59 Age - years 63.5 64.0 63.0 68.0 66.0 57.0 63.5 69.0 65.1 (10.47).dagger. .sup. 64.5 (9.70).dagger. .sup. Range 55-76 56-66 53-71 55-79 61-71 50-66 43-83 50-85 43-85 43-85 Gender Male 2 3 1 2 2 2 18 4 22 (55.0%) 34 (57.6%) Female 2 0 2 1 1 1 16 2 18 (45.0%) 25 (42.4%) Race White 3 2 3 3 3 2 29 6 35 (87.5%) 51 (86.4%) Black, African 0 0 0 0 0 0 1 0 1 (2.5%) 1 (1.7%) American Asian 1 1 0 0 0 0 3 0 3 (7.5%) 5 (8.5%) Other 0 0 0 0 0 1 1 0 1 (2.5%) 2 (3.4%) Diagnosis PMF 3 2 1 3 2 2 27 4 31 (77.5%) 44 (74.6%) Post-PV MF 1 1 2 0 1 1 6 0 6 (15.0%) 12 (20.3% ) Post-ET MF 0 0 0 0 0 0 1 2 3 (7.5%) 3 (5.1%) Risk Category (Mayo PSS) High 0 0 1 2 0 3 14 6 20 (50.0%) 26 (44.1%) Not high* 4 3 2 1 3 0 20 0 20 (50.0%) 33 (55.9%) JAK2.sup.V617F 3 3 3 2 3 2 29 6 35 (87.5%) 51 (86.4%) Positive Transfusion 1 1 0 1 0 2 13 3 16 (40.0%) 21 (35.6%) Dependent Spleen Size > 3 3 3 2 3 2 28 5 33 (82.5%) 49 (83.1%) 10 cm Abbreviations: ET, essential thrombocythemia; JAK, Janus kinase; MF, myelofibrosis; PMF, primary myelofibrosis; PV, polycythemia vera; PSS, prognostic scoring system. *Equivalent to symptomatic/treatment refractory intermediate-risk disease. .dagger.Mean (standard deviation)
[0149] In the dose-escalation phase, the starting dose of TG101348 was 30 mg/day and subsequent dose levels were 60, 120, 240, 360, 520, 680 and 800 mg/day (Table 7). At 800 mg/day, 2 of 6 patients experienced DLT; consequently, the MTD was declared at 680 mg/day. In the dose-confirmation phase, all patients started treatment at the MID. The "MTD cohort" (n=40; Table 7) included patients who received 680 mg/day as their starting dose (dose-escalation cohort, n=3; dose-confirmation cohort, n=31) and those whose drug dose was decreased from 800 mg/day (n=6) to 680 mg/day after MTD was declared.
[0150] The median (range) exposure to TG101348 for the overall (n=59) and MTD (n=40) cohorts was 155 (2-172) and 147 (8-171) days, respectively. TG101348 doses at the end of each cycle per dose cohort are illustrated in FIGS. 10 and 11. In the MTD cohort, 28 subjects (70%) required dose-reduction during the first 6 cycles; the primary reasons were: cytopenia(s) (20%), gastrointestinal adverse events (12.5%), amylase/lipase elevation (10%), ALT elevation (7.5%), investigator discretion (7.5%), or other adverse events (12.5%). The median cycle at dose-reduction for the MTD cohort was cycle 3 (range 1-7); the median (range) dose at the end of cycle 3 was 680 mg/day (360-680 mg/day); and 520 mg/day (360-680 mg/day) at the end of cycle 6.
[0151] Forty three (73%) subjects, including 28 (70%) from the MTD cohort, continued treatment on the extension study; at entry into the extension study, 31 (72%) subjects were receiving <680 mg/day of the drug (median 520 mg/day; range 120-680 mg/day). At data cutoff, the median (range) cumulative exposure to TG101348 for the 43 subjects was 380 days (170-767). The number of treatment cycles completed ranged from 7-29; 39 subjects (66%), including 27 (68%) from the MTD cohort completed 12 treatment cycles. At data cutoff, 28%, and 14% of subjects who entered the extension study had completed 18 and 24 treatment cycles, respectively. The median (range) treatment dose during the extension phase was 440 mg/day (120-680 mg/day).
[0152] Pharmacokinetics:
[0153] Peak plasma concentration of TG101348 was achieved 1-4 hours after dosing. TG101348 showed greater than dose-proportional increases in plasma PK parameters (C.sub.max and AUC.sub.0-4) (Table 8 and FIG. 12). Mean steady-state C.sub.max and AUC.sub.0-t values increased approximately 54- and 88-fold, respectively, over a 27-fold increase in dose. The terminal phase half-life at steady state remained similar across all doses (16 to 34 hours), consistent with linear drug elimination. FIG. 18 shows a plot of mean plasma TG101348 concentrations versus time on a linear plot after once daily oral doses (Cycle 1; Day 28). The figure shows the IC50, IC90, and 3 times IC90 (3.times.IC90) values for TG101348 in relation to the plasma concentration of TG101348 over time. A dose of 520 mg/day exhibited a plasma concentration TG101348 that was above 3.times.IC90 over the course of at least 24 hours after the dose was administered. A dose of 360 mg/day exhibited a Cmax above 3.times.IC90 and a plasma concentration of TG101348 that was above IC90 over the course of at least 24 hours after the dose was administered.
TABLE-US-00009 TABLE 8 Mean (SD) plasma pharmacokinetic parameters following multiple daily doses of TG101348 (Cycle 1, Day 28) in MF-TG101348-001 Dose/Day 30 mg 60 mg 120 mg 240 mg 360 mg 520 mg 680 mg 800 mg Parameter (n = 3) (n = 3) (n = 3) (n = 3) (n = 3) (n = 3) (n = 27) (n = 5) C.sub.max 81.85 257.33 556.67 1796.67 1717.33 3886.67 3064.07 4380.00 (ng/mL) (95.630) (121.138) (135.500) (648.254) (1558.705) (3560.707) (1129.671) (1764.809) T.sub.max* (hr) 2.00 (0.5, 1.00 (1.0, 2.00 (0.5, 2.00 (2.0, 2.00 (2.0, 4.00 (4.0, 4.00 (0.0, 2.25 (2.0, 4.0) 4.0) 4.0) 2.1) 4.0) 4.0) 8.3) 4.0) AUC.sub.(0-t) 806.76 2426.53 7645.69 26193.40 23879.05 61749.22 55111.68 70840.97 (hr*ng/mL) (806.973) (1048.264) (2810.740) (11767.460) (16898.162) (57240.295) (25702.038) (32668.886) T.sub.1/2 (hr) 20.94 15.68 24.42 20.77 21.39 20.94 33.71 23.99 (7.039) (3.464) (8.434) (6.238) (7.090) (5.006) (33.674) (9.674) .lamda.z (1/hr) 0.0354 0.0456 0.0305 0.0352 0.0353 0.0343 0.0301 0.0331 (0.01016) (0.00918) (0.00932) (0.00903) (0.01309) (0.00723) (0.01421) (0.01321) *T.sub.max is presented as median (min, max) SD indicates standard deviation; C.sub.max, peak plasma concentration; T.sub.max, the time to the maximal concentration; AUC.sub.(0-t), area under the concentration-time curve from time zero to the last measurable concentration; T.sub.1/2, terminal half-life; and .lamda.z, the elimination rate constant.
[0154] Safety Profile:
[0155] The DLT in 2 of 6 patients treated at 800 mg/day was asymptomatic grade 3 or 4 hyperamylasemia (with or without hyperlipasemia) that was reversible. The most common non-hematologic adverse events at least possibly related to TG101348 included predominantly grade 1 nausea, diarrhea and vomiting; grade 3 events were reported overall/in the MTD cohort for 3%/5%, 10%/13%, and 3%/3% of subjects, respectively, and there were no Grade 4 events (Table 9). These adverse events were dose-dependent, with grade 3 occurrences observed almost exclusively with a TG101348 starting dose of >680 mg/day. The gastrointestinal symptoms were largely self-limited or controlled by symptomatic treatment and/or dose reduction. Other adverse events (Grades 3/4; overall/MTD cohort) included asymptomatic increases in serum lipase (10%/15%), AST (2%/3%). ALT (7%/8%), creatinine (0%/0%) and alkaline phosphatase (0%/0%) (Table 9).
TABLE-US-00010 TABLE 9 Treatment-Emergent Non-Hematologic Adverse Events Considered at Least Possibly Related to TG101348 and Reported for .gtoreq. 0% of Subjects MTD Cohort All Subjects (n = 40) (n = 59) Severity Severity Severity Severity Adverse Events Grade 1-2 Grade 3- Grade 1- Grade 3-4 Gastrointestinal disorders Nausea 31 2 (5.0%) 39 2 (3.4%) Diarrhea 25 5 32 6 (10.2%) Vomiting 27 1 (2.5%) 32 2 (3.4%) Abdominal pain 4 (10.0%) 0 6 (10.2%) 0 General disorders Anorexia 6 (15.0%) 0 8 (13.6%) 0 Edema peripheral 4 (10.0%) 0 6 (10.2%) 0 Abnormal laboratory values Hyperlipasemia 9 (22.5%) 6 10 6 (10.2%) Alanine 9 (22.5%) 3 (7.5%) 11 4 (6.8%) aminotransferase increased Aspartate 13 1 (2.5%) 15 1 (1.7%) aminotransferase increased Blood creatinine 11 0 14 0 increased Blood alkaline 9 (22.5%) 0 10 0 phosphatase increased Hypocalcemia 6 (15.0%) 1 (2.5%) 7 (11.9%) 1 (1.7%) Skin and subcutaneous tissue disorders Skin exfoliation 8 (20.0%) 0 8 (13.6%) 0 Dry skin 6 (15%) 0 6 (10.2%) 0
[0156] Grade 3/4 hematological adverse events considered related to TG101348 included anemia (35% of 37 subjects who were not transfusion dependent at baseline), thrombocytopenia (24%) and/or neutropenia (10%) (Table 10). The majority of treatment-emergent cytopenias were noted in the first three cycles of treatment. Of the 13 subjects who developed grade 3/4 anemia (all in the MTD cohort). 67% entered the study with grade 2 anemia. Emergence of transfusion requirement was significantly lower for subjects who initiated treatment at 240-520 mg/day (33%) as opposed to 680 mg/day (72%). Of the 14 subjects with grade 3/4 thrombocytopenia, 4 and 5 subjects entered the study with grade 1 and 2 thrombocytopenia, respectively.
TABLE-US-00011 TABLE 10 Treatment-Emergent Hematologic Adverse Events Considered at Least Possibly Related to TG101348 and Reported for .gtoreq.10% of Subjects MTD Cohort All Subjects (n = 40) (n = 59) Severity Severity Severity Severity Grade 1-2 Grade 3-4 Grade 1-2 Grade 3-4 Anemia* 2 (8.3%) 13 (54.2%) 3 (8.1%) 13 (35.1%) Throm- 8 (20.0%) 11 (27.5%) 10 (17.0%) 14 (23.7%) bocytopenia Neutropenia 2 (5.0%) 4 (10.0%) 2 (3.4%) 6 (10.2%) *Events reported only for subjects who were not transfusion dependent at study entry (MTD Cohort, n = 24; All Subjects, n = 37) are presented.
[0157] At data cutoff, no unique safety findings have emerged with continued dosing of TG101348 beyond 6 cycles of therapy.
[0158] Serious adverse events considered at least possibly related to TG101348 occurred in 8 subjects and included asymptomatic hyperlipasemia, thrombocytopenia/neutropenia, depression, tumor lysis syndrome, cerebrovascular accident, and dehydration (Table 11). One subject discontinued treatment due to Grade 4 thrombocytopenia; all other events were reversible and subjects were able to resume treatment at a lower dose after resolution of the adverse event.
TABLE-US-00012 TABLE 11 Serious Adverse Events Assessed by Investigators as at Least Possibly Related to Therapy (MF-TG101348-001 and MF-TG101348-002) Starting Dose/ Onset From CTCAE Dose at Event Start of Dosing Severity Action Taken Subject # Event (mg/day) (days) Grade With Study Drug Outcome 105-013 Thrombocytopenia 240/360 215 4 None Recovered/resolved Thrombocytopenia 240/360 247 4 Permanently discontinued Not recovered/ not resolved Hyperlipasemia 240/0 356 4 None Recovered/resolved 104-015 Depression 360/520 256 3* Permanently discontinued Not recovered/ not resolved 106-024 Nausea 800/680 87 2 Stopped temporarily Recovered/resolved Vomiting 800/680 87 2 Stopped temporarily Recovered/resolved Diarrhea 800/680 87 3 Stopped temporarily Recovered/resolved Dehydration 800/680 87 2 Stopped temporarily Recovered/resolved Tumor lysis syndrome 800/440 366 3 Stopped temporarily Recovered/resolved Dehydration 800/400 474 3 None Recovered/resolved 106-033 Pleuritic pain 680/680 8 2 Stopped temporarily Recovered/resolved 106-045 Dehydration 680/440 170 3 Stopped temporarily Recovered/resolved 101-047 Neutropenia 680/680 52 2 Stopped temporarily Recovered/resolved 105-056 Cerebrovascular 680/680 22 4 Stopped temporarily Recovered/resolved accident Gallbladder pain 680/520 95 3 Stopped temporarily Recovered/resolved with sequelae 105-059 Hyperlipasemia 680/680 8 3 Stopped temporarily Recovered/resolved Hyperlipasemia 680/520 28 3 Stopped temporarily Recovered/resolved Cardiac arrest 680/360 42 5 Permanently discontinued Fatal *Subject died (suicide) approximately 12 weeks after discontinuation of study drug.
One subject presented with severe pulmonary hypertension and right heart failure during cycle 4 (at 240 mg/day); the event was considered unrelated to TG101348 per the investigator.
[0159] Fifteen (25%) subjects discontinued treatment during the first 6 cycles of therapy (Table 12). Reasons for discontinuation included treatment-related adverse events (n=6); investigator decision/intercurrent illness (n=3) or withdrawal of consent (n=6). Eight of 43 subjects (19%) discontinued treatment during the extension study, including 3 because of adverse events following a total of 24 to 46 weeks on therapy (Table 12).
TABLE-US-00013 TABLE 12 Subjects discontinuing study due to death, toxicity, withdrawal of consent, or intercurrent illness MF-TG101348-001 Reasons for Discontinuation (Table 12 A) Starting Dose at Duration of Dose Termination Treatment Subject (mg/day) (mg/day) (days) Reason 102-002 30 30 2 Investigator discretion - previously undiagnosed cardiac condition with long QT.sub.c interval 106-009 120 240 109 Patient withdrew consent 101-011 240 240 100 Patient withdrew consent 102-019 520 520 42 Adverse event - neutropenia (grade 3; probably related) 102-023 800 680 70 Investigator discretion - recurrent Waldenstrom's macroglobulinemia 104-027 800 680 77 Adverse event - thrombocytopenia (grade 4; possibly related) 106-028 800 520 44 Adverse event - thrombocytopenia (grade 4; possibly related) 104-029 680 680 44 Adverse event - endocarditis (grade 3; not related), embolic stroke (grade 3; not related) 101-032 680 680 8 Investigator discretion - Acquired factor VIII inhibitor 101-040 680 520 24 Adverse events - diarrhea (grade 3; possibly related) 103-043 680 360 68 Patient withdrew consent 103-046 680 680 26 Patient withdrew consent 102-051 680 600 108 Patient withdrew consent 102-054 680 680 75 Patient withdrew consent 105-059 680 360 27 Adverse event - cardiac arrest (grade 5; possibly related) MF-TG101348-002 Reasons for Discontinuation (Table 12B) Cumulative Starting Dose at Duration of Dose Termination Treatment Subject (mg/day) (mg/day) (days) Reason 101-005 60 360 196 Investigator discretion - lack of response to treatment 106-010 120 520 185 Investigator discretion 105-013 240 360 321 Adverse event - thrombocytopenia (grade 4; probably related) 104-015 360 520 257 Adverse event - depression (grade 3; possibly related) 106-016 360 680 527 Investigator discretion - lack of response to treatment 104-017 520 200 309 Investigator discretion - disease progression 105-021 680 520 357 Patient withdrew consent 101-047 680 320 233 Adverse event - elevated creatinine (grade 2; possibly related)
[0160] Three subjects had disease progression (doses at study start and discontinuation are indicated): one each with progressive hepatosplenomegaly and ascites with superimposed endocarditis (cycle 2; 680 and 520 mg/day), accelerated myelofibrosis (cycle 13; 520 and 200 mg/day), and leukemic transformation (cycle 2; 520 and 520 mg/day).
[0161] Responses are shown below.
[0162] Splenomegaly:
[0163] The onset of spleen response was rapid, and generally seen within the first 2 cycles. By cycle 6, 36 subjects (61%) had experienced a minimum 25% decrease in palpable spleen size, including 65% in the MTD cohort (intent-to-treat analysis). By this time-point, a .gtoreq.50% decrease in palpable spleen size persistent for at least 8 weeks (i.e. Clinical Improvement ("CI") per IWG-MRT criteria) had been observed in 39% and 45% of subjects overall and in the MTD cohort, respectively. Spleen responses per treatment cycle for the MTD cohort are shown in FIG. 13. Three of 4 subjects (75%) with JAK2V617F-negative MF who completed 6 cycles of treatment achieved CI. The lowest starting dose at which CI was observed was 240 mg/day. The median time (range) to CI across doses was 141 days (41 to 171), and 113 days (41-170) for the MTD cohort. By cycle 12, spleen responses (CI) were observed in 48% and 50% of subjects, for the overall and MTD cohorts, respectively. The mean (standard deviation) duration of spleen response per IWG-MRT criteria was 315 (.+-.129) days and 288 (.+-.76) days for the overall and MTD cohorts, respectively.
[0164] Constitutional Symptoms:
[0165] Thirty five subjects in the MTD cohort endorsed the presence and severity of early satiety, fatigue, night sweats, cough, and pruritus on an 11-point scale (0=absence of symptoms to 10=worst imaginable symptoms) at baseline and at the end of at least one cycle. Symptoms were categorized as "absent" (score=0), "mild" (score=1-3), "moderate" (score=4-7), or "severe" (score=8-10).
[0166] Early satiety was reported by 29 (85%) subjects at baseline. After 2 cycles of treatment (n=27), 56% reported complete resolution of this symptom (FIG. 14A). Fatigue was reported at baseline by 26 (76%) subjects. After 6 cycles (n=16), 63% reported improvement and 25% complete resolution of this symptom (FIG. 14B). Night sweats were reported at baseline by 14 (40%) subjects. After 1 cycle, 64% of subjects had complete resolution of this symptom; after 6 cycles, this proportion had increased to 89% (n=9) (FIG. 14C). Cough was reported at baseline by 13 (37%) subjects. After 1 cycle (n=12), 75% reported improvement and 67% complete resolution of this symptom. Pruritus was reported by 8 (23%) subjects at baseline. After 1 cycle, 75% had improvement, with 50% reporting complete resolution. Responses in constitutional symptoms were durable in most instances.
[0167] Body Weight:
[0168] At the end of 6 and 12 cycles, the median body weight was stable relative to baseline for the overall and MTD cohorts (Table 13).
TABLE-US-00014 TABLE 13 Change in weight during study treatment Baseline 6 Cycles 12 Cycles MTD MTD MTD Overall Cohort Overall Cohort Overall Cohort Weight (kg) (n = 57) (n = 38) (n = 43) (n = 28) (n = 36) (n = 26) Median (range) 75.6 77.7 76.9 77.7 76.1 76.5 (48.2-105.2) (48.2-96.1) (51.4-105.8) (51.4-97.6) (49.8-106.8) (49.8-99.5) Change from n/a n/a 0.4 0.6 0.7 0.35 baseline Median (-11.7-8.9) (-9.2-8.9) (-10.7-13.7) (-10.7-13.7) (range) kg indicates kilograms; n, number, and MTD, maximum tolerated dose
[0169] Leukocytosis and Thrombocytosis:
[0170] Leukocytosis (WBC count >11.times.10.sup.9/L) was present at baseline in 33 subjects (56%), 28 of whom completed 6 cycles of treatment; of these, 18 were in the MTD cohort. Following 6 cycles, 16 subjects across doses (57%) and 13 subjects in the MTD cohort (72%) achieved a normal WBC count (FIG. 15); following 12 cycles, 14 of 25 (56%) across doses and 10 of 17 (59%) in the MTD cohort had normal WBC counts.
[0171] Thrombocytosis (platelet count >450.times.10.sup.9/L) was noted at baseline for 10 (17%) subjects across doses and 7 (19%) in the MTD cohort (n=37), all of whom completed 6 cycles of therapy. At this time point, 90% and 100% of subjects across doses and in the MTD cohort, respectively, achieved a normal platelet count; following 12 cycles, 7 of 8 subjects (88%) across doses and all 6 subjects in the MTD cohort had a normal platelet count.
[0172] JAK2V617F Allele Burden:
[0173] Fifty-one subjects (86%) were JAK2V617F-positive, with a median (range) allele burden of 20% (3%-100%); of these, 23 (45%) had a "significant" allele burden (defined as >20% at baseline) with a median (range) of 60% (23%-100%). For the overall mutation-positive subjects, there was a significant decrease in the JAK2V617F allele burden after 6 cycles (p=0.04) and 12 cycles of treatment (p=0.01) (FIGS. 16A and 16B). After 6 and 12 cycles of treatment, the median (range) allele burden was 17% (0%-100%) and 19% (0%-100%), respectively. Similarly, for the 23 subjects with baseline JAK2V617F allele burden of >20%, there was a significant and even more pronounced decrease in the JAK2V617F allele burden after 6 cycles (p=0.002) and 12 cycles of treatment (p=0.002) (FIGS. 16C and 16D). After 6 and 12 cycles of treatment, the median (range) allele burden was 31% (4%-100%) and 32% (7%-100%), respectively. After 6 cycles, 16 of 20 subjects (80%) with baseline allele burden >20% who reached this time-point exhibited a median 61% (range 6% to 96%) decrease, and 9 subjects (45%) had a >50% decrease in JAK2V617F allele burden. In contrast, 4 subjects (20%) exhibited an increase (18%, 21%, 30%, and 58%). Eighteen subjects (78%) of the group with allele burden >20% completed 12 cycles of treatment with a median 50% (range 29% to 82%) decrease, and 7 (39%) subjects had a >50% decrease in JAK2V617F. Three (17%) subjects exhibited an increase in allele burden (7%. 18%, and 22%), and 2 others with 100% allele burden at baseline exhibited no change.
[0174] Discussion:
[0175] A significant proportion of patients treated in this study experienced rapid, substantial, and durable control of symptomatic splenomegaly, leukocytosis, thrombocytosis, and constitutional symptoms. In addition, there was also evidence for a significant reduction in genomic disease burden that indicates potential for disease modifying activity. There were responses in MF patients who were JAK2V617F negative. It is unknown whether the subjects in this study have other mutations in the JAK-STAT signal transduction pathway such as MPL, LNK or as yet unknown alleles (Pardanani A D et al., Blood 108:3472-3476, 2006; Oh S T et al., Blood First Edition Paper, prcpublishcd online Apr. 19, 2010; DOI 101182/blood-2010-02-270108 2010; Pardanani A et al., Leukemia In press:2010).
[0176] The clinical study results show that TG101348 therapy can be discontinued without prior dose reduction or tapering. Subjects that were discontinued (whether or not recontinued at a later date) did not experience "cytokine rebound". This indicates that the treatment may be discontinued without prior dose reduction.
[0177] Cytokine rebound in the context of myelofibrosis is a phenomenon that has occurred in patients receiving therapy other than TG101348 therapy and were discontinued for any reason. In some cases, the discontinued patients experienced severe symptoms including acute spleen size enlargement and relapse of constitutional symptoms. In some cases, the discontinued patients experienced life-threatening hemodynamic disturbances (Wadleigh and Tefferi, Clinical Advances in Hematology & Oncology, 8:557-563, 2010).
[0178] Of note, among small molecule inhibitors of the JAK-STAT pathway in MF, TG101348 appeared to be unique in its ability to induce a significant and sustained decrease in JAK2V617F mutant allele burden. Without wishing to be bound by any theory, it appeared that the effect of JAK2 inhibition on disease burden was the basis for evidence of clinical efficacy in myelofibrosis with TG101348, as opposed to an indirect anti-cytokine effect that may play a major role in responses to JAK family antagonists that have off-target activity for JAK1 as well as for JAK2. In support of this, there were no consistent changes in levels of pro-inflammatory cytokines (interleukin ("IL")-6, IL-2, IL-8, and TNF-.alpha.) relative to baseline during the course of TG101348 treatment (FIG. 17). In contrast, and consistent with the on-target activity of TG101348 for JAK2, increases in serum EPO and to a lesser extent TPO levels relative to baseline were observed after treatment initiation (data not shown).
[0179] The DLT (asymptomatic hyperamylasemia, sometimes with hyperlipasemia) for TG101348 was observed with other small molecule inhibitors including nilotinib (Kantarjian H M et al., Blood 110:3540-3546, 2007). Gastrointestinal adverse events were frequent in this study but accounted for treatment discontinuation in only one subject. These symptoms occurred as early as after the first administered dose, and demonstrated a clear dose-dependent relationship. The myelosuppressive effects of TG101348 were also dose-dependent.
[0180] While the MTD (680 mg/day) of TG101348 was the most efficacious dose, it was also associated with the highest incidence of adverse events. Therefore, a lower starting dose (e.g. 400-500 mg/day) may provide an optimal risk/benefit balance. Furthermore, because myelofibrosis is a heterogeneous disease, a dynamic dosing schedule may maximize the opportunity for identifying a patient-specific optimal dose.
[0181] These observations suggest that, in addition to MF, TG101348 may also have a potential role for the treatment of PV and ET.
Example 4. Synthesis of TG101348
Example 4.1 N-tert-Butyl-3-(2-chloro-5-methyl-pyrimidin-4-ylamino)-benzenesulfonamide (Intermediate)
Example 4.1(a)
##STR00003##
[0183] A mixture of 2-chloro-5-methyl-pyrimidin-4-ylamine (1) (0.4 g, 2.8 mmol), 3-bromo-N-tert-butyl-benzenesulfonamide (2) (1.0 g, 3.4 mmol), Pd.sub.2(dba).sub.3 (0.17 g, 0.19 mmol), Xantphos (0.2 g, 3.5 mmol) and cesium carbonate (2.0 g. 6.1 mmol) was suspended in dioxane (25 mL) and heated at reflux under the argon atmosphere for 3 h. The reaction mixture was cooled to room temperature and diluted with DCM (30 mL). The mixture was filtered and the filtrate concentrated in vacuo. The residue was dissolved in EtOAc and hexanes added until solid precipitated. After filtration, the title compound (1.2 g, 98%) was obtained as a light brown solid. It was used in the next step without purification. MS (ES+): m/z 355 (M+H).sup.+.
Example 4.1(b)
##STR00004##
[0185] The Intermediate was synthesized from 2,4-dichloro-5-methylpyrimidine (SM1) and N-t-butyl-3-aminobenzenesulfonamide (SM2) in the following steps: (1) Mix MeOH (6.7 UOa) and SM1 (Combi Blocks) (UOa); (2) Add SM2 (1.15 UOa, 082eq) and H.sub.2O (8.5 UOa); (3) Heat 45.degree. C., 20h, N.sub.2, IPC CPL SM2<2%; (4) Cool 20.degree. C.: (5) Centrifuge, N.sub.2; (6) Wash H.sub.2O (2.1 UOa)+MeOH (1.7 UOa); (7) Mix solid in H.sub.2O (4.3 UOa)+MeOH (3.4 UOa); (8) Centrifuge, N.sub.2; (9) Wash H.sub.2O (2.1 UOa)+MeOH (1.7 UOa); and (10) Dry 45.degree. C. vacuum, 15h. Obtained Intermediate, mass 49.6 kg (UOb); Yield 79%; OP: 99.6%.
Example 4.2 N-tert-Butyl-3-[(5-methyl-2-{[4-(2-pyrrolidin-1-ylethoxy)phenyl]amino}pyr- imidin-4-yl)amino]benzenesulfonamide
##STR00005##
[0186] Example 4.2(a)
[0187] A mixture of N-tert-Butyl-3-(2-chloro-5-methyl-pyrimidin-4-ylamino)-benzenesulfonamide (Intermediate) (0.10 g, 0.28 mmol) and 4-(2-pyrrolidin-1-yl-ethoxy)-phenylamine (3) (0.10 g, 0.49 mmol) in acetic acid (3 mL) was sealed in a microwave reaction tube and irradiated with microwave at 150.degree. C. for 20 min. After cooling to room temperature, the cap was removed and the mixture concentrated. The residue was purified by HPLC and the corrected fractions combined and poured into saturated NaHCO.sub.3solution (30 mL). The combined aqueous layers were extracted with EtOAc (2.times.30 mL) and the combined organic layers washed with brine, dried over anhydrous Na.sub.2SO.sub.4
References
















D00001

D00002
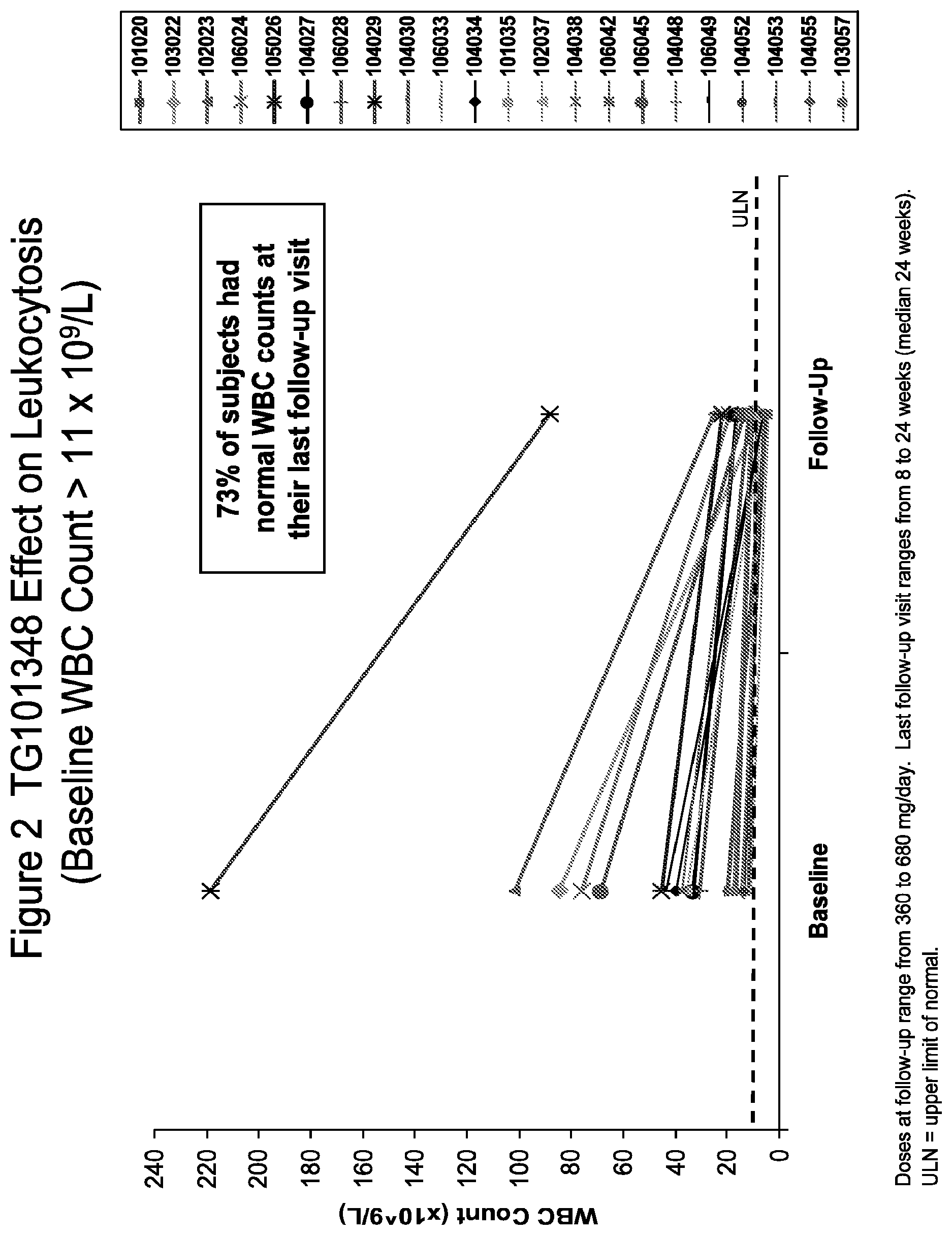
D00003

D00004
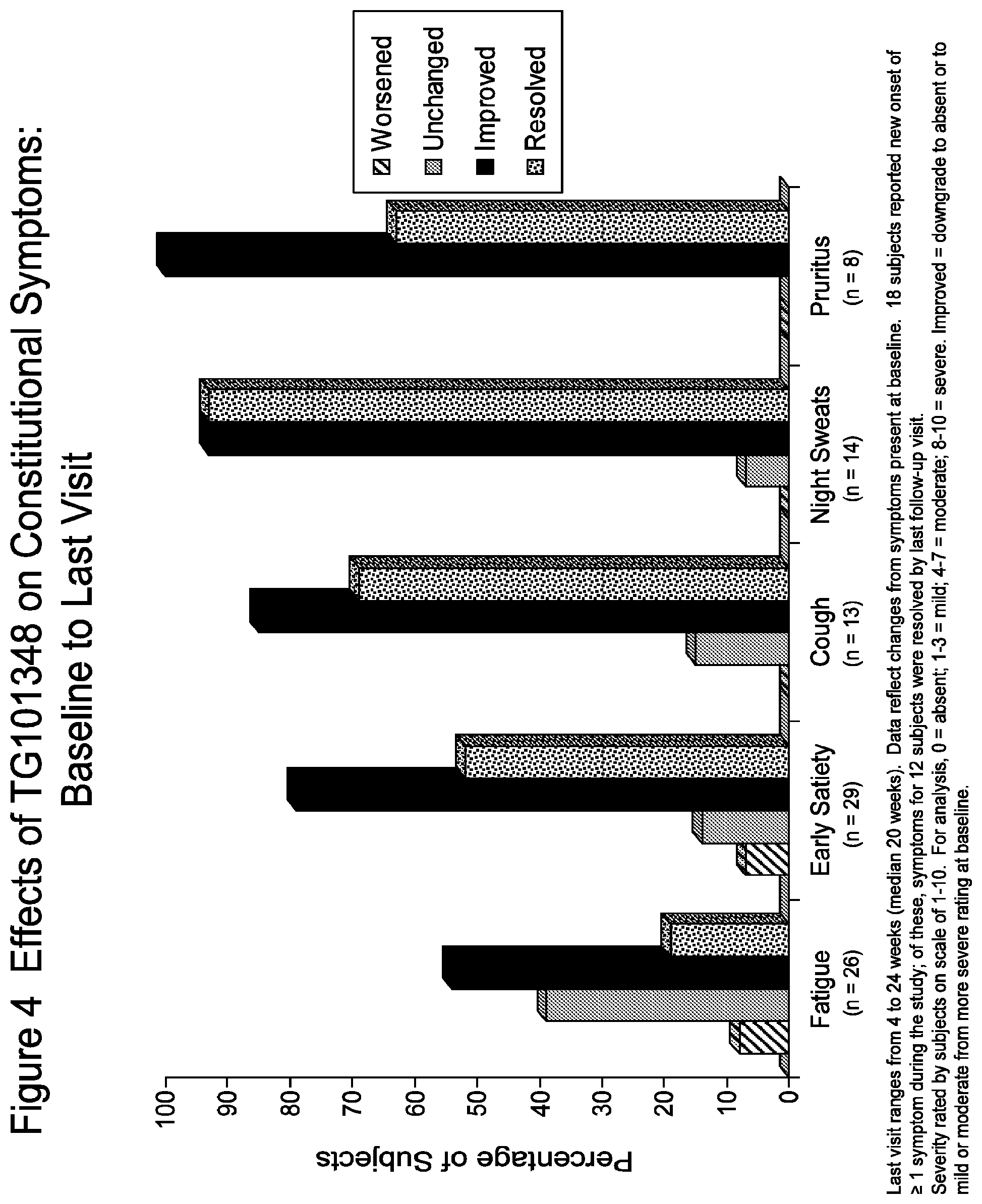
D00005

D00006

D00007

D00008

D00009

D00010
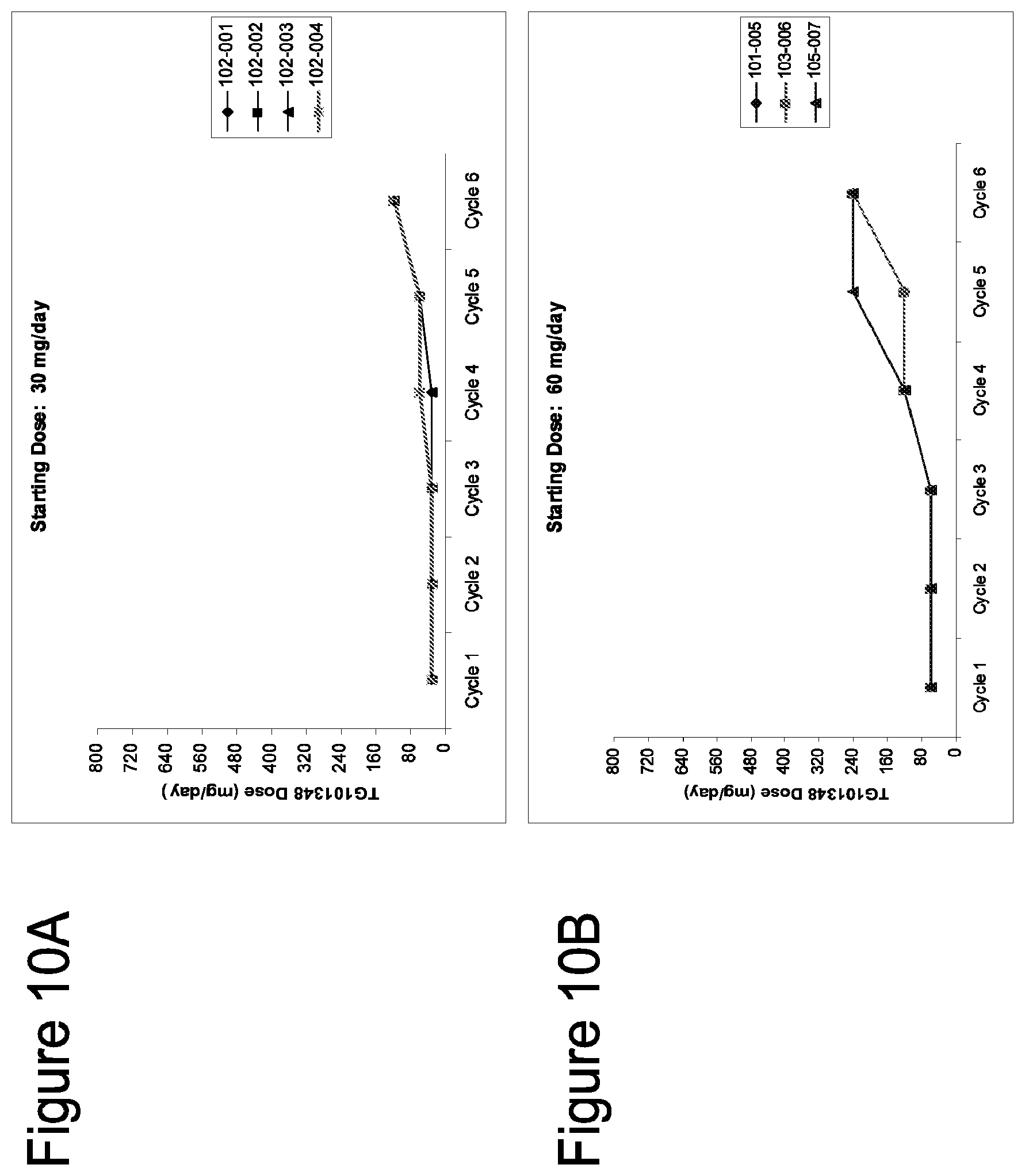
D00011

D00012

D00013

D00014
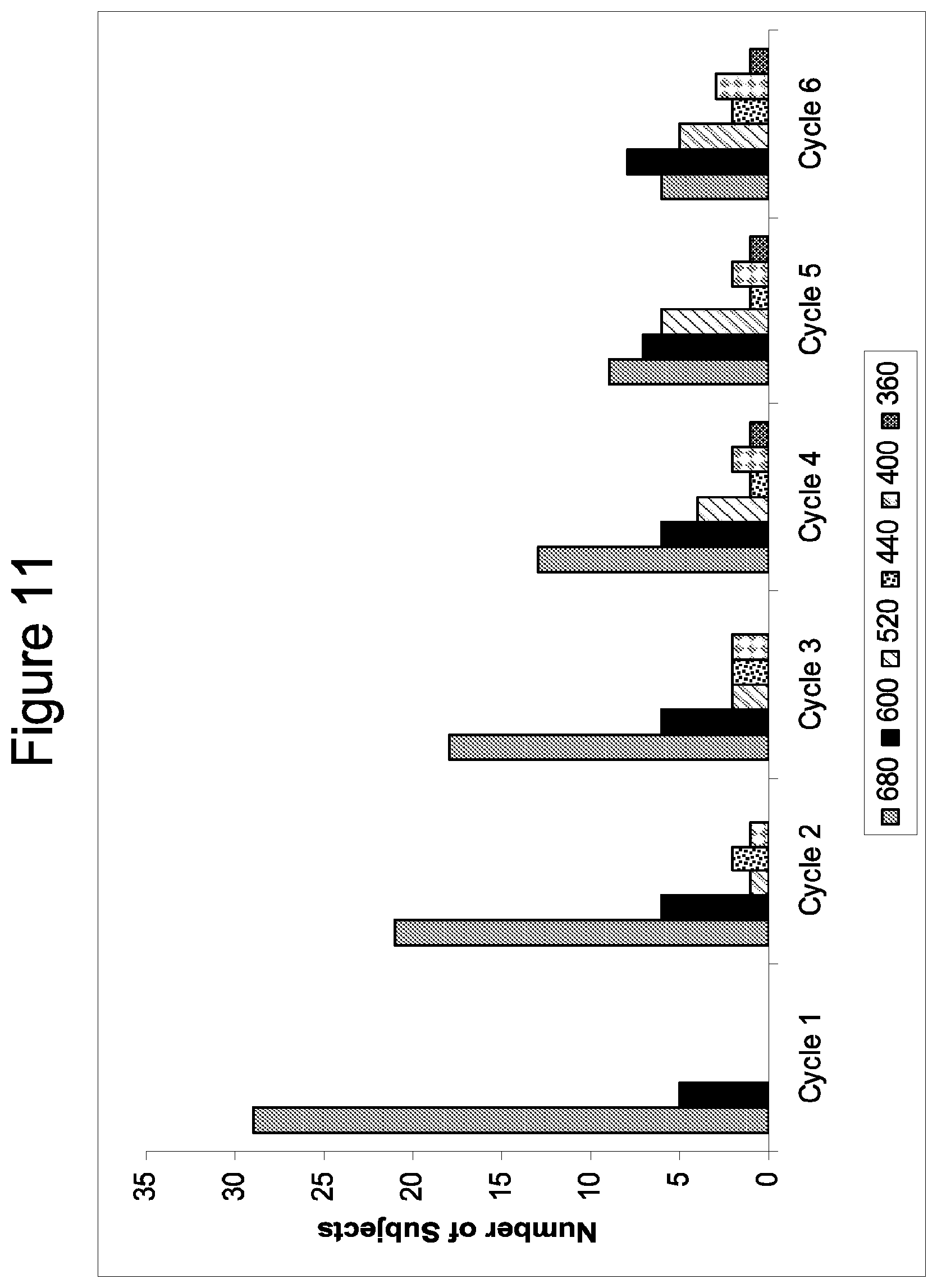
D00015
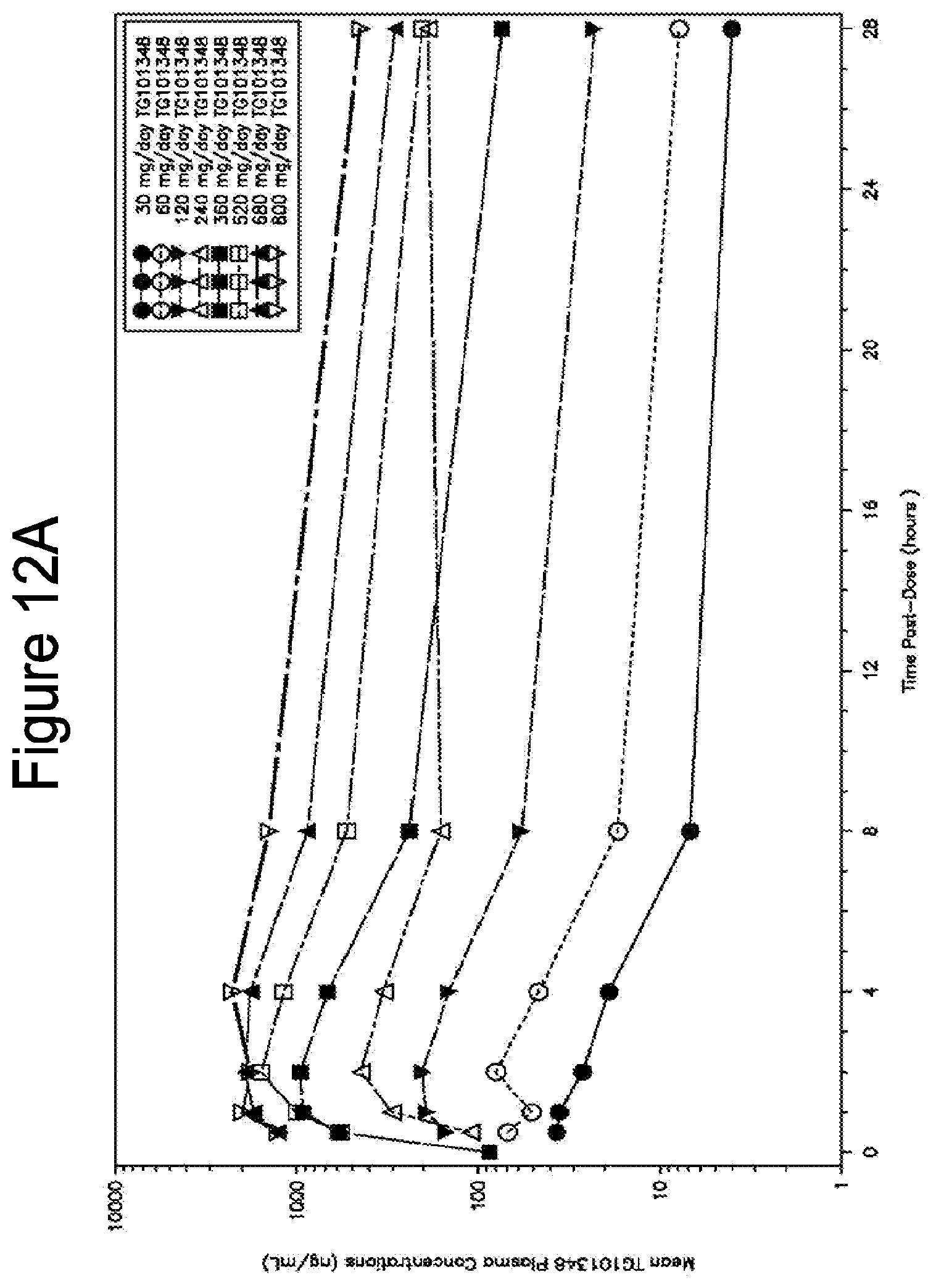
D00016

D00017
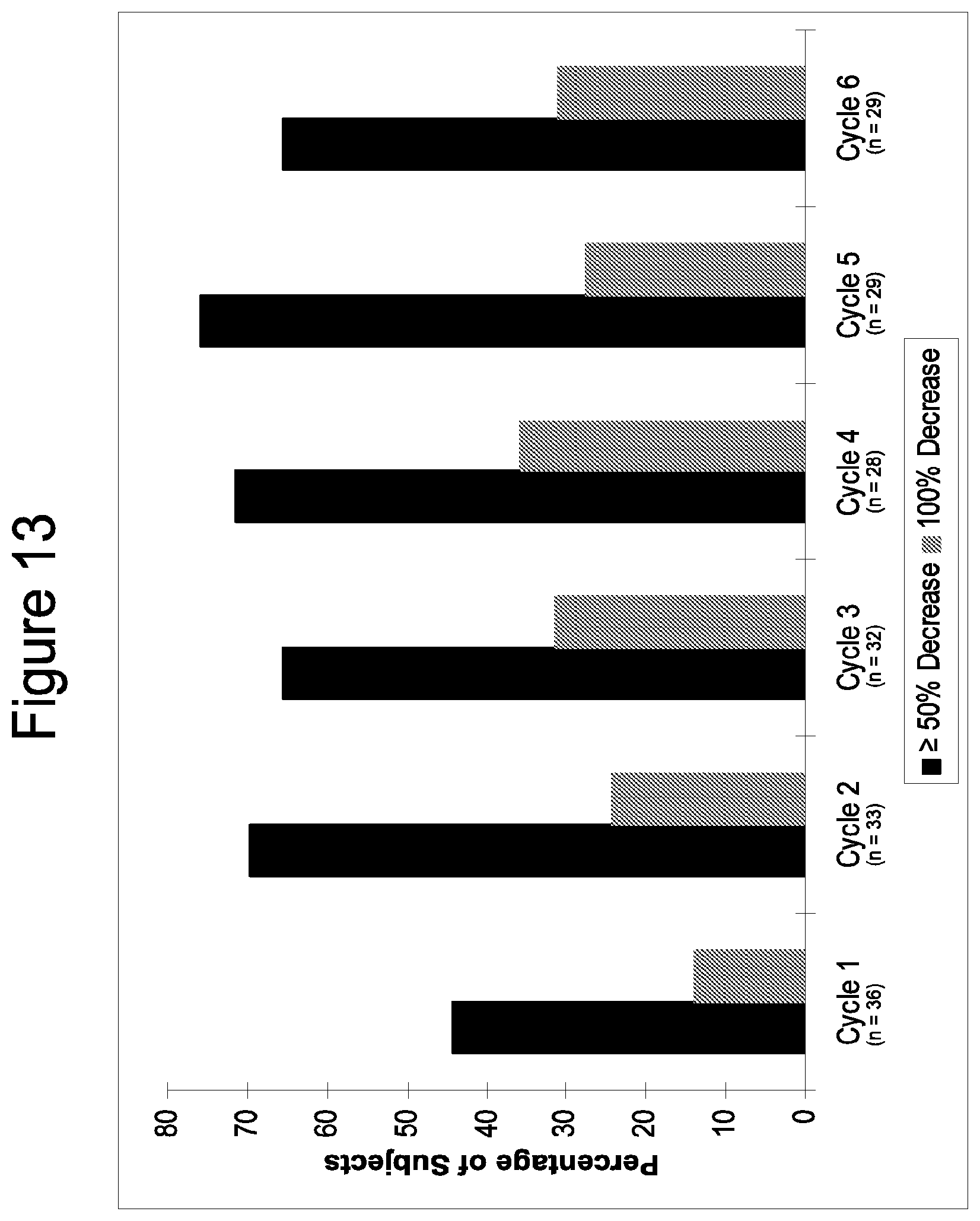
D00018

D00019

D00020
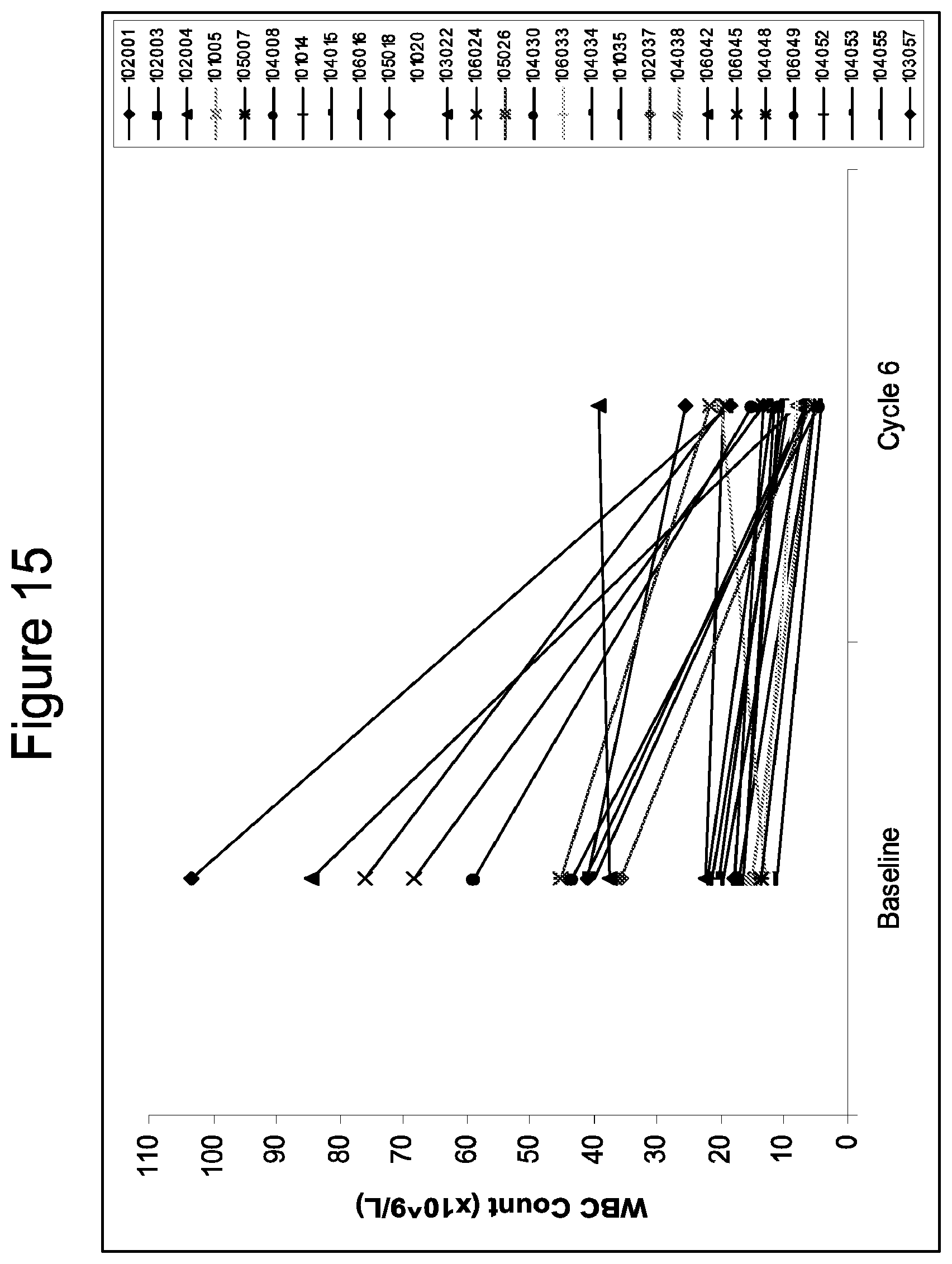
D00021

D00022
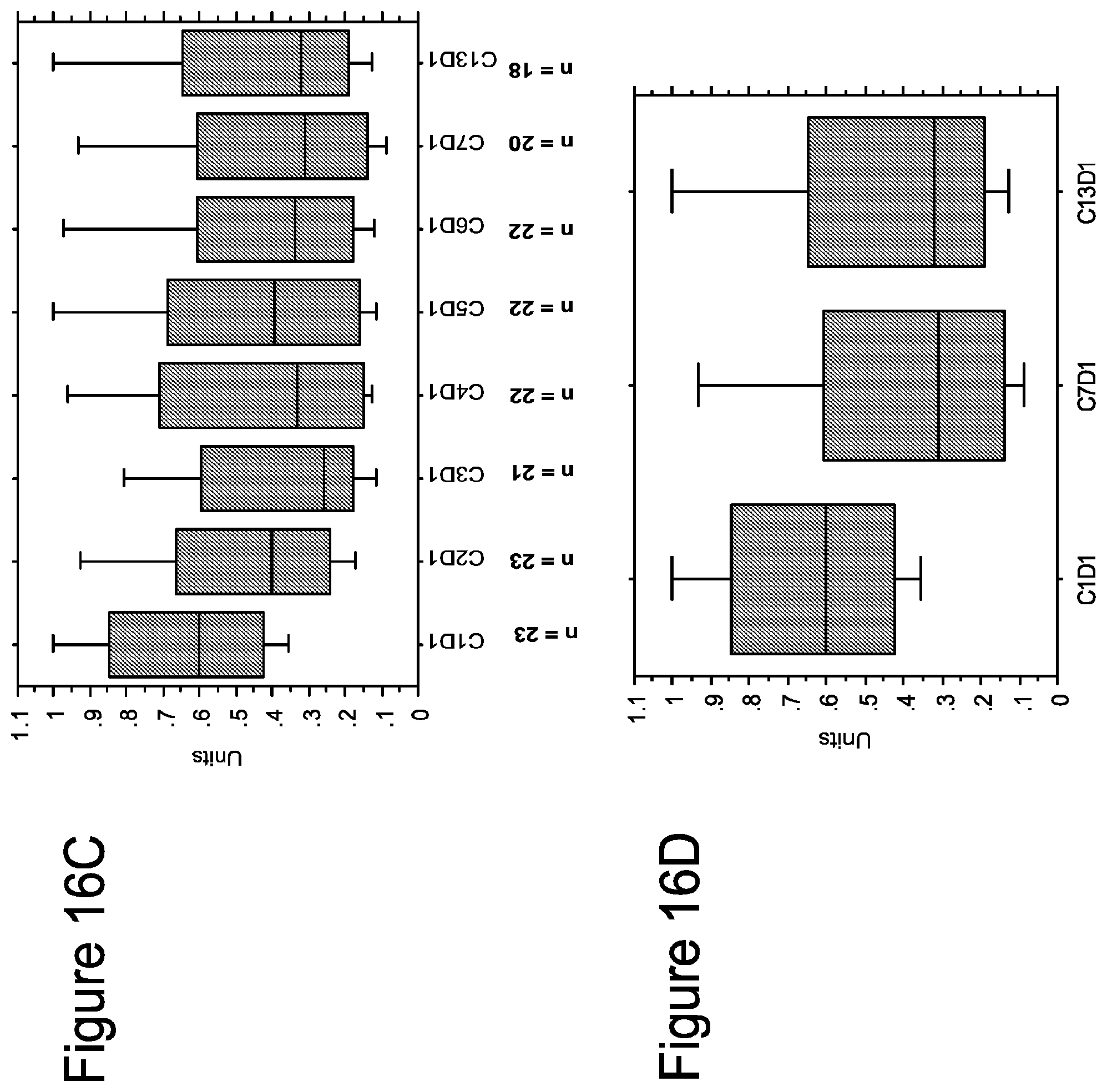
D00023

D00024
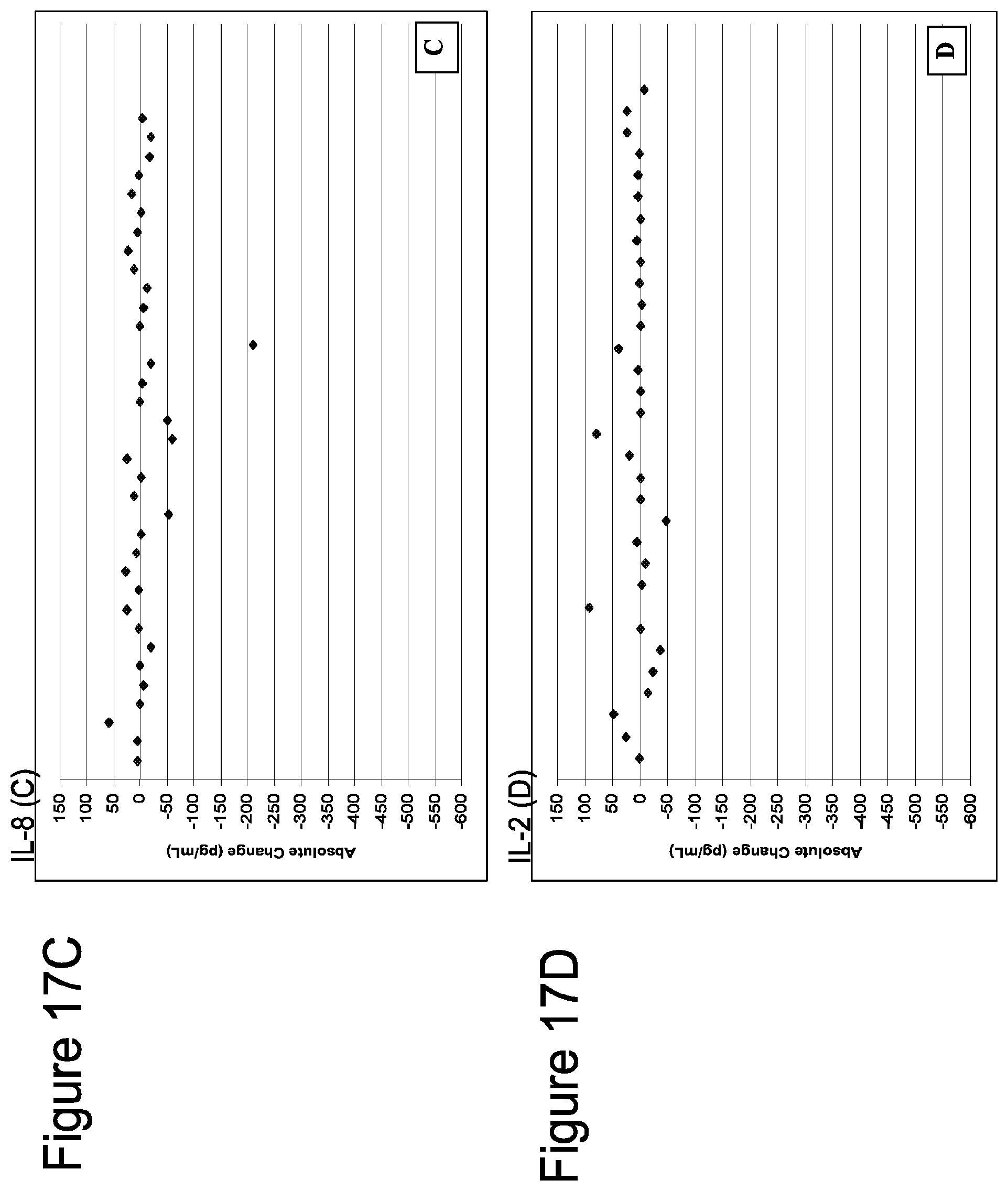
D00025

XML
uspto.report is an independent third-party trademark research tool that is not affiliated, endorsed, or sponsored by the United States Patent and Trademark Office (USPTO) or any other governmental organization. The information provided by uspto.report is based on publicly available data at the time of writing and is intended for informational purposes only.
While we strive to provide accurate and up-to-date information, we do not guarantee the accuracy, completeness, reliability, or suitability of the information displayed on this site. The use of this site is at your own risk. Any reliance you place on such information is therefore strictly at your own risk.
All official trademark data, including owner information, should be verified by visiting the official USPTO website at www.uspto.gov. This site is not intended to replace professional legal advice and should not be used as a substitute for consulting with a legal professional who is knowledgeable about trademark law.