Population Pharmacokinetics Tools And Uses Thereof
Jiang; Haiyan
U.S. patent application number 16/404385 was filed with the patent office on 2019-11-28 for population pharmacokinetics tools and uses thereof. The applicant listed for this patent is Bioverativ Therapeutics Inc.. Invention is credited to Haiyan Jiang.
| Application Number | 20190362856 16/404385 |
| Document ID | / |
| Family ID | 53274200 |
| Filed Date | 2019-11-28 |












View All Diagrams
| United States Patent Application | 20190362856 |
| Kind Code | A1 |
| Jiang; Haiyan | November 28, 2019 |
POPULATION PHARMACOKINETICS TOOLS AND USES THEREOF
Abstract
The present invention is directed to computer based pharmacokinetics systems, such as, web-based pharmacokinetics systems, and their use to predict a dose and a dosing interval for a patient in need of a clotting factor therapy.
| Inventors: | Jiang; Haiyan; (Belmont, MA) | ||||||||||
| Applicant: |
|
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Family ID: | 53274200 | ||||||||||
| Appl. No.: | 16/404385 | ||||||||||
| Filed: | May 6, 2019 |
Related U.S. Patent Documents
| Application Number | Filing Date | Patent Number | ||
|---|---|---|---|---|
| 15101756 | Jun 3, 2016 | 10325687 | ||
| PCT/US2014/068956 | Dec 6, 2014 | |||
| 16404385 | ||||
| 61944467 | Feb 25, 2014 | |||
| 61934286 | Jan 31, 2014 | |||
| 61913149 | Dec 6, 2013 | |||
| Current U.S. Class: | 1/1 |
| Current CPC Class: | G16C 20/90 20190201; A61K 38/4846 20130101; C12N 9/644 20130101; G06F 19/3456 20130101; G16H 20/10 20180101; G16H 50/50 20180101; C07K 2319/30 20130101; C12Y 304/21022 20130101; C07K 14/755 20130101; G16C 20/70 20190201; G06N 7/005 20130101; G16C 20/30 20190201; A61K 38/37 20130101 |
| International Class: | G16H 50/50 20060101 G16H050/50; G16H 20/10 20060101 G16H020/10; G06N 7/00 20060101 G06N007/00; G16C 20/70 20060101 G16C020/70; C12N 9/64 20060101 C12N009/64; C07K 14/755 20060101 C07K014/755; G16C 20/30 20060101 G16C020/30; A61K 38/48 20060101 A61K038/48; A61K 38/37 20060101 A61K038/37 |
Claims
1-44. (canceled)
45. A web-based method of estimating individual patient pharmacokinetics (PK) of a long-acting Factor VIII (FVIII), the method comprising: (a) receiving, by one or more electronic devices, individual long-acting FVIII PK information, (b) transmitting, by a processing device, the individual long-acting FVIII PK information to a web-based application program accessible through a web server, wherein the application is programmed to implement a long-acting FVIII population pharmacokinetic (popPK) model, such as that of Example 9 or 11, and a Bayesian estimation program, (c) receiving from the web-based server and program, individualized patient long-acting FVIII PK information using the popPK model, the Bayesian estimation program, and the transmitted information of (b), and (d) outputting, by the one or more electronic devices, the individualized patient PK information.
46. (canceled)
47. A web-based method of estimating individual patient pharmacokinetics (PK) of a long-acting Factor VIII (FVIII), the method comprising: (a) receiving, of individual long-acting FVIII PK information by a web-based application program accessible through a web server and programmed to implement a long-acting FVIII population pharmacokinetic (popPK) model, such as that of Example 9 or 11, and a Bayesian estimation program, wherein the received information is transmitted by one or more electronic devices, (b) calculating by the web-based program, individualized patient PK information of a long-acting FVIII using the FVIII popPK model, the Bayesian estimation program and the received information, and (c) transmitting, by a processing device, the estimated individualized patient long-acting FVIII PK information of (b) to one or more electronic devices, for output of the information.
48-52. (canceled)
53. A web-based method of estimating individual patient pharmacokinetics (PK) of a long-acting Factor VIII (FVIII), the method comprising: (a) receiving, by one or more electronic devices, information regarding individual body weight and (i) desired rise of plasma factor activity level following dosing or (ii) desired dose or desired dose interval, (b) transmitting, by a processing device, the information of (a) to a web-based application program accessible through a web server, wherein the application is programmed to implement a long-acting FVIII population pharmacokinetic (popPK) model, such as that of Example 9 or 11, and a Bayesian estimation program, (c) receiving from the web based server and program, individualized patient PK information of a long-acting FVIII calculated using the popPK model, the Bayesian estimation program, and the transmitted information of (b), and (d) outputting, by the one or more electronic devices, the estimated patient PK information.
54-56. (canceled)
57. The method of claim 53, further comprising selecting a dosing regimen based on the output estimated patient PK information of (d), and administering the long-acting FVIII to the patient according to the selected regimen.
58-70. (canceled)
71. The method of claim 53, wherein the long-acting FVIII polypeptide comprises a FVIII portion and a second portion.
72. (canceled)
73. (canceled)
74. The method of claim 71, wherein the second portion comprises a human Fc.
75. The method of claim 71, wherein the second portion comprises a mutant Fc.
76. The method of claim 71, wherein the long-acting FVIII polypeptide is in the form of a hybrid comprising a second polypeptide which comprises a neonatal Fc receptor (FcRn) binding partner (BP).
77. (canceled)
78. (canceled)
79. The method of claim 71, wherein said Factor VIII portion is human Factor VIII.
80. The method of claim 71, wherein said Factor VIII portion has a full or partial deletion of the B domain.
81-93. (canceled)
94. A web-based method of estimating individual patient pharmacokinetics (PK) of a long-acting Factor VIII (FVIII), the method comprising: (a) receiving, by one or more electronic devices, individual long-acting FVIII PK information, (b) transmitting, by a processing device, the individual long-acting FVIII PK information to a web-based application program accessible through a web server, wherein the application is programmed to implement a long-acting FVIII population pharmacokinetic (popPK) model, such as that of Example 16, and a Bayesian estimation program, (c) receiving from the web-based server and program, individualized patient long-acting FVIII PK information using the popPK model, the Bayesian estimation program, and the transmitted information of (b), and (d) outputting, by the one or more electronic devices, the individualized patient PK information.
95. A web-based method of estimating individual patient pharmacokinetics (PK) of a long-acting Factor VIII (FVIII), the method comprising: (a) receiving, of individual long-acting FVIII PK information by a web-based application program accessible through a web server and programmed to implement a long-acting FVIII population pharmacokinetic (popPK) model, such as that of Example 16, and a Bayesian estimation program, wherein the received information is transmitted by one or more electronic devices, (b) calculating by the web-based program, individualized patient PK information of a long-acting FVIII using the FVIII popPK model, the Bayesian estimation program and the received information, and (c) transmitting, by a processing device, the estimated individualized patient long-acting FVIII PK information of (b) to one or more one electronic devices, for output of the information.
96. (canceled)
97. (canceled)
98. A web-based method of estimating individual patient pharmacokinetics (PK) of a long-acting Factor VIII (FVIII), the method comprising: (a) receiving, by one or more electronic devices, information regarding individual body weight and (i) desired rise of plasma factor activity level following dosing or (ii) desired dose or desired dose interval, (b) transmitting, by a processing device, the information of (a) to a web-based application program accessible through a web server, wherein the application is programmed to implement a long-acting FVIII population pharmacokinetic (popPK) model, such as that of Example 16, and a Bayesian estimation program, (c) receiving from the web based server and program, individualized patient PK information of a long-acting FVIII calculated using the popPK model, the Bayesian estimation program, and the transmitted information of (b), and (d) outputting, by the one or more electronic devices, the estimated patient PK information.
99. (canceled)
100. The method of claim 98, further comprising selecting a dosing regimen based on the output estimated patient PK information of (d), and administering the long-acting FVIII to the patient according to the selected regimen.
101-109. (canceled)
110. The method of claim 98, wherein the long-acting FVIII polypeptide comprises a FVIII portion and a second portion.
111. (canceled)
112. (canceled)
113. The method of claim 110, wherein the second portion comprises a human Fc.
114. The method of claim 110, wherein the second portion comprises a mutant Fc.
115. The method of claim 110, wherein the long-acting FVIII polypeptide is in the form of a hybrid comprising a second polypeptide which comprises a neonatal Fc receptor (FcRn) binding partner (BP).
116. The method of claim 110, wherein said Factor VIII portion is human Factor VIII.
117. The method of claim 110, wherein said Factor VIII portion has a full or partial deletion of the B domain.
118-139. (canceled)
Description
RELATED APPLICATIONS
[0001] This application is a continuation of U.S. patent application Ser. No. 15/101,756, filed Jun. 3, 2016, which is a 35 U.S.C. .sctn. 371 filing of International Patent Application No. PCT/US2014/068956, filed Dec. 6, 2014, which claims priority to U.S. Provisional Patent Application Ser. Nos. 61/944,467, filed Feb. 25, 2014, 61/934,286, filed Jan. 31, 2014, and 61/913,149, filed Dec. 6, 2013, the entire disclosures of which are hereby incorporated herein by reference in their entirety.
FIELD OF THE INVENTION
[0002] The present invention is directed to computer based pharmacokinetics systems, such as, web-based pharmacokinetics systems, and their use to predict a dose and a dosing interval for a patient in need of a clotting factor therapy.
BACKGROUND ART
[0003] While plasma-derived and recombinant clotting factor products allow hemophilia patients to live longer and healthier, hemophilia still remains one of the most costly and complex conditions to manage. The cost of clotting factor products exceeds $50,000 a year per patient. See Blankenship C. S., Biotechnol. Healthc. 2008, 5(4): 37-40. According to the National Heart, Lung, and Blood Institute, National Institute of Health (NIH), approximately 18,000 people in the U.S. have hemophilia, and 400 babies are born with the disease each year. Morbidity & Mortality: 2012 Chart Book on Cardiovascular, Lung and Blood Disease, page 5, National Heart, Lung, and Blood Institute, NIH. Due to its complexity, this chronic disease requires a special therapeutic management process for doctors, pharmacies, and patients. Clinicians often assess lifestyle, psychosocial requirements, and the home environment when evaluating a patient's or guardian's ability to provide adequate care.
[0004] In hemophilia, blood clotting is disturbed by a lack of certain plasma blood clotting factors. Hemophilia A, the most common form of hemophilia, is caused by Factor VIII deficiency. Hemophilia B is caused by decreased synthesis of Factor IX protein or synthesis of defective Factor IX having reduced activity. Treating hemophilia involves replacing missing or defective clotting factor with recombinant or plasma-derived FVIII or FIX. For patients who have developed antibodies against recombinant or plasma-derived FVIII or FIX, Factor VII can be used as a bypass therapy. Commercially available clotting factors are usually administered by peripheral intravenous injection. However, for patients with small veins or children who require frequent injections, clotting factors can be administered by a central venous access device. See Blankenship C. S., Biotechnol. Healthc. 2008, 5(4): 37-40.
[0005] Currently, three FIX products are approved by the Food and Drug Administration (FDA). The first, BENEFIX.RTM., is a recombinant FIX product marketed by Pfizer. The second and third products are plasma-derived FIX products, ALPHANINE.RTM. marketed by Grifols and MONONINE.RTM. marketed by CSL Behring. According to their labels, BENEFIX.RTM. is supplied as a lyophilized powder in five different dosages: 250 IU, 500 IU, 1000 IU, 2000 IU, and 3000 IU. MONONINE.RTM. is supplied as a single dose vial with Sterile Water for Injection at 500 IU and 1000 IU. ALPHANINE is supplied in lyophilized form as single doses at 500 IU, 1000 IU, and 1500 IU. The FIX dose required for each patient is calculated based on the formula:
Number of factor IX IU required (IU)=Body Weight (kg).times.Desired Factor IX Increase (% or IU/dL).times.Reciprocal of Observed Recovery (IU/kg per IU/dL) (A)
[0006] Several Factor VIII products are also commercially available, which include recombinant FVIII products (ADVATE.RTM. and RECOMBINATE.RTM. marketed by Baxter, KOGENATE.RTM. FS marketed by Bayer, HELIXATE.RTM. FS marketed by CSL-Behring, and XYNTHA.RTM. and REFACTO.RTM. marketed by PFIZER) and Plasma-derived FVIII products (HEMOFIL-M.RTM. marketed by Baxter, MONARC-M.RTM. by American Red Cross, and MONOCLATE-P.RTM. marketed by CSL Behring). The required FVIII dose for each patient is calculated using the following formula:
Number of factor FVIII IU required (IU)=Body Weight (kg).times.Desired Factor FVIII Increase (IU/dL or % of normal).times.0.5(IU/kg per IU/dL) (B)
[0007] However, administering clotting factors can be complicated and costly for patients. The invention as described herein provides improved clotting factor-dosing methods.
BRIEF SUMMARY OF THE INVENTION
[0008] The present invention is directed to a method of estimating long-acting FIX dosing information individualized for a patient, the method comprising: a) receiving, by a computer-based system containing (i) the long-acting FIX population pharmacokinetic (popPK) model of Example 5 or 7 and (ii) a Bayesian estimation program, at least one of patient information and desired treatment outcome information, b) calculating, by the computer-based system, individualized long-acting FIX dosing information using the FIX popPK model, respectively, the Bayesian estimation program, and the received information, and c) outputting, by the computer-based system, the individualized dosing information.
[0009] Also disclosed is a method of estimating long-acting FVIII dosing information individualized for a patient, the method comprising: a) receiving, by a computer-based system containing (i) the long-acting FVIII popPK model of Example 9 or 11 or 16 and (ii) a Bayesian estimation program, at least one of patient information and desired treatment outcome information, b) calculating, by the computer-based system, individualized long-acting FVIII dosing information using the FVIII popPK model, respectively, the Bayesian estimation program, and the received information, and c) outputting, by the computer-based system, the individualized dosing information. Further disclosed is the method as described herein, further comprising selecting a dosing regimen based on the output individualized dosing information of (c) and administering the long-acting FIX polypeptide to the patient according to the selected dosing regimen. Also disclosed is the method as described herein, further comprising selecting a dosing regimen based on the output individualized dosing information of (c) and administering the long-acting FVIII polypeptide to the patient according to the selected dosing regimen.
[0010] Certain embodiments include a computer readable storage medium having instructions stored thereon that, when executed by a processor, causes the processor to perform the method as described herein.
[0011] Also disclosed is a system comprising a processor and a memory, the memory having instructions stored thereon that, when executed by the processor, cause the processor to perform the method as described herein.
[0012] Further disclosed is a method of estimating a long-acting FIX dosing regimen based on median popPK, the method comprising: a) receiving, by a computer-based system containing (i) the long-acting FIX popPK model of Example 5 or 7 and (ii) a Bayesian estimation program, at least one of patient information and desired treatment outcome information, b) calculating, by the computer-based system, median long-acting FIX PK information using the FIX popPK model, respectively, the Bayesian estimation program, and the received information, and c) outputting, by the computer-based system, the median PK information. Also disclosed is the method as described herein, further comprising selecting a dosing regimen based on the output median PK information of (c), and administering the long-acting FIX to a patient according to the selected dosing regimen.
[0013] Certain embodiments include a method of estimating a long-acting FVIII dosing regimen based on median popPK, the method comprising: a) receiving, by a computer-based system containing (i) the long-acting FVIII popPK model of Example 9 or 11 or 16 and (ii) a Bayesian estimation program, at least one of patient information and desired treatment outcome information, b) calculating, by the computer-based system, median long-acting FVIII PK information using the FVIII popPK model, respectively, the Bayesian estimation program, and the received information, and c) outputting, by the computer-based system, the median PK information. Also disclosed is the method as described herein, further comprising selecting a dosing regimen based on the output median PK information of (c), and administering the long acting FVIII to a patient according to the selected dosing regimen.
[0014] Certain embodiments include a computer readable storage medium having instructions stored thereon that, when executed by a processor, cause the processor to perform the method as described herein.
[0015] Also disclosed is a system comprising a processor and a memory, the memory having instructions stored thereon that, when executed by the processor, causes the processor to perform the method as described herein.
[0016] Some embodiments include a method of estimating individual patient PK of a long-acting FIX, the method comprising: (a) receiving, by a computer-based system containing (i) the long-acting FIX population pharmacokinetic (popPK) model of Example 5 or 7 and (ii) a Bayesian estimation program, individual long-acting FIX PK information, b) estimating, by the computer-based system, individualized patient PK information of a long-acting FIX using the FIX popPK model, the Bayesian estimation program, and the received information, and c) outputting, by the computer-based system, the individualized patient PK information. Also disclosed is the method as described herein, further comprising selecting a dosing regimen based on the output individualized patient PK information of (c), and administering the long-acting FIX to the patient according to the selected regimen.
[0017] Certain embodiments include a method of estimating individual patient PK of a long-acting FVIII, the method comprising: (a) receiving, by a computer-based system containing (i) the long-acting FVIII popPK model of Example 9 or 11 or 16 and a Bayesian estimation program, individual long-acting FVIII PK information, b) estimating, by the computer-based system, individualized patient PK information of a long-acting FVIII using the FVIII popPK model, the Bayesian estimation program, and the received information, and c) outputting, by the computer-based system, the individualized patient PK information. Also disclosed is the method as described herein, further comprising selecting a dosing regimen based on the output individualized patient PK information of (c), and administering the long-acting FVIII to the patient according to the selected regimen.
[0018] Some embodiments include a computer readable storage medium having instructions stored thereon that, when executed by a processor, causes the processor to perform the method as described herein.
[0019] Also disclosed is a system comprising a processor and a memory, the memory having instructions stored thereon that, when executed by the processor, cause the processor to perform the method as described herein.
[0020] Some embodiments include the method as described herein, wherein the desired treatment outcome information is desired rise in plasma FIX or FVIII level following dosing and the output information is dose for acute treatment.
[0021] Also disclosed is the method, wherein the desired treatment outcome information is desired dosing interval and the output information is dose for prophylaxis.
[0022] Some embodiments include the method as described herein, wherein the desired treatment outcome information is desired dose and the output information is interval for prophylaxis.
[0023] Also disclosed is the method as described herein, wherein (a) further comprises receiving, by the computer-based system, additional patient information.
[0024] Some embodiments include the method as described herein, wherein the patient information is age or body weight.
[0025] Some embodiments include a web-based method of estimating long-acting FIX dosing information individualized for a patient, the method comprising: (a) receiving, by one or more electronic devices, at least one of patient information and desired treatment outcome information, (b) transmitting, by a processing device, the at least one of patient information and desired treatment outcome information to a web-based application program accessible through a web server, wherein the application is programmed to implement a long-acting FIX population pharmacokinetic (popPK) model of Example 5 or 7 and a Bayesian estimation program, (c) receiving from the web based server and program, individualized dosing information calculated using the popPK model, the Bayesian estimation program, and the transmitted information of (b), and (d) outputting, by the one or more electronic devices, the individualized dosing information.
[0026] Also disclosed is a web-based method of estimating long-acting FVIII dosing information individualized for a patient, the method comprising: (a) receiving, by one or more electronic devices, at least one of patient information and desired treatment outcome information, (b) transmitting, by a processing device, the at least one of patient information and desired treatment outcome information to a web-based application program accessible through a web server, wherein the application is programmed to implement a long-acting FVIII popPK model of Example 9 or 11 or 16, and a Bayesian estimation program, (c) receiving from the web based server and program, individualized dosing information calculated using the popPK model, the Bayesian estimation program, and the transmitted information of (b), and (d) outputting, by the one or more electronic devices, the individualized dosing information.
[0027] Some embodiments include a web-based method of estimating long-acting FIX dosing information individualized for a patient, the method comprising: (a) receiving, by a processing device, at least one of patient information and desired treatment outcome information by a web-based application program accessible through a web server and programmed to implement a long-acting FIX population pharmacokinetic (popPK) model, and a Bayesian estimation program, wherein the received information is transmitted by one or more electronic devices, (b) calculating, by the web-based program, individualized long-acting FIX dosing information using the FIX popPK model, the Bayesian estimation program, and the received information, and (c) transmitting, by a processing device, the individualized calculated dosing information of (b) to one or more electronic devices for output of the information.
[0028] Also disclosed is a web-based method of estimating long-acting FVIII dosing information individualized for a patient, the method comprising: (a) receiving, by a processing device, at least one of patient information and desired treatment outcome information by a web-based application program accessible through a web server and programmed to implement a long-acting FVIII popPK model, and a Bayesian estimation program, wherein the received information is transmitted by one or more electronic devices, (b) calculating, by the web-based program, individualized long-acting FVIII dosing information using the FVIII popPK model of Example 9 or 11 or 16, the Bayesian estimation program, and the received information, and (c) transmitting, by a processing device, the individualized calculated dosing information of (b) to one or more electronic devices for output of the information. In some embodiments, the method as described herein further comprises selecting a dosing regimen based on the output individualized dosing information of (e) and administering the long-acting FIX to the patient according to the selected dosing regimen. In other embodiments, the method as described herein further comprises selecting a dosing regimen based on the output individualized dosing information of (e) and administering the long-acting FVIII to the patient according to the selected dosing regimen.
[0029] Some embodiments include the method as described herein, wherein the desired treatment outcome information is desired rise in plasma FIX activity level following dosing and the dosing output information is dose for acute treatment.
[0030] Also disclosed is the method as described herein, wherein the desired treatment outcome information is desired rise in plasma FVIII activity level following dosing and the dosing output information is dose for acute treatment.
[0031] Some embodiments include is the method as described herein, wherein the desired treatment outcome information is desired dosing interval and the dosing output information is dose for prophylaxis.
[0032] Also disclosed is the method as described herein, wherein, the desired treatment outcome information is desired dose and the dosing output information is interval for prophylaxis.
[0033] Some embodiments include a web-based method of estimating a long-acting FIX dosing regimen based on median FIX popPK, the method comprising: (a) receiving, by one or more electronic devices at least one of patient information and desired treatment outcome information, (b) transmitting, by a processing device, the at least one of patient information and desired treatment outcome information to a web-based application program accessible through a web server, wherein the application is programmed to implement a long-acting FIX population pharmacokinetic (popPK) model, such as that of Example 5 or 7, and a Bayesian estimation program, (c) receiving from the web based server and program, median long-acting FIX PK dosing information calculated using the FIX popPK model, respectively, the Bayesian estimation program, and the received information, and (d) outputting, by the one or more electronic devices, the median PK information.
[0034] Also disclosed is a web-based method of estimating a long-acting FVIII dosing regimen based on median FVIII popPK, the method comprising: (a) receiving, by one or more electronic devices at least one of patient information and desired treatment outcome information, (b) transmitting, by a processing device, the at least one of patient information and desired treatment outcome information to a web-based application program accessible through a web server, wherein the application is programmed to implement a long-acting FVIII population pharmacokinetic (popPK) model, such as that of Example 9 or 11 or 16, and a Bayesian estimation program, (c) receiving from the web based server and program, median long-acting FVIII PK dosing information calculated using the FVIII popPK model, respectively, the Bayesian estimation program, and the received information, and (d) outputting, by the one or more electronic devices, the median PK information.
[0035] Some embodiments include a web-based method of estimating a long-acting FIX dosing regimen based on median FIX popPK, the method comprising: (a) receiving, by a processing device, at least one of patient information and desired treatment outcome information by a web-based application program accessible through a web server and programmed to implement a long-acting FIX popPK model, and a Bayesian estimation program, wherein the received information is transmitted by one or more electronic devices, (b) calculating, by the web-based program, individualized long-acting FIX dosing information using the FIX popPK model, the Bayesian estimation program, and the received information, and (c) transmitting, by a processing device, the individualized calculated dosing information of (b) to one or more electronic devices for output of the information.
[0036] Also disclosed is a web-based method of estimating a long-acting FVIII dosing regimen based on median FVIII popPK, the method comprising: (a) receiving, by a processing device, at least one of patient information and desired treatment outcome information by a web-based application program accessible through a web server and programmed to implement a long-acting FVIII population pharmacokinetic (popPK) model, and a Bayesian estimation program, wherein the received information is transmitted by one or more electronic devices, (b) calculating, by the web-based program, individualized long-acting FVIII dosing information using the FVIII popPK model, the Bayesian estimation program, and the received information, and (c) transmitting, by a processing device, the individualized calculated dosing information of (b) to one or more electronic devices for output of the information. Also disclosed is the method as described herein, further comprising selecting a dosing regimen based on the output median PK information of (e), and (f) administering the long-acting FIX to a patient according to the selected dosing regimen. Some embodiments include the method as described herein, further comprising selecting a dosing regimen based on the output median PK information of (e), and (f) administering the long-acting FVIII to a patient according to the selected dosing regimen.
[0037] Some embodiments include the method as described herein, wherein the desired treatment outcome information is desired rise in plasma FIX activity level following dosing and the dosing output information is dose for acute treatment. Some embodiments include the method as described herein, wherein the desired treatment outcome information is desired rise in plasma FVIII activity level following dosing and the dosing output information is dose for acute treatment. Also disclosed is the method as described herein, wherein the desired treatment outcome information is desired dosing interval and the dosing output information is dose for prophylaxis. Some embodiments include the method as described herein, wherein, the desired treatment outcome information is desired dose and the dosing output information is interval for prophylaxis.
[0038] Also disclosed is a web-based method of method of estimating individual patient PK of a long-acting FIX, the method comprising: (a) receiving, by one or more electronic devices, individual long-acting FIX PK information, (b) transmitting, by a processing device, the individual long-acting FIX PK information to a web-based application program accessible through a web server, wherein the application is programmed to implement a long-acting FIX population pharmacokinetic (popPK) model, such as that of Example 5 or 7, and a Bayesian estimation program, (c) receiving from the web-based server and program, individualized patient long-acting FIX PK information using the popPK model, the Bayesian estimation program, and the transmitted information of (b) and (d) outputting, by the one or more electronic devices, the individualized patient PK information.
[0039] Some embodiments include is a web-based method of estimating individual patient PK of a long-acting FVIII, the method comprising: (a) receiving, by one or more electronic devices, individual long-acting FVIII PK information, (b) transmitting, by a processing device, the individual long-acting FVIII PK information to a web-based application program accessible through a web server, wherein the application is programmed to implement a long-acting FVIII population pharmacokinetic (popPK) model, such as that of Example 9 or 11 or 16, and a Bayesian estimation program, (c) receiving from the web-based server and program, individualized patient long-acting FVIII PK information using the popPK model, the Bayesian estimation program, and the transmitted information of (b) and (d) outputting, by the one or more electronic devices, the individualized patient PK information.
[0040] Also disclosed is a web-based method of estimating individual patient PK of a long-acting FIX, the method comprising: (a) receiving, of individual long-acting FIX PK information by a web-based application program accessible through a web server and programmed to implement a long-acting FIX population pharmacokinetic (popPK) model, such as that of Example 5 or 7, and a Bayesian estimation program, wherein the received information is transmitted by one or more electronic devices, (b) calculating by the web-based program, individualized patient PK information of a long-acting FIX using the FIX popPK model, the Bayesian estimation program and the received information, and (c) transmitting, by a processing device, the estimated individualized patient long-acting FIX PK information of (b) to one or more one or more electronic devices, for output of the information.
[0041] Some embodiments include web-based method of estimating individual patient PK of a long-acting FVIII, the method comprising: (a) receiving, of individual long-acting FVIII PK information by a web-based application program accessible through a web server and programmed to implement a long-acting FVIII popPK model, such as that of Example 9 or 11 or 16, and a Bayesian estimation program, wherein the received information is transmitted by one or more electronic devices, (b) calculating by the web-based program, individualized patient PK information of a long-acting FVIII using the FVIII popPK model, the Bayesian estimation program and the received information, and (c) transmitting, by a processing device, the estimated individualized patient long-acting FVIII PK information of (b) to one or more one or more electronic devices, for output of the information.
[0042] In certain embodiments, the method as described herein further comprises selecting a dosing regimen based on the output estimated patient PK information of (e), and administering the long-acting FIX to the patient according to the selected regimen. In other embodiments, the method as described herein further comprises selecting a dosing regimen based on the output estimated patient PK information of (e), and administering the long-acting FVIII to the patient according to the selected regimen.
[0043] Some embodiments include the method as described herein, further comprising selecting a dosing regimen based on the output estimated patient PK information of (e), and administering the long-acting FIX to the patient according to the selected regimen.
[0044] In certain embodiments, the method as described herein further comprises selecting a dosing regimen based on the output estimated patient PK information of (e), and administering the long-acting FVIII to the patient according to the selected regimen.
[0045] Some embodiments include a web-based method of estimating individual patient PK of a long-acting FIX, the method comprising: (a) receiving, by one or more electronic devices, information regarding individual body weight and (i) desired rise of plasma factor activity level following the dose or (ii) desired dose or desired dose interval, (b) transmitting, by a processing device, the information of (a) to a web-based application program accessible through a web server, wherein the application is programmed to implement a long-acting FIX population pharmacokinetic (popPK) model, such as that of Example 5 or 7, and a Bayesian estimation program, (c) receiving from the web based server and program, individualized patient PK information of a long-acting FIX calculated using the popPK model, the Bayesian estimation program, and the transmitted information of (b), and (d) outputting, by the one or more electronic devices, the estimated patient PK information.
[0046] Also included is a web-based method of estimating individual patient PK of a long-acting FVIII, the method comprising: (a) receiving, by one or more electronic devices, information regarding individual body weight and (i) desired rise of plasma factor activity level following the dose or (ii) desired dose or desired dose interval, (b) transmitting, by a processing device, the information of (a) to a web-based application program accessible through a web server, wherein the application is programmed to implement a long-acting FVIII popPK model, such as that of Example 9 or 11 or 16, and a Bayesian estimation program, (c) receiving from the web based server and program, individualized patient PK information of a long-acting FVIII calculated using the popPK model, the Bayesian estimation program, and the transmitted information of (b), and (d) outputting, by the one or more electronic devices, the estimated patient PK information.
[0047] Some embodiments include a web-based method of estimating individual patient PK of a long-acting FIX, the method comprising: (a) receiving, by one or more electronic devices, information regarding individual body weight and (i) desired rise of plasma factor activity level following the dose or (ii) desired dose or desired dose interval, (b) transmitting, by a processing device, the information of (a) to a web-based application program accessible through a web server, wherein the application is programmed to implement a long-acting FIX population pharmacokinetic (popPK) model, such as that of Example 5 or 7, and a Bayesian estimation program, (c) receiving from the web based server and program, individualized patient PK information of the long-acting FIX calculated using the popPK model, the Bayesian estimation program, and the transmitted information of (b), and (d) outputting, by the one or more electronic devices, the estimated patient PK information.
[0048] Some embodiments include a web-based method of estimating individual patient PK of a long-acting FVIII, the method comprising: (a) receiving, by one or more electronic devices, information regarding individual body weight and (i) desired rise of plasma factor activity level following the dose or (ii) desired dose or desired dose interval, (b) transmitting, by a processing device, the information of (a) to a web-based application program accessible through a web server, wherein the application is programmed to implement a long-acting FVIII popPK model, such as that of Example 9 or 11 or 16, and a Bayesian estimation program, (c) receiving from the web based server and program, individualized patient PK information of the long-acting FVIII calculated using the popPK model, the Bayesian estimation program, and the transmitted information of (b), and (d) outputting, by the one or more electronic devices, the estimated patient PK information.
[0049] In other embodiments, the method as described herein further comprises selecting a dosing regimen based on the output estimated patient PK information of (e), and administering the long-acting FIX to the patient according to the selected regimen. Some embodiments include the method as described herein, further comprising selecting a dosing regimen based on the output estimated patient PK information of (e), and administering the long-acting FIX to the patient according to the selected regimen. Also included is the method as described herein, wherein (a) further comprises receiving, by the electronic device, patient information and (b) further comprises transmitting, by a processing device, the patient information to the web-based application program.
[0050] Some embodiments include the method as described herein, wherein (a) further comprises receiving information by the electronic device information relating to diagnostic (baseline) factor level, dosing history, actual dose, actual time of PK sampling or factor activity level, and (b) further comprises transmitting, by a processing device, the information to the web-based application program.
[0051] Also disclosed is the method as described herein, wherein the individualized patient PK includes a PK curve or a PK parameter selected from incremental recovery (Cmax/Dose), mean residence time, terminal t.sub.1/2, clearance, Vss and AUC/Dose.
[0052] Some embodiments include the method as described herein, wherein the information is desired rise in plasma FIX activity level following dosing and the dosing output information is dose for acute treatment.
[0053] Also disclosed is the method as described herein, wherein the information is desired rise in plasma FVIII activity level following dosing and the dosing output information is dose for acute treatment.
[0054] Some embodiments include the method as described herein, wherein the information is desired dose and the dosing output information is dose for prophylaxis.
[0055] Also disclosed is the method as described herein, wherein, the information is desired dose interval and the dosing output information is interval for prophylaxis.
[0056] Some embodiments include the method as described herein, wherein, the electronic device is selected from a digital pen, a smart phone, a tablet computer, a personal digital assistant, a handheld computer, a laptop computer, a scanner, a camera, and a fax machine.
[0057] Also disclosed is a computer readable storage medium having instructions stored thereon that, when executed by a processor, cause the processor to estimate a long-acting FIX dosing information individualized for a patient, wherein the computer-based system comprises (i) a long-acting FIX population pharmacokinetic (popPK) model of Example 5 or 7 and (ii) a Bayesian estimation program.
[0058] Some embodiments include a computer readable storage medium having instructions stored thereon that, when executed by a processor, cause the processor to estimate a long-acting FVIII dosing information individualized for a patient, wherein the computer-based system comprises (i) a long-acting FVIII population pharmacokinetic (popPK) model of Example 9 or 11 or 16 and (ii) a Bayesian estimation program.
[0059] Also disclosed is a system comprising a processor and a memory, the memory having instructions stored thereon that, when executed by the processor, cause the processor to estimate a long-acting FIX dosing information individualized for a patient, wherein the memory comprises (i) a long-acting FIX population pharmacokinetic (popPK) model of Example 5 or 7 and (ii) a Bayesian estimation program and wherein the system receives at least one of patient information and desired treatment outcome information, calculates individualized long-acting FIX dosing information using the popPK model, the Bayesian estimation program, and the received information, and outputting the individualized dosing information.
[0060] Some embodiments include a system comprising a processor and a memory, the memory having instructions stored thereon that, when executed by the processor, cause the processor to estimate a long-acting FVIII dosing information individualized for a patient, wherein the memory comprises (i) a long-acting FVIII population pharmacokinetic (popPK) model of Example 9 or 11 or 16 and (ii) a Bayesian estimation program and wherein the system receives at least one of patient information and desired treatment outcome information, calculates individualized long-acting FVIII dosing information using the popPK model, the Bayesian estimation program, and the received information, and outputting the individualized dosing information.
[0061] Also disclosed is a method of treating a bleeding episode comprising administering to a subject in need thereof a therapeutic dose of a clotting factor at a dosing interval, wherein the dose and dosing interval are calculated using a web-based application that is accessible through a web server, wherein the application is programmed to implement a clotting factor population pharmacokinetic (popPK) model and a Bayesian estimation program to calculate the dose and dosing interval.
[0062] Also disclosed is a method of treating a bleeding episode comprising (1) calculating a therapeutic dose of a clotting factor and a dosing interval of the clotting factor for a subject in need thereof using a web-based application that is accessible through a web server, wherein the application is programmed to implement a clotting factor population pharmacokinetic (popPK) model and a Bayesian estimation program to calculate the dose and dosing interval and (2) administering the clotting factor at the calculated dose and the dosing interval to the subject.
[0063] In some embodiments, the method further comprises entering individual clotting factor pharmacokinetic information.
[0064] In some embodiments, the method further comprises, optionally contemporaneously, updating the popPK model based on the individual clotting factor pharmacokinetic information.
[0065] In some embodiments, the application continuously updates the popPK model based on newly input clotting factor pharmacokinetic information.
[0066] In some embodiments, the method further comprises, before the calculating, inputting a body weight of the subject.
[0067] In some embodiments, the method further comprises inputting a rise of clotting factor plasma activity level desired following the administrating ("desired rise of clotting factor plasma activity level").
[0068] Also disclosed is the method as described herein, wherein the clotting factor is long-acting. Also disclosed is the method as described herein, wherein the long-acting clotting factor is rFVIIIFc or rFIXFc.
[0069] In some embodiments, the method further comprises, before the calculating, inputting the subject's age. Also disclosed is the method, as described herein, wherein the subject is less than 6 years old, equal to or greater than 6 years old and less than 12 years old, less than 12 years old, or equal to or greater than 12 years old.
[0070] Also disclosed is the method, as described herein, wherein the long-acting clotting factor is rFVIIIFc and the method further comprises, before the calculating, inputting the subject's Von Willebrand Factor (VWF) level.
[0071] In some embodiments, the method further comprises, before the calculating, measuring a clotting factor activity level in plasma at various time points after an initial dose of the clotting factor, wherein individual subject clotting factor pharmacokinetic information is, optionally contemporaneously, calculated based on the clotting factor activity level.
[0072] In some embodiments, the method, further comprises, before the measuring, administering an initial dose of the clotting factor.
[0073] Also disclosed is the method, as described herein wherein the initial dose is a fixed interval dose.
[0074] In some embodiments of the method herein, the clotting factor popPK model is updated, optionally contemporaneously, and is, optionally immediately, available through the web server.
[0075] In some embodiments, the clotting factor popPK model is updated, optionally immediately, after the individual subject clotting factor pharmacokinetic information is added to the application and wherein an updated clotting factor popPK model is available for a next use.
[0076] Some embodiments include a web-based method of, optionally contemporaneously, improving the predictive accuracy of clotting factor dosing information, the method comprising: (a) accessing a web-based application accessible through a web server, the application comprising a dataset comprising clotting factor population pharmacokinetic (popPK) information, (b) inputting individual subject clotting factor pharmacokinetic information into the application to create a new dataset, and (c) calculating, using the application, a clotting factor popPK model using the new dataset.
[0077] Also disclosed is the method as described herein, wherein the calculating is performed automatically or upon request.
[0078] Also disclosed is the method as described herein, wherein the popPK model is used to create a dosing regimen for clotting factor administration to a subject in need thereof.
[0079] In some embodiments, the method further comprises administering to the subject a clotting factor according to the regimen.
[0080] Also disclosed is the method as described herein, wherein the clotting factor is long-acting.
[0081] Also disclosed is the method as described herein, wherein the long-acting clotting factor is rFVIIIFc or rFIXFc.
[0082] Also disclosed is the method as described herein, wherein (a) the clotting factor is rFVIIIFc and the popPK model includes one or more parameters selected from the group consisting of the parameters in Example 9, 11, and 16 (Table 18, 24, 25, or 33), or (b) the clotting factor is rFIXFc and the popPK model includes one or more parameters selected from the group consisting of the parameters in Example 5 or 7 (Table 10, 13, or 14). Also disclosed is the method as described herein, wherein the clotting factor is rFVIIIFc and the popPK model is generated as disclosed in Examples 9, 11, 16, or any combinations thereof. Also disclosed is the method as described herein, wherein one or more parameters for the popPK model are selected from the group consisting of the parameters in Table 18, 24, 25, 33, and any combinations thereof. Also disclosed is the method as described herein, wherein the clotting factor is rFIXFc and the popPK model is generated as disclosed in Example 5, 7, or both. Also disclosed is the method as described herein, wherein one or more parameters for the popPK model are selected from the group consisting of the parameters in Table 10, 13, 14, and any combinations thereof.
[0083] Some embodiments include a system for producing an improved clotting factor regimen to be administered to a subject in need thereof, the system comprising a web-based application accessible through a web server, wherein the application comprises: (a) a first dataset comprising clotting factor population pharmacokinetic (popPK) information, (b) a second dataset comprising the first dataset and individual clotting factor pharmacokinetic information of a subject, and (c) a first regimen for a subject in need thereof calculated by the application using the dataset of (b), wherein the first regimen has improved predictive accuracy in comparison to a second regimen calculated by the application using the dataset of (a).
[0084] Also disclosed is the system, as described herein, wherein the application continuously updates a popPK model based on newly input clotting factor pharmacokinetic information. 122. Also disclosed is the system as described herein, wherein the individual clotting factor pharmacokinetic information of (b) is from the subject of (c) or is from a subject different from the subject of (c).
[0085] Some embodiments include a method of producing an improved clotting factor regimen for administration to a subject in need thereof, the method comprising: (a) accessing a web-based application accessible through a web server, the application comprising a first dataset comprising clotting factor population pharmacokinetic (popPK) information, (b) inputting individual clotting factor pharmacokinetic information into the application to create a second dataset, (c) calculating the regimen for the subject in need thereof using the dataset of (b), wherein the calculated regimen has improved predictive accuracy in comparison to a regimen calculated from the dataset of (a), and (d) recording the calculated regimen.
[0086] Also disclosed is the method as described herein, which comprises recording the calculated regimen on a computer readable storage medium.
[0087] Also disclosed is the method as described herein, wherein the individual clotting factor pharmacokinetic information of (b) is from the subject of (c).
[0088] Also disclosed is the method as described herein, wherein the individual clotting factor pharmacokinetic information of (b) is from a subject different from the subject of (c).
[0089] The method may further comprises producing the recorded regimen.
[0090] The method may further comprise administering the regimen to the subject of (c)
[0091] Also disclosed is the method as described herein, wherein the calculating is performed automatically or upon request.
[0092] Also disclosed is the system or method described herein, wherein the dataset includes data from the popPK model in Examples 9, 11, 16, or any combinations thereof. Also disclosed is the system or method described herein, wherein the data include one or more parameters for the popPK model selected from the group consisting of the parameters in Table 18, 24, 25, 33, and any combinations thereof. Also disclosed is the system or method described herein, wherein the dataset includes data from the popPK model in Example 5, 7, or both. Also disclosed is the system or method described herein, wherein the data include one or more parameters for the popPK model selected from the group consisting of the parameters in Table 10, 13, 14, and any combinations thereof.
[0093] Some embodiments include a method of administering rFVIIIFc to a subject in need thereof, comprising administering to the subject a therapeutic dose of rFVIIIFc at a dosing interval greater than one times longer than the dosing interval required for an equivalent amount of FVIII, wherein the subject is <6 years old or 6 to <12 years old, and wherein the therapeutic dose has at least one pharmacokinetic property, expressed in arithmetic mean with 95% confidence interval, selected from the group consisting of: a terminal half-life of 12.67 (11.23, 14.11) hours, a terminal half-life of 14.88 (11.98, 17.77) hours, a clearance of 3.60 (3.13, 4.07) mL/h/kg, a clearance of 2.78 (2.44, 3.13) mL/h/kg, an incremental recovery of 1.92 (1.80, 2.04) IU/dL per IU/kg, an incremental recovery of 2.44 (2.07, 2.80) IU/dL per IU/kg, a mean recovery time of 17.24 (15.40, 19.07) hours, a recovery time of 20.90 (17.06, 24.74) hours, a volume of distribution at steady state of 58.58 (54.90, 62.27) mL/kg, a volume of distribution at steady state of 52.13 (45.25, 59.01) mL/kg, a dose normalized area under the concentration-time curve of 30.04 (26.45, 33.63) IU*h/dL per IU/kg, and a dose normalized area under the concentration-time curve of 41.87 (34.00, 49.75) IU*h/dL per IU/kg for the older cohort.
[0094] Also disclosed is the method as described herein, the medium as described herein, or the system as described herein, wherein the long-acting FIX polypeptide comprises a FIX portion and a second portion.
[0095] Some embodiments include the method as described herein, wherein the long-acting FVIII polypeptide comprises a FVIII portion and a second portion. Also disclosed is the method as described herein, wherein the second portion is albumin or a fragment thereof or an immunoglobulin constant region or a portion thereof. Some embodiments include the method as described herein, wherein the immunoglobulin constant region or a portion thereof comprises a neonatal Fc receptor (FcRn) or an Fc domain.
[0096] Some embodiments include the method as described herein, wherein the second portion comprises a human Fc. Also disclosed is the method as described herein, wherein the second portion comprises a mutant Fc.
[0097] Also disclosed is the method as described herein, wherein the long-acting FIX polypeptide or the long-acting FVIII polypeptide is in the form of a hybrid comprising a second polypeptide in association with said chimeric polypeptide, wherein said second polypeptide comprises a FcRn BP.
[0098] Some embodiments include the method as described herein, wherein the Factor IX is a human Factor IX. Also disclosed is the method as described herein, wherein the FIX is a mutant Factor IX. Some embodiments include the method as described herein, wherein said Factor VIII is human Factor VIII. Also disclosed is the method as described herein, wherein said Factor VIII has a full or partial deletion of the B domain.
BRIEF DESCRIPTION OF DRAWINGS/FIGURES
[0099] FIG. 1 shows FIXFc study design and CONSORT chart. Efficacy data that were collected outside of the efficacy period were not included in the efficacy analyses. *PK subgroup dosed with rFIX followed by PK assessment and washout (greater than or equal to 5 days) prior to rFIXFc dosing for PK evaluation. rFIX sampling was done as follows: pre-injection, 10 (.+-.2) min, 1 hour (.+-.15 min), 3 hr (.+-.15 min), 6 hr (.+-.15 min), 24 (.+-.2) hr, 48 (.+-.2) hr, 72 (.+-.3) hr, and 96 (.+-.3) hr (4 d) from the start of the injection. rFIXFc sampling was done as follows: pre-injection, 10 (.+-.2) min, 1 hour (.+-.15 min), 3 hr (.+-.15 min), 6 hr (.+-.15 min), 24 (.+-.2) hr, 48 (.+-.2) hr, 96 (.+-.3) hr (4 d), 144 (.+-.3) hr (6 d), 168 (.+-.3) hr (7 d), 192 (.+-.3) hr (8 d), and 240 (.+-.3) hr (10 d) from the start of the injection. Infusion was within 10 minutes. Blood samples were collected over 96 hours for each subject. A repeat PK assessment of rFIXFc was also performed at Week 26. ED=exposure day; PK=pharmacokinetics.
[0100] FIGS. 2A-2C show study design for phase 1/2a (B) and phase 3 (C) clinical trials of a long-acting FIXFc polypeptide (i.e., rFIXFc). FIG. 2C shows rFIXFc sampling schemes.
[0101] FIG. 3 shows a summary of Arm 1 sequential dosing and PK sampling of a long-acting FIX polypeptide (i.e., rFIXFc).
[0102] FIG. 4 shows a diagram of three-compartment pharmacokinetic model of a long-acting FIX polypeptide (i.e., rFIXFc). IV intravenous V.sub.1 volume of compartment 1, V.sub.2 volume of compartment 2, V.sub.3 volume of compartment 3, Q.sub.2 inter-compartmental clearance between compartments 1 and 2, Q.sub.3 inter-compartmental clearance between compartments 1 and 2.
[0103] FIG. 5A shows pairwise comparison of baseline and repeat pharmacokinetics CL estimates for the base model with IOV for a long-acting FIX polypeptide (i.e., rFIXFc).
[0104] FIG. 5B shows pairwise comparison of baseline and repeat pharmacokinetics V.sub.1 estimates for the base model with IOV. Dashed line represents the mean. CL clearance, IOV inter-occasion variability, PK pharmacokinetic, V.sub.1 volume of compartment 1.
[0105] FIG. 6 shows individual PK parameters versus body weight (BW) of a long-acting FIX polypeptide (i.e., rFIXFc).
[0106] FIGS. 7A-7D show goodness-of-fit plots of the final model of FIX activity predicted by the population or individual PK model compared to observed FIX activity. The solid line is the unit line; dashed line represents the linear regression line in (FIG. 7A) and (FIG. 7B) and the LOESS smoother in (FIG. 7C) and (FIG. 7D); DV is observed FIX activity (adjusted for baseline activity and residual decay) and unit is IU/dL (%); PRED is the population FIX activity prediction and unit is IU/dL; IPRED is the individual FIX activity prediction and unit is IU/dL; CWRES is conditional weighted residual; TIME is the time after dose and unit is hour. DV is dependent variable.
[0107] FIGS. 8A-8D show Visual Predictive Check (VPC) plots of the population PK model for 50 IU/kg or 100 IU/kg doses of a long-acting FIX polypeptide (i.e., rFIXFc). Visual predictive check for the final model derived from the modeling dataset (8A and 8B), and the model derived from the full dataset (8C and 8D). The solid and dashed lines are 10th, 50th and 90.sup.th percentiles of the observation (solid) and simulation (dashed), respectively. FIGS. 8A and 8C represent dose groups of 50 IU/kg. FIGS. 8B and 8D represent dose groups of 100 IU/kg.
[0108] FIG. 9 shows validation of the population PK model with the trough/peak records for a long-acting FIX polypeptide (i.e., rFIXFc). R2=0.9857, P<0.001.
[0109] FIG. 10 shows a representative plot of observed and predicted perioperative FIX activity for a long-acting FIX polypeptide (i.e., rFIXFc).
[0110] FIGS. 11A-11C show a population simulation of steady-state FIX activity time profile (5th-95th percentile) for a long-acting FIX polypeptide (i.e., rFIXFc).
[0111] FIG. 12 shows a simulation of steady-state FIX activity vs. time profile for a long-acting FIX polypeptide (i.e., rFIXFc) comparing 50 IU/kg vs 4000 IU once weekly and 100 IU/kg vs 8000 IU every 10 days in 5th to 95th percentile of the population.
[0112] FIG. 13 shows a proposed output for individual PK assessment of a long-acting FIX polypeptide (i.e., rFIXFc) or a long-acting FVIII polypeptide (i.e., rFVIIIFc).
[0113] FIG. 14 shows a proposed output for individualized dosing regimen selection for episodic treatment of a long-acting FIX polypeptide (i.e., rFIXFc) or a long-acting FVIII polypeptide (i.e., rFVIIIFc).
[0114] FIG. 15 shows a proposed output for dosing regimen selections without individualized PK assessment of a long-acting FIX polypeptide (i.e., rFIXFc) or a long-acting FVIII polypeptide (i.e., rFVIIIFc).
[0115] FIG. 16 shows another proposed output for dosing regimen selections without individualized PK assessment of a long-acting FIX polypeptide (i.e., rFIXFc).
[0116] FIG. 17 shows an example computer system that can be used in embodiments for a long-acting FIX polypeptide (i.e., rFIXFc) or a long-acting FVIII polypeptide (i.e., rFVIIIFc).
[0117] FIG. 18 shows a graph plotting the predicted total number of bleeds vs. time under 1% FIX activity level of a long-acting FIX polypeptide (i.e., rFIXFc).
[0118] FIG. 19 shows a graph plotting the predicted total number of bleeds vs. time under 5% FIX activity level of a long-acting FIX polypeptide (i.e., rFIXFc).
[0119] FIG. 20 shows goodness-of-fit plots for the full dataset model of a long-acting FIX polypeptide (i.e., rFIXFc). The solid line is the unit line; dashed line represents the linear regression line in (A) and (B) and the LOESS smoother in (C) and (D); DV is observed FIX activity (adjusted for baseline activity and residual decay) and unit is IU/dL (%); PRED is the prediction by population PK parameter estimates and unit is IU/dL; IPRED is the prediction by individual PK parameter estimates and unit is IU/dL; CWRES is conditional weighted residual; TIME unit is hour; and DV is dependent variable.
[0120] FIG. 21 shows details on the design of the sequential PK subgroup (Arm 1) dosing and PK sampling of a long-acting FVIII polypeptide (i.e., rFVIIIFc).
[0121] FIG. 22 shows patient disposition enrolled in the A-LONG study (N=165) for a long-acting FVIII polypeptide.
[0122] FIG. 23 shows dose modification in Arm 1 (individualized prophylaxis) for a long-acting FVIII polypeptide.
[0123] FIGS. 24A-24D show goodness of fit diagnostic plots for the two-compartment model of pharmacokinetics of long-acting rFVIIIFc. FIG. 24A shows observed (DV) v. predicted (PRED). FIG. 24B shows observed (DV) v. individual predicted (IPRE). FIG. 24C shows conditional weighted residuals (CWRES) v. Predicted (PRED). FIG. 24D shows conditional weighted residuals (CWRES) v. Time (TIME).
[0124] FIGS. 25A-25C show the predicted steady-state activity profiles of selected rFVIIIFc prophylaxis dosing regimens. The line in the middle represents the median; the dark shaded area covers the 25th to 75th percentiles; the light shaded area covers the 5th to 95th percentiles. FIG. 25A shows a dosing regimen of 50 IU/kg at every 3 days. FIG. 25B shows a dosing regimen of 50 IU/kg at every 4 days. FIG. 25C shows a dosing regimen of 50 IU/kg at every 5 days.
[0125] FIG. 26 shows the predicted FVIII activity for the hypothetical perioperative dosing regimen in Table 21 for a long-acting FVIII polypeptide (i.e., rFVIIIFc). The middle line shows the 50 percentile. The light shaded areas represent the 5th to 25th percentile and 75th to 95th percentile. The dark shaded areas represent the 25th to 50th percentile and the 50th to 75th percentile.
[0126] FIG. 27 shows the predicted FVIII activity for the hypothetical perioperative dosing regimen in Table 22 for a long-acting FVIII polypeptide (i.e., rFVIIIFc).
[0127] FIG. 28 is a representative plot comparing the simulated and observed FVIII activities within the first 21 days after the first rFVIIIFc surgical dose (n=13; 9 major surgeries, 4 minor surgeries). The upper line represents the line of identity (unity line); the lower line (linear regression line) is the nonparametric fit of the data.
[0128] FIG. 29 shows another proposed output for dosing regimen selections without individualized PK assessment for a long-acting FVIII polypeptide.
[0129] FIG. 30A-30D show the goodness of fit diagnostics of the final model for rFVIIIFc. FIG. 30A shows Observed (DV) vs Predicted (PRED), and FIG. 30B shows Observed (DV) vs Individual Predicted (IPRE). FIG. 30C shows Conditional Weighted Residuals (CWRES) vs Predicted (PRED) for a long-acting FVIII polypeptide (i.e., rFVIIIFc), and FIG. 30D shows Conditional Weighted Residuals (CWRES) vs Time (TIME) for a long-acting FVIII polypeptide (i.e., rFVIIIFc).
[0130] FIG. 31A shows the visual predictive check (VPC) results (Baseline PK profiles) of the final model for Arm 1 sequential PK group.
[0131] FIG. 31B shows the visual predictive check (VPC) results (Baseline PK profiles) of the final model for Arm 1 non-sequential PK group. For FIGS. 31A and 31B, the 5th, 50th (median), and 95th percentiles of simulated data are represented by the dotted lines and gray shaded area, while the 5th, 50th (median), and 95th percentiles of the observed data are presented as solid lines and solid circles.
[0132] FIG. 31C shows VPC results (Baseline PK profiles) of the final model for Arm 2 (phase 3 study) rFVIIIFc.
[0133] FIG. 31D shows VPC results (Baseline PK profiles) of the final model for Arm 3 (phase 3 study) rFVIIIFc.
[0134] FIG. 31E shows VPC results (Baseline PK profiles) of the final model for Cohort A (phase 1/2a study) rFVIIIFc. FIG. 31F shows VPC results (Baseline PK profiles) of the final model for Cohort B (phase 1/2a study) rFVIIIFc. For FIGS. 31C-F, the 5th, 50th (median), and 95th percentiles of simulated data are represented by the dotted lines and gray shaded area, while the 5th, 50.sup.th, and 95th percentiles of the observed data are presented as solid lines and solid circles.
[0135] FIG. 32 shows the external validation of the rFVIIIFc model. Observed (DV) vs Individual Predicted (IPRE) values from the validation set only.
[0136] FIG. 33A-33B shows the goodness of fit diagnostics of the base model for ADVATE.RTM.. FIG. 33A shows Observed (DV) vs Individual Predicted (IPRE); FIG. 33B shows Conditional Weighted Residuals (CWRES) vs Predicted (PRED).
[0137] FIG. 34 shows an ADVATE.RTM. model comparison. The lower line in the graph is the current model; the upper line is the model reported by Bjorkman et al. Superimposed are the ADVATE.RTM. activity data from the Phase 3 study dataset.
[0138] FIG. 35A-35H show steady state activity profiles of selected rFVIII prophylaxis dosing regimens. FIG. 35A shows 50 IU/dL E3D without uncertainty; FIG. 35B shows 50 IU/dL E3D with uncertainty; FIG. 35C shows 50 IU/dL E4D without uncertainty; FIG. 35D shows 50 IU/dL E4D with uncertainty; FIG. 35E shows 50 IU/dL E5D without uncertainty; FIG. 35F shows 50 IU/dL E5D with uncertainty; FIG. 35G shows 65 IU/dL QW without uncertainty; FIG. 35 H shows 65 IU/dL QW with uncertainty. In FIGS. 35A, 35C, 35E, and 35G, the solid line is the predicted median activity, the dark grey shaded region covers the 25th to 75th percentiles of the predicted activity and the light grey shaded region covers the 5th to 95th percentiles of the predicted activity. In FIGS. 35B, 35D, 35F, and 35H, the middle line is the predicted median activity with the 90% confidence interval around the predictions represented by the grey shaded region. The upper and the lower lines represent the 5th and 95th percentiles of the predicted activity, respectively, along with the corresponding 90% confidence intervals represented by the grey shaded regions.
[0139] FIGS. 36A-36C show a comparison of individual Bayesian parameter estimates for rFVIII and rFVIIIFc. FIG. 36A: Clearance (CL)--Each point represents one individual. Both agents were administered at a nominal dose of 50 IU/kg. FIG. 36B: Central Volume (V.sub.1)--each point represents one individual. The solid line is the identity line. Both agents were administered at a nominal dose of 50 IU/kg. FIG. 36C: Time to 1 IU/dL (Time 1%)--each point represents one individual. The solid line is the identity line. Both agents were administered at a nominal dose of 50 IU/kg.
[0140] FIG. 37 shows the predicted annualized bleeding rate (ABR) correlated with time under the target trough FVIII levels of 1, 3, and 5 IU/dL.
[0141] FIG. 38 shows A-LONG study design for a long-acting FVIII polypeptide (i.e., rFVIIIFc).
[0142] FIG. 39 shows comparison of the number of prophylactic infusions for FVIII (prestudy) and rFVIIIFc (on-study) in Arm-1 subjects.
[0143] FIG. 40 shows comparison of patient-reported, 12 month, prestudy bleeding events and on-study ABR (last 3 months); stratified by last on-study dosing interval.
[0144] FIG. 41 shows simulated dosing regiments: predicted proportion of individuals with steady-state FVIII trough levels above 5 IU/dL (1%).
[0145] FIG. 42 shows time (days) under target FVIII trough levels by treatment arm in the A-LONG study.
[0146] FIG. 43 shows predicted ABR versus time under target trough FVIII levels of 1, 3, and 5 IU/dL, based on (A) the unadjusted NBR model and (B) the adjusted NBR model.
[0147] FIG. 44 shows probability of bleeding versus the time under the target trough FVIII levels of 1, 3, and 5 IU/dL for (A) any bleed, (B) spontaneous bleeds, (C) traumatic bleeds, and (D) joint bleeds.
[0148] FIG. 45 shows a block diagram of an exemplary network-based system 2000 for obtaining an estimated patient individualized dosing information, patient individualized PK information, and patient median PK information.
[0149] FIGS. 46A to 46J show exemplary screen shots of the pharmacokinetic tool (e.g., web-based application) for calculating individual dosing information.
[0150] FIGS. 47A to 47B show exemplary screen shots for inputting user administration (A) and prior therapy information (B).
DETAILED DESCRIPTION OF THE INVENTION
[0151] The present invention provides a computer-based system, e.g., web-based system for estimating individual patient PK of a long-acting FIX protein or a long-acting FVIII protein for treatment of hemophilia, e.g., Hemophilia B or Hemophilia A or a method of estimating individual patient PK of a long-acting FIX protein or a long-acting FVIII protein using the computer-based system, e.g., web-based system.
I. Definitions
[0152] The term "about" is used herein to mean approximately, roughly, around, or in the regions of. When the term "about" is used in conjunction with a numerical range, it modifies that range by extending the boundaries above and below the numerical values set forth. In general, the term "about" is used herein to modify a numerical value above and below the stated value by a variance of 10 percent, up or down (higher or lower).
[0153] The term "polypeptide," "peptide" and "protein" are used interchangeably and refer to a polymeric compound comprised of covalently linked amino acid residues.
[0154] The term "polynucleotide" and "nucleic acid" are used interchangeably and refer to a polymeric compound comprised of covalently linked nucleotide residues. Polynucleotides can be DNA, cDNA, RNA, single stranded, or double stranded, vectors, plasmids, phage, or viruses. Polynucleotides include those in Table 33 or Table 35, which encode the polypeptides of Table 34 or Table 36, respectively. Polynucleotides also include fragments of the polynucleotides of Table 33 or Table 35, e.g., those that encode fragments of the polypeptides of Table 34 or Table 36, such as the Factor IX, Factor VIII, Fc, signal sequence, propeptide, 6His and other fragments of the polypeptides of Table 34 or Table 36.
[0155] The term "administering," as used herein, means to or prescribe or give a pharmaceutically acceptable a long-acting FIX polypeptide or a long-acting FVIII polypeptide of the invention to a subject via a pharmaceutically acceptable route. Examples of routes of administration include, but are not limited to, intravenous, e.g., intravenous injection and intravenous infusion, e.g., via central venous access. Additional routes of administration include subcutaneous, intramuscular, oral, nasal, and pulmonary administration, preferably subcutaneous. A long-acting FIX polypeptide or a long-acting FVIII polypeptide (a FIX or FVIII chimeric or hybrid proteins) can be administered as part of a pharmaceutical composition comprising at least one excipient. Advantages of the present invention include: improved regimen compliance; reduced break through bleeds; increased protection of joints from bleeds; prevention of joint damage; reduced morbidity; reduced mortality; prolonged protection from bleeding; decreased thrombotic events; and improved quality of life.
[0156] The term "chimeric polypeptide," as used herein, means a polypeptide that includes within it at least two polypeptides (or portions thereof such as subsequences or peptides) from different sources. Chimeric polypeptides can include two, three, four, five, six, seven, or more polypeptides or portions thereof from different sources, such as different genes, different cDNAs, or different animal or other species. Chimeric polypeptides can include one or more linkers joining the different polypeptides or portions thereof. Thus, the polypeptides or portions thereof can be joined directly or they can be joined indirectly, via linkers, or both, within a single chimeric polypeptide. Chimeric polypeptides can include additional peptides such as signal sequences and sequences such as 6His and FLAG that aid in protein purification or detection. In addition, chimeric polypeptides can have amino acid or peptide additions to the N- and/or C-termini. Exemplary chimeric polypeptides of the invention are Factor IX-FcRn BP chimeric polypeptides, e.g., FIXFc in SEQ ID NO: 2 (Table 34) or Factor VIII-FcRn BP chimeric polypeptides, e.g., FVIIIFc in SEQ ID NO: 10 (Table 36).
[0157] Factor IX or Factor VIII coagulant activity is expressed as International Unit(s) (IU). Several assays are available for measuring Factor IX activity, including the one stage clotting assay (activated partial thromboplastin time; aPTT), thrombin generation time (TGA) and rotational thromboelastometry (ROTEM.RTM.).
[0158] "Dosing interval," as used herein, means the amount of time that elapses between multiple doses being administered to a subject. Dosing interval can thus be indicated as ranges. The dosing interval in the methods of the invention using a chimeric FIX-FcRn BP, e.g., a chimeric FIX-Fc can be at least about one and one-half to eight times longer than the dosing interval required for an equivalent amount (in IU/kg) of said Factor IX without the FcRn BP, e.g., Fc portion (i.e., a polypeptide consisting of said FIX). Dosing interval can thus be indicated as ranges. The dosing interval in the methods of the invention using a chimeric FVIII-FcRn BP, e.g., a chimeric FVIII-Fc can be at least about one and one-half to eight times longer than the dosing interval required for an equivalent amount (in IU/kg) of said Factor VIII without the FcRn BP, e.g., Fc portion (i.e., a polypeptide consisting of said FVIII).
[0159] The term "dosing frequency" as used herein refers to the frequency of administering doses of a long-acting FIX polypeptide or a long-acting FVIII polypeptide in a given time. Dosing frequency can be indicated as the number of doses per a given time, e.g., once a week or once in two weeks.
[0160] The term "bleeding episode" as used herein is given a standardized definition: A bleeding episode starts from the first sign of a bleed, and ends 72 hours after the last treatment for the bleeding, within which any symptoms of bleeding at the same location, or injections less than or equal to 72 hours apart, is considered the same bleeding episode. See Blanchette V. (2006) Haemophilia 12:124-7. As used herein, any injection to treat the bleeding episode, taken more than 72 hours after the preceding one, is considered the first injection to treat a new bleeding episode at the same location. Likewise, any bleeding at a different location is considered a separate bleeding episode regardless of time from the last injection.
[0161] The term "prophylaxis of one or more bleeding episode" or "prophylactic treatment" as used herein means administering a long-acting FIX polypeptide or a long-acting FVIII polypeptide in multiple doses to a subject over a course of time to increase the level of Factor IX or Factor VIII activity in a subject's plasma. In one embodiment, "prophylaxis of one or more bleeding episode" indicates use of a long-acting FIX polypeptide or a long-acting FVIII polypeptide to prevent or inhibit occurrence of one or more spontaneous or uncontrollable bleeding or bleeding episodes or to reduce the frequency of one or more spontaneous or uncontrollable bleeding or bleeding episodes. In another embodiment, the increased FIX or FVIII activity level is sufficient to decrease the incidence of spontaneous bleeding or to prevent bleeding in the event of an unforeseen injury. Prophylactic treatment decreases or prevents bleeding episodes, for example, those described under on-demand treatment. Prophylactic treatment can be individualized, as discussed under "dosing interval", e.g., to compensate for inter-subject variability.
[0162] The term "about once a week" as used herein means approximate number, and "about once a week" can include every seven days.+-.two days, i.e., every five days to every nine days. The dosing frequency of "once a week" thus can be every five days, every six days, every seven days, every eight days, or every nine days.
[0163] The term "individualized interval prophylaxis" as used herein means use of a long-acting FIX polypeptide or a long-acting FVIII polypeptide for an individualized dosing interval or frequency to prevent or inhibit occurrence of one or more spontaneous and/or uncontrollable bleeding or bleeding episodes or to reduce the frequency of one or more spontaneous and/or uncontrollable bleeding or bleeding episodes. In one embodiment, the "individualized interval" includes every 10 days.+-.3 days, i.e. every seven days to every 13 days. The dosing frequency of the "individualized interval prophylaxis" thus can be ever three days, every seven days, every eight days, every nine days, every ten days, every 11 days, every 12 days, or every 13 days.
[0164] The term "on-demand treatment," as used herein, means treatment that is intended to take place over a short course of time and is in response to an existing condition, such as a bleeding episode, or a perceived short term need such as planned surgery. The "on-demand treatment" is used interchangeably with "episodic" treatment. Conditions that can require on-demand treatment include a bleeding episode, hemarthrosis, muscle bleed, oral bleed, hemorrhage, hemorrhage into muscles, oral hemorrhage, trauma, trauma capitis, gastrointestinal bleeding, intracranial hemorrhage, intra-abdominal hemorrhage, intrathoracic hemorrhage, bone fracture, central nervous system bleeding, bleeding in the retropharyngeal space, bleeding in the retroperitoneal space, or bleeding in the illiopsoas sheath. Bleeding episodes other than these are also included. The subject can be in need of surgical prophylaxis, peri-operative management, or treatment for surgery. Such surgeries include minor surgery, major surgery, tooth extraction, tonsillectomy, other dental/thoraco-facial surgeries, inguinal herniotomy, synovectomy, total knee replacement, other joint replacement, craniotomy, osteosynthesis, trauma surgery, intracranial surgery, intra-abdominal surgery, intrathoracic surgery. Surgeries other than these are also included.
[0165] Additional conditions that can require on-demand treatment include minor hemorrhage, hemarthroses, superficial muscle hemorrhage, soft tissue hemorrhage, moderate hemorrhage, intramuscle or soft tissue hemorrhage with dissection, mucous membrane hemorrhage, hematuria, major hemorrhage, hemorrhage of the pharynx, hemorrhage of the retropharynx, hemorrhage of the retroperitonium, hemorrhage of the central nervous system, bruises, cuts, scrapes, joint hemorrhage, nose bleed, mouth bleed, gum bleed, intracranial bleeding, intraperitoneal bleeding, minor spontaneous hemorrhage, bleeding after major trauma, moderate skin bruising, or spontaneous hemorrhage into joints, muscles, internal organs or the brain. Additional reasons for on-demand treatment include the need for pen-operative management for surgery or dental extraction, major surgery, extensive oral surgery, urologic surgery, hernia surgery, orthopedic surgery such as replacement of knee, hip, or other major joint.
[0166] The term "treatment" or "treating" as used herein means amelioration or reduction of one or more symptoms of bleeding diseases or disorders including, but not limited to, hemophilia B. In one embodiment, "treatment of" or "treating" a bleeding disease or disorder includes prevention of one or more symptoms of a bleeding disease or disorder. In a bleeding disease or disorder caused by a FIX deficiency (e.g., a low baseline FIX activity) or a FVIII deficiency, the term "treatment" or "treating" means a FIX or FVIII replacement therapy. By administering a long-acting FIX polypeptide or a long-acting FVIII polypeptide to a subject, the subject can achieve and/or maintain a plasma trough level of a FIX or FVIII activity at about 1 IU/dl or above 1 IU/dl. In other embodiments, "treatment" or "treating" means reduction of the frequency of one or more symptoms of bleeding diseases or disorders, e.g., spontaneous or uncontrollable bleeding episodes. "Treatment," however, need not be a cure.
[0167] The term "perioperative management" as used herein means use of a long-acting FIX polypeptide or a long-acting FVIII polypeptide before, concurrently with, or after an operative procedure, e.g., a surgical operation. The use for "perioperative management" of one or more bleeding episode includes surgical prophylaxis before (i.e., preoperative), during (i.e., intraoperative), or after (i.e., postoperative) a surgery to prevent one or more bleeding or bleeding episode or reducing or inhibiting spontaneous and/or uncontrollable bleeding episodes before, during, and after a surgery.
[0168] Pharmacokinetic (PK) parameters include the terms above and the following terms, which have their ordinary meaning in the art, unless otherwise indicated. Some of the terms are explained in more detail in the Examples. PK parameters can be based on FIX or FVIII antigen level (often denoted parenthetically herein as "antigen") or FIX or FVIII activity level (often denoted parenthetically herein as "activity"). In the literature, PK parameters are often based on FIX or FVIII activity level due to the presence in the plasma of some subjects of endogenous, inactive FIX or FVIII, which interferes with the ability to measure administered (i.e., exogenous) FIX or FVIII using antibody against FIX or FVIII, respectively. However, when FIX or FVIII is administered as part of a fusion or hybrid protein containing a heterologous polypeptide such as an FcRn BP, administered (i.e., exogenous) FIX or FVIII antigen can be accurately measured using antibody to the heterologous polypeptide. In addition, certain PK parameters can be based on model predicted data (often denoted parenthetically herein as "model predicted") or on observed data (often denoted parenthetically herein as "observed"), and preferably are based on observed data.
[0169] "Baseline," as used herein, is the lowest measured plasma Factor IX or FVIII level in a subject prior to administering a dose. The Factor IX or FVIII plasma levels can be measured at two time points prior to dosing: at a screening visit and immediately prior to dosing. Alternatively, (a) the baseline in subjects whose pretreatment FIX or FVIII activity is <1%, who have no detectable FIX or FVIII antigen, and have nonsense genotypes can be defined as 0%, (b) the baseline for subjects with pretreatment FIX or FVIII activity <1% and who have detectable FIX or FVIII antigen can be set at 0.5%, (c) the baseline for subjects whose pretreatment FIX or FVIII activity is between 1-2% is Cmin (the lowest activity throughout the PK study), and (d) the baseline for subjects whose pretreatment FIX or FVIII activity is .gtoreq.2% can be set at 2%. Activity above the baseline pre-dosing can be considered residue drug from prior treatment, and can be decayed to baseline and subtracted from the PK data following long-acting FIX polypeptide or long-acting FVIII polypeptide dosing.
[0170] "T.sub.1/2.beta.," or "T.sub.1/2 beta" or "Beta HL," as used herein, is half-life associated with elimination phase, t.sub.1/2.beta.=(ln 2)/elimination rate constant associated with the terminal phase. The T.sub.1/2 beta can be measured by FIX or FVIII activity or by FIX or FVIII antigen level in plasma. The T.sub.1/2 beta based on activity is shown as T.sub.1/2 beta (activity), and the T.sub.1/2 beta based on the FIX or FVIII antigen level can be shown as T.sub.1/2 beta (antigen). Both T.sub.1/2 beta (activity) and T.sub.1/2 beta (antigen) can be shown as ranges or a geometric mean.
[0171] "Trough," as used herein, is the lowest plasma Factor IX or FVIII activity level reached after administering a dose of chimeric polypeptide of the invention or another Factor IX or FVIII molecule and before the next dose is administered, if any. Trough is used interchangeably herein with "threshold." Baseline Factor IX or FVIII levels are subtracted from measured Factor IX or FVIII levels to calculate the trough level.
[0172] The term "annualized bleeding rate" ("ABR) as used herein refers to the number of bleeding episodes (including spontaneous and traumatic bleeds) experienced by a subject during a defined time period, extrapolated to 1 year. For example two bleeds in six months would indicate an ABR of four. The median ABR provides a single number to describe all subjects, indicating that half of the subjects had individual ABRs less than or equal to the median and half had ABRs greater than or equal to the median. For example, an ABR can be calculated according to the following formula:
Annualized bleeding rate = Number of bleeding episodes during the efficacy period Total number of days during the efficacy period .times. 365.25 ( C ) ##EQU00001##
[0173] The population pharmacokinetic modeling terms used herein (e.g., model, modeling, validation, dataset) have their ordinary and customary meaning in the field of pharmacokinetics.
[0174] "Immediately," as used herein in reference to updating a popPK model, means that the model is updated as soon as the application performs necessary modeling computations to arrive at an updated model. Thus, "immediately," may reasonably differ in duration of time depending on the hardware and software on which the application is running.
[0175] "Contemporaneously," as used herein in reference to updating, calculating, and inmproving, means shortly after the user has input the information needed to update the popPK model or to calculate the pharmacokinetic information, preferably during the same session in which the user has input the information.
[0176] "Subject," as used herein means a human. Subject as used herein includes an individual who is known to have at least one incidence of uncontrolled bleeding episodes, who has been diagnosed with a disease or disorder associated with uncontrolled bleeding episodes, e.g., a bleeding disease or disorder, e.g., hemophilia A or hemophilia B, who are susceptible to uncontrolled bleeding episodes, e.g., hemophilia, or any combinations thereof. Subjects can also include an individual who is in danger of one or more uncontrollable bleeding episodes prior to a certain activity, e.g., a surgery, a sport activity, or any strenuous activities. The subject can have a baseline FIX or FVIII activity less than 1%, less than 0.5%, less than 2%, less than 2.5%, less than 3%, or less than 4%. Subjects also include pediatric humans. Pediatric human subjects are birth to 20 years, preferably birth to 18 years, birth to 16 years, birth to 15 years, birth to 12 years, birth to 11 years, birth to 6 years, birth to 5 years, birth to 2 years, and 2 to 11 years of age.
[0177] "Therapeutic dose," "dose," "effective dose," or "dosing amount" as used herein, means a dose that achieves a plasma trough level of a FIX or FVIII activity at least about 1 IU/dl or above 1 IU/dl in the subject administered with the long-acting FIX polypeptide or the long-acting FVIII polypeptide. For the purpose of this invention, in one embodiment, the "dose" refers to the amount of the doses that a plasma trough level of a FIX or FVIII activity is maintained at least about 1 IU/dl or above 1 IU/dl, at least about 2 IU/dl or above 2 IU/dl, at least about 3 IU/dl or above 3 IU/dl, at least about 4 IU/dl or above 4 IU/dl, or at least about 5 IU/dl or above 5 IU/dl throughout the administration of the long-acting FIX polypeptide or the long-acting FVIII polypeptide. In another embodiment, the "dose" reduces or decreases frequency of bleeding or bleeding disorder. In other embodiments, the "dose" stops on-going, uncontrollable bleeding or bleeding episodes. In still other embodiments, the "dose" prevents spontaneous bleeding or bleeding episodes in a subject susceptible to such spontaneous bleeding or bleeding episodes. The "dose" or "therapeutic dose" need not cure hemophilia.
[0178] "Variant," as used herein, refers to a polynucleotide or polypeptide differing from the original polynucleotide or polypeptide, but retaining essential properties thereof, e.g., Factor IX coagulant activity or Fc (FcRn binding) activity. Generally, variants are overall closely similar, and, in many regions, identical to the original polynucleotide or polypeptide. Variants include polypeptide and polynucleotide fragments, deletions, insertions, and modified versions of original polypeptides.
II. Methods, Systems, and Storage Medium for Estimating Patient Individualized Dosing Information, Patient Individualized PK Information, and Patient Median PK Information--Long-Acting FIX Polypeptide
[0179] The invention includes a method of estimating a long-acting FIX dosing information individualized for a patient, the method comprising: (a) receiving, by a computer-based system containing the long-acting FIX population pharmacokinetic (popPK) model of Example 5 or 7, e.g., Table 10, 13, or 14, and, optionally, a Bayesian estimation program, at least one of patient information and desired treatment outcome information, (b) calculating, by the computer-based system, individualized long-acting FIX dosing information using the popPK model, the optional Bayesian estimation program, and the received information, and (c) outputting, by the computer-based system, the individualized dosing information.
[0180] In some embodiments, the method also comprises selecting a dosing regimen based on the output individualized dosing information of (c) and administering the long-acting FIX polypeptide to the patient according to the selected dosing regimen.
[0181] In some embodiments, the desired treatment outcome information is desired rise in plasma FIX activity level following dosing and the output information is dose for acute treatment.
[0182] In some embodiments, the desired treatment outcome information is desired dosing interval and the output information is dose for prophylaxis.
[0183] In some embodiments, the desired treatment outcome information is desired dose and the output information is interval for prophylaxis.
[0184] The invention also includes a method of estimating a long-acting FIX dosing regimen based on median popPK, the method comprising: (a) receiving, by a computer-based system containing the long-acting FIX popPK model of Example 5 or 7, e.g., Table 10, 13, or 14, and, optionally, a Bayesian estimation program, at least one of patient information and desired treatment outcome information, (b) calculating, by the computer-based system, median long-acting FIX PK information using the popPK model, the optional Bayesian estimation program, and the received information, and (c) outputting, by the computer-based system, the median PK information.
[0185] In some embodiments, the method also comprises selecting a dosing regimen based on the output median PK information of (c), and administering the long-acting FIX polypeptide to a patient according to the selected dosing regimen.
[0186] The invention also includes a method of estimating individual patient long-acting FIX PK, the method comprising: (a) receiving, by a computer-based system containing the long-acting FIX population pharmacokinetic (popPK) model of Example 5 or 7, e.g., Table 10, 13, or 14, and, optionally, a Bayesian estimation program, individual long-acting FIX PK information, (b) estimating, by the computer-based system, individualized patient long-acting FIX PK information using the popPK model, the optional Bayesian estimation program, and the received information, and (c) outputting, by the computer-based system, the individualized patient PK information.
[0187] In some embodiments, the method also comprises selecting a dosing regimen based on the output individualized patient PK information of (c), and administering the long-acting FIX polypeptide to the patient according to the selected regimen.
[0188] In some embodiments (a) further comprises receiving, by the computer-based system, patient information.
[0189] In some embodiments the patient information is age, e.g., 12 and older, or body weight. Additional patient information includes diagnostic (baseline) FIX level, PK determinations, time of PK sampling, dosing history if PK samples were taken from multiple doses, actual dose, FIX activity level, etc.
[0190] In some embodiments, desired treatment outcome information is, e.g., desired PK or desired regimen outcome, e.g., desired rise in plasma FIX activity level following dose, desired dosing interval, and desired dose.
[0191] In some embodiments, output information is, e.g., PK curve, PK parameter such as incremental recovery (Cmax/dose), mean residence time, terminal t1/2, clearance, Vss, AUC/dose, doses and associated troughs, and intervals and associated troughs.
[0192] For example, for assessing individualized patient PK, the system can recommend that the user input 2-3 optimized PK sampling time points. In this case, system output can include PK curve and one or more selected PK parameters, e.g., incremental recovery (Cmax/Dose), mean residence time, terminal t1/2, clearance, Vss, AUC, and time to 1 or X %, etc. e.g., FIG. 12.
[0193] As additional examples, to select an individualized dosing regimen using the output individual PK parameters discussed in the preceding paragraph, (i) the dose selected for acute treatment can be based on user input of the desired rise in plasma FIX activity level following the dose, (ii) the dose selected for prophylaxis can be based on user input of the desired dosing interval, or (iii) the selected interval for prophylaxis can be based on user input for the desired dose. In the first case, the system can output the dose (IU) based in the patient's incremental recovery, e.g., FIG. 14. In the second case, system output can be a table of doses and associated troughs, e.g., x IU/kg, 1% trough, y IU/kg, 2% trough, etc. e.g., FIG. 15, top. In the third case, system output can be a table of intervals and associated troughs, e.g., x days, 1% trough, y IU/kg, 2% trough, etc., e.g., FIG. 15, bottom.
[0194] The user may wish to use the system without inputting any individualized PK data. In this case, the dosing output would be based on the population median rather than being individualized for the particular patient. E.g., FIG. 15. In this way, the user inputs, e.g., body weight and age, and (i) the desired rise in plasma FIX activity level following the dose, (ii) the desired dose interval for prophylaxis, or (iii) the desired dose for prophylaxis. In the first case, the system can output the dose. In the second case, the system can output the dose and associated trough, e.g., Table 6. In the third case, the system can output the interval and associated trough, e.g., Table 7.
[0195] In some embodiments, the system is compliant with patient privacy laws. In some embodiments, the system is encrypted, e.g., with SSL. In some embodiments, input patient information is made anonymous.
[0196] In some embodiments, the system includes a user help function.
[0197] The method can be carried out by, e.g., a physician, a nurse, or another healthcare practitioner.
[0198] Additional embodiments include a computer readable storage medium having instructions stored thereon that, when executed by a processor, cause the processor to perform any of the methods or processes described herein.
[0199] Additional embodiments include a system comprising a processor and a memory, the memory having instructions stored thereon that, when executed by the processor, cause the processor to perform any of the above methods.
[0200] The user of the system or computer readable storage medium, can be, e.g., a physician, a nurse, or another healthcare practitioner.
[0201] For additional embodiments of these aspects of the invention, see Examples 5 and 7, and the Figures discussed therein.
[0202] Additional embodiments include a computer readable storage medium having instructions stored thereon that, when executed by a processor, cause the processor to perform any of the methods or processes described herein.
[0203] In some embodiments, the system is web-based.
[0204] According to one embodiment, the invention includes a web-based method of estimating a long-acting FIX dosing information individualized for a patient, the method comprising: (a) receiving, by one or more electronic devices, at least one of patient information and desired treatment outcome information, (b) transmitting, by a processing device, the at least one of patient information and desired treatment outcome information to a web-based application program accessible through a web server, wherein the application is programmed to implement a long-acting FIX population pharmacokinetic (popPK) model, such as that of Example 5 or 7, e.g., Table 10, 13, or 14, and, optionally, a Bayesian estimation program, (c) receiving from the web based server and program, individualized dosing information calculated using the popPK model, the optional Bayesian estimation program, and the transmitted information of (b), and (d) outputting, by the one or more electronic devices, the individualized dosing information. In some embodiments, the method also comprises selecting a dosing regimen based on the output individualized dosing information of (d) and administering the long-acting FIX polypeptide to the patient according to the selected dosing regimen.
[0205] In some embodiments, the patient information includes body weight. In some embodiments, the desired treatment outcome information is desired rise in plasma FIX activity level following dosing and the output information is dose for acute treatment. In some embodiments, the desired treatment outcome information is desired dosing interval and the output information is dose for prophylaxis. In some embodiments, the desired treatment outcome information is desired dose and the output information is interval for prophylaxis.
[0206] The invention also includes a web-based method of estimating a long-acting FIX dosing information individualized for a patient, wherein the method comprises: (a) receiving, by a processing device, at least one of patient information and desired treatment outcome information by a web-based application program accessible through a web server and programmed to implement a long-acting FIX population pharmacokinetic (popPK) model, and a Bayesian estimation program, and the received information, and (c) transmitting, by a processing device, the individualized calculated dosing information of (b) to one or more electronic devices for output of the information. In some embodiments, the method also comprises selecting a dosing regimen based on the output individualized dosing information transmitted in (c) and administering the long-acting FIX to the patient according to the selected dosing regimen.
[0207] In some embodiments, the patient information includes body weight. In some embodiments, the desired treatment outcome information is desired rise in plasma FIX activity level following dosing and the output information is dose for acute treatment. In some embodiments, the desired treatment outcome information is desired dosing interval and the output information is dose for prophylaxis. In some embodiments, the desired treatment outcome information is desired dose and the output information is interval for prophylaxis.
[0208] The invention also includes a web-based method of estimating a long-acting FIX dosing information individualized for a patient, the method comprising: (a) receiving, by an electronic device, at least one of patient information and desired treatment outcome, (b) transmitting, by a processing device, the individual long-acting FIX PK information to outcome information to a web-based application program accessible through a web server, and programmed to implement a long-acting FIX population pharmacokinetic (popPK) model, such as that of Example 5 or 7, e.g., Table 10, 13, or 14, and, optionally, a Bayesian estimation program, (c) calculating, by the web-based program, individualized long-acting FIX dosing information using the popPK model, and. Optionally a Bayesian estimation program, and the received information, (d) transmitting, by a processing device, the individualized calculated dosing information of (c) to one or more one or more electronic devices, and (e) outputting, by the one or more electronic devices, the individualized dosing information. In some embodiments, the method also comprises selecting a dosing regimen based on the output individualized dosing information of (e) and administering the long-acting FIX polypeptide to the patient according to the selected dosing regimen. In some embodiments, the method also comprises selecting a dosing regimen based on the output individualized dosing information in (e) and administering the long-acting FIX polypeptide to the patient according to the selected dosing regimen.
[0209] In some embodiments, the patient information includes body weight. In some embodiments, the desired treatment outcome information is desired rise in plasma FIX activity level following dosing and the output information is dose for acute treatment. In some embodiments, the desired treatment outcome information is desired dosing interval and the output information is dose for prophylaxis. In some embodiments, the desired treatment outcome information is desired dose and the output information is interval for prophylaxis.
[0210] The invention also includes a web-based method of estimating a long-acting FIX dosing regimen based on median popPK, the method comprising: (a) receiving, by one or more electronic devices at least one of patient information and desired treatment outcome information, (b) transmitting, by a processing device, the at least one of patient information and desired treatment outcome information to a web-based application program accessible through a web server, wherein the application is programmed to implement a long-acting FIX population pharmacokinetic (popPK) model, such as that of Example 5 or 7, e.g., Table 10, 13, or 14, and a Bayesian estimation program, (c) receiving from the web based server and program, median long-acting FIX PK dosing information calculated using the popPK model, the Bayesian estimation program, and the received information, and (d) outputting, by the one or more electronic devices, the median PK information. In some embodiments, the method also comprises selecting a dosing regimen based on the output median PK information of (e), and (f) administering the long-acting FIX polypeptide to a patient according to the selected dosing regimen. In some embodiments, the method also comprises selecting a dosing regimen based on the output individualized dosing information output in (d) and administering the long-acting FIX polypeptide to the patient according to the selected dosing regimen.
[0211] In some embodiments, the patient information includes body weight. In some embodiments, the desired treatment outcome information is desired rise in plasma FIX activity level following dosing and the output information is dose for acute treatment. In some embodiments, the desired treatment outcome information is desired dosing interval and the output information is dose for prophylaxis. In some embodiments, the desired treatment outcome information is desired dose and the output information is interval for prophylaxis.
[0212] The invention also includes a web-based method of estimating a long-acting FIX dosing regimen based on median popPK, that comprises: (a) receiving, by a processing device, at least one of patient information and desired treatment outcome information by a web-based application program accessible through a web server and programmed to implement a long-acting FIX population pharmacokinetic (popPK) model, and a Bayesian estimation program, wherein the received information is transmitted by one or more electronic devices, (b) calculating, by the web-based program, individualized long-acting FIX dosing information using the popPK model, the Bayesian estimation program, and the received information, and (c) transmitting, by a processing device, the individualized calculated dosing information of (b) to one or more electronic devices for output of the information. In some embodiments, the method also comprises selecting a dosing regimen based on the output individualized dosing information transmitted in (c) and administering the long-acting FIX polypeptide to the patient according to the selected dosing regimen.
[0213] In some embodiments, the desired treatment outcome information is desired rise in plasma FIX activity level following dosing and the output information is dose for acute treatment. In some embodiments, the desired treatment outcome information is desired dosing interval and the output information is dose for prophylaxis. In some embodiments, the desired treatment outcome information is desired dose and the output information is interval for prophylaxis.
[0214] The invention also includes a web-based method of estimating individual patient long-acting FIX PK, the method comprising: (a) receiving, by one or more electronic devices, individual long-acting FIX PK information, (b) transmitting, by a processing device, the individual long-acting FIX PK information to a web-based application program accessible through a web server, wherein the application is programmed to implement a long-acting FIX population pharmacokinetic (popPK) model, such as that of Example 5 or 7, e.g., Table 10, 13, or 14, and a Bayesian estimation program, (c) receiving from the web-based server and program, individualized patient long-acting FIX PK information using the popPK model, the Bayesian estimation program, and the transmitted information of (b) and (d) outputting, by the one or more electronic devices, the individualized patient PK information. In some embodiments the patient information is age or body weight. In some embodiments, the method also comprises selecting a dosing regimen based on the individualized patient PK information output in (d) and administering the long-acting FIX polypeptide to the patient according to the selected dosing regimen.
[0215] The invention also includes a web-based method of estimating a long-acting FIX dosing regimen based on median popPK, the method comprising: (a) receiving, by one or more electronic devices at least one of patient information and desired treatment outcome information, (b) transmitting, by a processing device, the at least one of patient information and desired treatment outcome information to a web-based application program accessible through a web server, wherein the application is programmed to implement a long-acting FIX population pharmacokinetic (popPK) model, such as that of Example 5 or 7, e.g., Table 10, 13, or 14, and, optionally, a Bayesian estimation program, (c) receiving from the web based server and program, median long-acting FIX PK dosing information calculated using the popPK model, the optional Bayesian estimation program, and the received information, and (d) outputting, by the one or more electronic devices, the median PK information. In some embodiments, the method also comprises selecting a dosing regimen based on the output median PK information of (d), and (f) administering long-acting FIX to a patient according to the selected dosing regimen.
[0216] In some embodiments, the desired treatment outcome information is desired rise in plasma FIX activity level following dosing and the output information is dose for acute treatment. In some embodiments, the desired treatment outcome information is desired dosing interval and the output information is dose for prophylaxis. In some embodiments, the desired treatment outcome information is desired dose and the output information is interval for prophylaxis.
[0217] The invention also includes a web-based method of estimating individual patient long-acting FIX PK, the method comprising: (a) receiving, by one or more electronic devices, individual long-acting FIX PK information, (b) transmitting, by a processing device, the individual long-acting FIX PK information to a web-based application program accessible through a web server, wherein the application is programmed to implement a long-acting FIX population pharmacokinetic (popPK) model, such as that of Example 5 or 7, e.g., Table 10, 13, or 14, and, optionally, a Bayesian estimation program, (c) receiving from the web-based server and program, individualized patient long-acting FIX PK information calculated using the popPK model, the optional Bayesian estimation program, and the transmitted information of (b) and (d) outputting, by the one or more electronic devices, the calculated patient PK information. In some embodiments, the method also comprises selecting a dosing regimen based on the output calculated patient PK information of (d) and administering the long-acting FIX polypeptide to the patient according to the selected dosing regimen.
[0218] In particular embodiments, the individual long-acting FIX PK information includes 2-3 PK sampling time points. In some embodiments, the individual long-acting FIX PK information includes one or more of patient body weight, diagnostic (baseline) factor level, dosing history if PK samples were taken from multiple doses, actual dose, actual time of PK sampling, factor activity level and patient body weight.
[0219] In some embodiments the output individualized patient PK includes a PK curve or a PK parameter selected from incremental recovery (Cmax/Dose), mean residence time, terminal t.sub.1/2, clearance, Vss and AUC/Dose. In some embodiments, the desired treatment outcome information based on the individual patient's PK is desired rise in plasma FIX activity level following dosing and the output information is dose for acute treatment.
[0220] The invention also includes a web-based method of estimating individual patient long-acting FIX PK, the method comprising: (a) receiving, of individual long-acting FIX PK information by a web-based application program accessible through a web server, and programmed to implement a long-acting FIX population pharmacokinetic (popPK) model, such as that of Example 5 or 7, e.g., Table 10, 13, or 14, and, optionally, a Bayesian estimation program, wherein the received information is transmitted by one or more electronic devices (b) estimating, by the web-based program, individualized patient long-acting FIX PK information using the popPK model, the optional Bayesian estimation program, and the received information, and (c) transmitting, by a processing device, the estimated individualized patient long-acting FIX PK information of (b) to one or more one or more electronic devices for output of the individualized patient PK information. In some embodiments, the method also comprises selecting a dosing regimen based on the transmitted patient PK information in (c) and administering the long-acting FIX polypeptide to the patient according to the selected dosing regimen.
[0221] In particular embodiments, the individual long-acting FIX PK information includes 2-3 PK sampling time points. In some embodiments, the individual long-acting FIX PK information includes one or more of patient body weight, diagnostic (baseline) factor level, dosing history if PK samples were taken from multiple doses, actual dose, actual time of PK sampling, factor activity level and patient body weight.
[0222] In some embodiments the output individualized patient PK includes a PK curve or a PK parameter selected from incremental recovery (Cmax/Dose), mean residence time, terminal t.sub.1/2, clearance, Vss and AUC/Dose. In some embodiments, the desired treatment outcome information based on the individual patient's PK is desired rise in plasma FIX activity level following dosing and the output information is dose for acute treatment.
[0223] The invention also includes a web-based method of estimating individual patient long-acting FIX PK, the method comprising: (a) receiving, by one or more electronic devices, individual long-acting FIX PK information, (b) transmitting, by a processing device, the individual long-acting FIX PK information to a web-based application program accessible through a web server, and programmed to implement a long-acting FIX population pharmacokinetic (popPK) model, such as that of Example 5 or 7, e.g., Table 10, 13, or 14, and, optionally, a Bayesian estimation program, (c) estimating, by the web-based program, individualized patient long-acting FIX PK information using the popPK model, the optional Bayesian estimation program, and the received information, (d) transmitting, by a processing device, the estimated individualized patient long-acting FIX PK information of (c) to one or more one or more electronic devices, and (e) outputting, by the one or more electronic devices, the individualized patient PK information. In some embodiments, the method also comprises selecting a dosing regimen based on the transmitted patient PK information of (d) and administering the long-acting FIX polypeptide to the patient according to the selected dosing regimen.
[0224] In particular embodiments, the individual long-acting FIX PK information includes 2-3 PK sampling time points. In some embodiments, the individual long-acting FIX PK information includes one or more of patient body weight, diagnostic (baseline) factor level, dosing history if PK samples were taken from multiple doses, actual dose, actual time of PK sampling, factor activity level and patient body weight.
[0225] In some embodiments the output individualized patient PK includes a PK curve or a PK parameter selected from incremental recovery (Cmax/Dose), mean residence time, terminal t1/2, clearance, Vss and AUC/Dose. In some embodiments, the desired treatment outcome information based on the individual patient's PK is desired rise in plasma FIX activity level following dosing and the output information is dose for acute treatment.
[0226] In another embodiment, the invention includes a web-based method of estimating individual patient long-acting FIX PK, the method comprising: (a) receiving, by one or more electronic devices, information regarding individual body weight and (i) desired rise of plasma factor activity level following the dose or (ii) desired dose or desired dose interval, (b) transmitting, by a processing device, the information of (a) to a web-based application program accessible through a web server, wherein the application is programmed to implement a long-acting FIX population pharmacokinetic (popPK) model, such as that of Example 5 or 7, e.g., Table 10, 13, or 14, and a Bayesian estimation program, (c) receiving from the web based server and program, individualized patient long-acting FIX PK information calculated using the popPK model, the Bayesian estimation program, and the transmitted information of (b), and (d) outputting, by the one or more electronic devices, the estimated patient PK information. In some embodiments, the method also comprises selecting a dosing regimen based on the output estimated patient PK information output of (d), and administering the long-acting FIX polypeptide to the patient according to the selected regimen.
[0227] In some embodiments (a) further comprises receiving, by the electronic device patient information and (b) further comprises transmitting, by a processing device, the patient information to the web-based application program. In some embodiments (a) further comprises receiving information, by the electronic device information relating to diagnostic (baseline) factor level, dosing history (if PK samples were taken from multiple doses), actual dose, actual time of PK sampling or factor activity level and (b) further comprises transmitting, by a processing device, the information to the web-based application program. In some embodiments the individualized patient PK includes a PK curve or a PK parameter selected from incremental recovery (Cmax/Dose), mean residence time, terminal t.sub.1/2, clearance, Vss and AUC/Dose.
[0228] In another embodiment, the invention includes a web-based method of estimating individual patient long-acting FIX PK, that comprises: (a) receiving information regarding individual body weight and (i) desired rise of plasma factor activity level following the dose or (ii) desired dose or desired dose interval, wherein the received information is transmitted by one or more electronic devices, (c) estimating, by the web-based program, individualized patient long-acting FIX PK information using the popPK model, the Bayesian estimation program, and the received information, based on population median, and (c) transmitting, by a processing device, the estimated patient PK information of (b) to one or more electronic devices for output of the information. In some embodiments, the method also comprises selecting a dosing regimen based on the estimated patient PK information transmitted in (c), and administering the long-acting FIX polypeptide to the patient according to the selected regimen.
[0229] In some embodiments (a) further comprises receiving, by the electronic device additional patient information and (b) further comprises transmitting, by a processing device, the additional patient information to the web-based application program. In some embodiments (a) further comprises receiving information, by the electronic device information relating to diagnostic (baseline) factor level, dosing history (if PK samples were taken from multiple doses), actual dose, actual time of PK sampling or factor activity level and (b) further comprises transmitting, by a processing device, the information to the web-based application program.
[0230] In another embodiment, the invention includes a web-based method of estimating individual patient long-acting FIX PK, the method comprising: (a) receiving, by one or more electronic devices, patient information regarding individual body weight and (i) desired rise of plasma factor activity level following the dose or (ii) desired dose or desired dose interval, (b) transmitting, by a processing device, the information of (a) to a web-based application program accessible through a web server, and programmed to implement a long-acting FIX population pharmacokinetic (popPK) model, such as that of Example 5 or 7, e.g., Table 10, 13, or 14, and, optionally, a Bayesian estimation program, (c) estimating, by the web-based program, individualized patient long-acting FIX PK information using the popPK model, the optional Bayesian estimation program, and the received information, based on population medium, (d) transmitting, by a processing device, the estimated patient PK information of (c) to one or more electronic devices, and (e) outputting, by the one or more electronic devices, the estimated patient PK information. In some embodiments, the method also comprises selecting a dosing regimen based on the estimated patient PK information of (c), and administering long-acting FIX to the patient according to the selected regimen.
[0231] In some embodiments, a processor (processing device) is an electronic device. In some embodiments, the electronic device is selected from a digital pen, a smart phone, a tablet computer, a personal digital assistant, a handheld computer, a laptop computer, a point-of-sale transaction device, a scanner, a camera, and a fax machine.
[0232] In some embodiments (a) further comprises receiving, by the electronic device patient information and (b) further comprises transmitting, by a processing device, the patient information to the web-based application program. In some embodiments (a) further comprises receiving information, by the electronic device information relating to diagnostic (baseline) factor level, dosing history (if PK samples were taken from multiple doses), actual dose, actual time of PK sampling or factor activity level and (b) further comprises transmitting, by a processing device, the information to the web-based application program. In some embodiments the individualized patient PK includes a PK curve or a PK parameter selected from incremental recovery (Cmax/Dose), mean residence time, terminal t.sub.1/2, clearance, Vss and AUC/Dose.
[0233] In some embodiments, the electronic device is selected from a digital pen, a smart phone, a tablet computer, a personal digital assistant, a handheld computer, a laptop computer, a point-of-sale transaction device, a scanner, a camera, and a fax machine.
[0234] The electronic device can be a general-purpose computer with a processor, local memory, display, and one or more computer input devices such as a keyboard, a mouse and/or a joystick. Alternatively, the electronic device can be a specialized computing device such as, for example, a mobile handset. The electronic device communicates with one or more network-based (e.g., web-based) application programs over one or more networks, such as the Internet. Similar to the electronic device, the network-based (e.g., web-based) application program can be implemented using any general-purpose computer capable of serving data to the electronic device.
[0235] Each of the client, authority, or transmitter may be implemented on any electronic device. Such electronic device can include, but is not limited to, a personal computer, mobile device such as a mobile phone, workstation, embedded system, game console, television, set-top box, or any other computing device. Further, an electronic device can include, but is not limited to, a device having a processor and memory for executing and storing instructions. Software may include one or more applications and an operating system. Hardware can include, but is not limited to, a processor, memory and graphical user interface display. The electronic device may also have multiple processors and multiple shared or separate memory components. For example, the electronic device may be a clustered computing environment or server farm.
[0236] Network 116 can be any network or combination of networks that can carry data communication, and may be referred to herein as a computer network. Such network 116 can include, but is not limited to, a local area network, medium area network, and/or wide area network such as the Internet. Network 116 can support protocols and technology including, but not limited to, World Wide Web protocols and/or services. Intermediate web servers, gateways, or other servers may be provided between components of system 100 depending upon a particular application or environment.
III. Method, System, and Storage Medium for Estimating Patient Individualized Dosing Information, Patient Individualized PK Information, and Patient Median PK Information--FVIII
[0237] The invention also includes a method of estimating a long-acting FVIII dosing information individualized for a patient, the method comprising: (a) receiving, by a computer-based system containing the long-acting FVIII population pharmacokinetic (popPK) model of Example 9 or 11 or 16, e.g., Table 18, 24, 25, or 33, and, optionally, a Bayesian estimation program, at least one of patient information and desired treatment outcome information, (b) calculating, by the computer-based system, individualized long-acting FVIII dosing information using the popPK model, the optional Bayesian estimation program, and the received information, and (c) outputting, by the computer-based system, the individualized dosing information.
[0238] In some embodiments, the method also comprises selecting a dosing regimen based on the output individualized dosing information of (c) and administering the long-acting FVIII polypeptide to the patient according to the selected dosing regimen.
[0239] In some embodiments, the desired treatment outcome information is desired rise in plasma FVIII activity level following dosing and the output information is dose for acute treatment.
[0240] In some embodiments, the desired treatment outcome information is desired dosing interval and the output information is dose for prophylaxis.
[0241] In some embodiments, the desired treatment outcome information is desired dose and the output information is interval for prophylaxis.
[0242] The invention also includes a method of estimating a long-acting FVIII dosing regimen based on median popPK, the method comprising: (a) receiving, by a computer-based system containing the long-acting FVIII popPK model of Example 9 or 11 or 16, e.g., Table 18, 24, 25, or 33, and, optionally, a Bayesian estimation program, at least one of patient information and desired treatment outcome information, (b) calculating, by the computer-based system, median long-acting FVIII PK information using the popPK model, the optional Bayesian estimation program, and the received information, and (c) outputting, by the computer-based system, the median PK information.
[0243] In some embodiments, the method also comprises selecting a dosing regimen based on the output median PK information of (c), and administering the long-acting FVIII polypeptide to a patient according to the selected dosing regimen.
[0244] The invention also includes a method of estimating individual patient long-acting FVIII PK, the method comprising: (a) receiving, by a computer-based system containing the long-acting FVIII population pharmacokinetic (popPK) model of Example 9 or 11 or 16, e.g., Table 18, 24, 25, or 33, and, optionally, a Bayesian estimation program, individual long-acting FVIII PK information, (b) estimating, by the computer-based system, individualized patient long-acting FVIII PK information using the popPK model, the optional Bayesian estimation program, and the received information, and (c) outputting, by the computer-based system, the individualized patient PK information.
[0245] In some embodiments, the method also comprises selecting a dosing regimen based on the output individualized patient PK information of (c), and administering the long-acting FVIII polypeptide to the patient according to the selected regimen.
[0246] In some embodiments (a) further comprises receiving, by the computer-based system, patient information.
[0247] In some embodiments the patient information is age, e.g., 12 and older, Von Willebrand Factor, hematocrit, or body weight. Additional patient information includes diagnostic (baseline) FVIII level, PK determinations, time of PK sampling, dosing history if PK samples were taken from multiple doses, actual dose, FVIII activity level, etc.
[0248] In some embodiments, desired treatment outcome information is, e.g., desired PK or desired regimen outcome, e.g., desired rise in plasma FVIII activity level following dose, desired dosing interval, and desired dose.
[0249] In some embodiments, output information is, e.g., PK curve, PK parameter such as incremental recovery (Cmax/dose), mean residence time, terminal t1/2, clearance, Vss, AUC/dose, doses and associated troughs, and intervals and associated troughs.
[0250] For example, for assessing individualized patient PK, the system can recommend that the user input 2-3 optimized PK sampling time points. In this case, system output can include PK curve and one or more selected PK parameters, e.g., incremental recovery (Cmax/Dose), mean residence time, terminal t1/2, clearance, Vss, AUC, and time to 1 or X %, etc., e.g., FIG. 14.
[0251] As additional examples, to select an individualized dosing regimen using the output individual PK parameters discussed in the preceding paragraph, (i) the dose selected for acute treatment can be based on user input of the desired rise in plasma FVIII activity level following the dose, (ii) the dose selected for prophylaxis can be based on user input of the desired dosing interval, or (iii) the selected interval for prophylaxis can be based on user input for the desired dose. In the first case, the system can output the dose (IU) based in the patient's incremental recovery, e.g., FIG. 14. In the second case, system output can be a table of doses and associated troughs, e.g., x IU/kg, 1% trough, y IU/kg, 2% trough, etc. e.g., FIG. 15, top. In the third case, system output can be a table of intervals and associated troughs, e.g., x days, 1% trough, y IU/kg, 2% trough, etc., e.g., FIG. 15, bottom.
[0252] The user may wish to use the system without inputting any individualized PK data. In this case, the dosing output would be based on the population median rather than being individualized for the particular patient. E.g., FIG. 15. In this way, the user inputs, e.g., body weight and age, and (i) the desired rise in plasma FVIII activity level following the dose, (ii) the desired dose interval for prophylaxis, or (iii) the desired dose for prophylaxis. In the first case, the system can output the dose. In the second case, the system can output the dose and associated trough. E.g., Table 19 In the third case, the system can output the interval and associated trough. E.g., Table 20.
[0253] In some embodiments, the system is compliant with patient privacy laws. In some embodiments, the system is encrypted, e.g., with SSL. In some embodiments, input patient information is made anonymous.
[0254] In some embodiments, the system includes a user help function.
[0255] The method can be carried out by, e.g., a physician, a nurse, or another healthcare practitioner.
[0256] Additional embodiments include a computer readable storage medium having instructions stored thereon that, when executed by a processor, cause the processor to perform any of the above methods.
[0257] Additional embodiments include a system comprising a processor and a memory, the memory having instructions stored thereon that, when executed by the processor, cause the processor to perform any of the above methods.
[0258] The user of the system or computer readable storage medium, can be, e.g., a physician, a nurse, or another healthcare practitioner.
[0259] For additional embodiments of these aspects of the invention, see Examples 9, 10, and 11 and the Figures discussed therein.
[0260] In some embodiments, the system is web-based.
[0261] According to one embodiment, the invention includes a web-based method of estimating a long-acting FVIII dosing information individualized for a patient, the method comprising: (a) receiving, by one or more electronic devices, at least one of patient information and desired treatment outcome information, (b) transmitting, by a processing device, the at least one of patient information and desired treatment outcome information to a web-based application program accessible through a web server, wherein the application is programmed to implement a long-acting FVIII population pharmacokinetic (popPK) model, such as that of Example 9 or 11 or 16, e.g., Table 18, 24, 25, or 33, and, optionally, a Bayesian estimation program, (c) receiving from the web based server and program, individualized dosing information calculated using the popPK model, the optional Bayesian estimation program, and the transmitted information of (b), and (d) outputting, by the one or more electronic devices, the individualized dosing information. In some embodiments, the method also comprises selecting a dosing regimen based on the output individualized dosing information of (d) and administering the long-acting FVIII polypeptide to the patient according to the selected dosing regimen.
[0262] In some embodiments, the patient information includes body weight. In some embodiments, the desired treatment outcome information is desired rise in plasma FVIII activity level following dosing and the output information is dose for acute treatment. In some embodiments, the desired treatment outcome information is desired dosing interval and the output information is dose for prophylaxis. In some embodiments, the desired treatment outcome information is desired dose and the output information is interval for prophylaxis.
[0263] The invention also includes a web-based method of estimating a long-acting FVIII dosing information individualized for a patient, wherein the method comprises: (a) receiving, by a processing device, at least one of patient information and desired treatment outcome information by a web-based application program accessible through a web server and programmed to implement a long-acting FVIII population pharmacokinetic (popPK) model, and a Bayesian estimation program, and the received information, and (c) transmitting, by a processing device, the individualized calculated dosing information of (b) to one or more electronic devices for output of the information. In some embodiments, the method also comprises selecting a dosing regimen based on the output individualized dosing information transmitted in (c) and administering the long-acting FVIII polypeptide to the patient according to the selected dosing regimen.
[0264] In some embodiments, the patient information includes body weight. In some embodiments, the desired treatment outcome information is desired rise in plasma FVIII activity level following dosing and the output information is dose for acute treatment. In some embodiments, the desired treatment outcome information is desired dosing interval and the output information is dose for prophylaxis. In some embodiments, the desired treatment outcome information is desired dose and the output information is interval for prophylaxis.
[0265] The invention also includes a web-based method of estimating a long-acting FVIII dosing information individualized for a patient, the method comprising: (a) receiving, by an electronic device, at least one of patient information and desired treatment outcome, (b) transmitting, by a processing device, the individual long-acting FVIII PK information to outcome information to a web-based application program accessible through a web server, and programmed to implement a long-acting FVIII population pharmacokinetic (popPK) model, such as that of Example 9 or 11 or 16, e.g., Table 18, 24, 25, or 33, and, optionally, a Bayesian estimation program, (c) calculating, by the web-based program, individualized long-acting FVIII dosing information using the popPK model, and optionally a Bayesian estimation program, and the received information, (d) transmitting, by a processing device, the individualized calculated dosing information of (c) to one or more one or more electronic devices, and (e) outputting, by the one or more electronic devices, the individualized dosing information. In some embodiments, the method also comprises selecting a dosing regimen based on the output individualized dosing information of (e) and administering the long-acting FVIII polypeptide to the patient according to the selected dosing regimen. In some embodiments, the method also comprises selecting a dosing regimen based on the output individualized dosing information in (e) and administering the long-acting FVIII polypeptide to the patient according to the selected dosing regimen.
[0266] In some embodiments, the patient information includes body weight. In some embodiments, the desired treatment outcome information is desired rise in plasma FVIII activity level following dosing and the output information is dose for acute treatment. In some embodiments, the desired treatment outcome information is desired dosing interval and the output information is dose for prophylaxis. In some embodiments, the desired treatment outcome information is desired dose and the output information is interval for prophylaxis
[0267] The invention also includes a web-based method of estimating a long-acting FVIII dosing regimen based on median popPK, the method comprising: (a) receiving, by one or more electronic devices at least one of patient information and desired treatment outcome information, (b) transmitting, by a processing device, the at least one of patient information and desired treatment outcome information to a web-based application program accessible through a web server, wherein the application is programmed to implement a long-acting FVIII population pharmacokinetic (popPK) model, such as that of Example 9 or 11 or 16, e.g., Table 18, 24, 25, or 33, and a Bayesian estimation program, (c) receiving from the web based server and program, median long-acting FVIII PK dosing information calculated using the popPK model, the Bayesian estimation program, and the received information, and (d) outputting, by the one or more electronic devices, the median PK information. In some embodiments, the method also comprises selecting a dosing regimen based on the output median PK information of (e), and (f) administering the long-acting FVIII polypeptide to a patient according to the selected dosing regimen. In some embodiments, the method also comprises selecting a dosing regimen based on the output individualized dosing information output in (d) and administering the long-acting FVIII polypeptide to the patient according to the selected dosing regimen.
[0268] In some embodiments, the patient information includes body weight. In some embodiments, the desired treatment outcome information is desired rise in plasma FVIII activity level following dosing and the output information is dose for acute treatment. In some embodiments, the desired treatment outcome information is desired dosing interval and the output information is dose for prophylaxis. In some embodiments, the desired treatment outcome information is desired dose and the output information is interval for prophylaxis.
[0269] The invention also includes a web-based method of estimating a long-acting FVIII dosing regimen based on median popPK, that comprises: (a) receiving, by a processing device, at least one of patient information and desired treatment outcome information by a web-based application program accessible through a web server and programmed to implement a long-acting FVIII population pharmacokinetic (popPK) model, and a Bayesian estimation program, wherein the received information is transmitted by one or more electronic devices, (b) calculating, by the web-based program, individualized long-acting FVIII dosing information using the popPK model, the Bayesian estimation program, and the received information, and (c) transmitting, by a processing device, the individualized calculated dosing information of (b) to one or more electronic devices for output of the information. In some embodiments, the method also comprises selecting a dosing regimen based on the output individualized dosing information transmitted in (c) and administering the long-acting FVIII polypeptide to the patient according to the selected dosing regimen.
[0270] In some embodiments, the desired treatment outcome information is desired rise in plasma FVIII activity level following dosing and the output information is dose for acute treatment. In some embodiments, the desired treatment outcome information is desired dosing interval and the output information is dose for prophylaxis. In some embodiments, the desired treatment outcome information is desired dose and the output information is interval for prophylaxis.
[0271] The invention also includes a web-based method of estimating individual patient long-acting FVIII PK, the method comprising: (a) receiving, by one or more electronic devices, individual long-acting FVIII PK information, (b) transmitting, by a processing device, the individual long-acting FVIII PK information to a web-based application program accessible through a web server, wherein the application is programmed to implement a long-acting FVIII population pharmacokinetic (popPK) model, such as that of Example 9 or 11 or 16, e.g., Table 18, 24, 25, or 33, and a Bayesian estimation program, (c) receiving from the web-based server and program, individualized patient long-acting FVIII PK information using the popPK model, the Bayesian estimation program, and the transmitted information of (b) and (d) outputting, by the one or more electronic devices, the individualized patient PK information. In some embodiments the patient information is age or body weight. In some embodiments, the method also comprises selecting a dosing regimen based on the individualized patient PK information output in (d) and administering the long-acting FVIII polypeptide to the patient according to the selected dosing regimen.
[0272] The invention also includes a web-based method of estimating a long-acting FVIII dosing regimen based on median popPK, the method comprising: (a) receiving, by one or more electronic devices at least one of patient information and desired treatment outcome information, (b) transmitting, by a processing device, the at least one of patient information and desired treatment outcome information to a web-based application program accessible through a web server, wherein the application is programmed to implement a long-acting FVIII population pharmacokinetic (popPK) model, such as that of Example 9 or 11 or 16, e.g., Table 18, 24, 25, or 33, and, optionally, a Bayesian estimation program, (c) receiving from the web based server and program, median long-acting FVIII PK dosing information calculated using the popPK model, the optional Bayesian estimation program, and the received information, and (d) outputting, by the one or more electronic devices, the median PK information. In some embodiments, the method also comprises selecting a dosing regimen based on the output median PK information of (d), and (f) administering the long-acting FVIII polypeptide to a patient according to the selected dosing regimen.
[0273] In some embodiments, the desired treatment outcome information is desired rise in plasma FVIII activity level following dosing and the output information is dose for acute treatment. In some embodiments, the desired treatment outcome information is desired dosing interval and the output information is dose for prophylaxis. In some embodiments, the desired treatment outcome information is desired dose and the output information is interval for prophylaxis.
[0274] The invention also includes a web-based method of estimating individual patient long-acting FVIII PK, the method comprising: (a) receiving, by one or more electronic devices, individual long-acting FVIII PK information, (b) transmitting, by a processing device, the individual long-acting FVIII PK information to a web-based application program accessible through a web server, wherein the application is programmed to implement a long-acting FVIII population pharmacokinetic (popPK) model, such as that of Example 9 or 11 or 16, e.g., Table 18, 24, 25, or 33, and, optionally, a Bayesian estimation program, (c) receiving from the web-based server and program, individualized patient long-acting FVIII PK information calculated using the popPK model, the optional Bayesian estimation program, and the transmitted information of (b) and (d) outputting, by the one or more electronic devices, the calculated patient PK information. In some embodiments, the method also comprises selecting a dosing regimen based on the output calculated patient PK information of (d) and administering the long-acting FVIII polypeptide to the patient according to the selected dosing regimen.
[0275] In particular embodiments, the individual long-acting FVIII PK information includes 2-3 PK sampling time points. In some embodiments, the individual long-acting FVIII PK information includes one or more of patient body weight, diagnostic (baseline) factor level, dosing history if PK samples were taken from multiple doses, actual dose, actual time of PK sampling, factor activity level and patient body weight.
[0276] In some embodiments the output individualized patient PK includes a PK curve or a PK parameter selected from incremental recovery (Cmax/Dose), mean residence time, terminal t1/2, clearance, Vss and AUC/Dose. In some embodiments, the desired treatment outcome information based on the individual patient's PK is desired rise in plasma FIX activity level following dosing and the output information is dose for acute treatment.
[0277] The invention also includes a web-based method of estimating individual patient long-acting FVIII PK, the method comprising: (a) receiving, of individual long-acting FVIII PK information by a web-based application program accessible through a web server, and programmed to implement a long-acting FVIII population pharmacokinetic (popPK) model, such as that of Example 9 or 11 or 16, e.g., Table 18, 24, 25, or 33, and, optionally, a Bayesian estimation program, wherein the received information is transmitted by one or more electronic devices (b) estimating, by the web-based program, individualized patient long-acting FVIII PK information using the popPK model, the optional Bayesian estimation program, and the received information, and (c) transmitting, by a processing device, the estimated individualized patient long-acting FVIII PK information of (b) to one or more one or more electronic devices for output of the individualized patient PK information. In some embodiments, the method also comprises selecting a dosing regimen based on the transmitted patient PK information in (c) and administering the long-acting FVIII polypeptide to the patient according to the selected dosing regimen.
[0278] In particular embodiments, the individual long-acting FVIII PK information includes 2-3 PK sampling time points. In some embodiments, the individual long-acting FVIII PK information includes one or more of patient body weight, diagnostic (baseline) factor level, dosing history if PK samples were taken from multiple doses, actual dose, actual time of PK sampling, factor activity level and patient body weight.
[0279] In some embodiments the output individualized patient PK includes a PK curve or a PK parameter selected from incremental recovery (Cmax/Dose), mean residence time, terminal t1/2, clearance, Vss and AUC/Dose. In some embodiments, the desired treatment outcome information based on the individual patient's PK is desired rise in plasma FVIII activity level following dosing and the output information is dose for acute treatment.
[0280] The invention also includes a web-based method of estimating individual patient long-acting FVIII PK, the method comprising: (a) receiving, by one or more electronic devices, individual long-acting FVIII PK information, (b) transmitting, by a processing device, the individual long-acting FVIII PK information to a web-based application program accessible through a web server, and programmed to implement a long-acting FVIII population pharmacokinetic (popPK) model, such as that of Example 9 or 11 or 16, e.g., Table 18, 24, 25, or 33, and, optionally, a Bayesian estimation program, (c) estimating, by the web-based program, individualized patient long-acting FVIII PK information using the popPK model, the optional Bayesian estimation program, and the received information, (d) transmitting, by a processing device, the estimated individualized patient long-acting FVIII PK information of (c) to one or more one or more electronic devices, and (e) outputting, by the one or more electronic devices, the individualized patient PK information. In some embodiments, the method also comprises selecting a dosing regimen based on the transmitted patient PK information of (d) and administering the long-acting FVIII polypeptide to the patient according to the selected dosing regimen.
[0281] In particular embodiments, the individual long-acting FVIII PK information includes 2-3 PK sampling time points. In some embodiments, the individual long-acting FVIII PK information includes one or more of patient body weight, diagnostic (baseline) factor level, dosing history if PK samples were taken from multiple doses, actual dose, actual time of PK sampling, factor activity level and patient body weight.
[0282] In some embodiments the output individualized patient PK includes a PK curve or a PK parameter selected from incremental recovery (Cmax/Dose), mean residence time, terminal t1/2, clearance, Vss and AUC/Dose. In some embodiments, the desired treatment outcome information based on the individual patient's PK is desired rise in plasma FVIII activity level following dosing and the output information is dose for acute treatment.
[0283] In another embodiment, the invention includes a web-based method of estimating individual patient long-acting FVIII PK, the method comprising: (a) receiving, by one or more electronic devices, information regarding individual body weight and (i) desired rise of plasma factor activity level following the dose or (ii) desired dose or desired dose interval, (b) transmitting, by a processing device, the information of (a) to a web-based application program accessible through a web server, wherein the application is programmed to implement a long-acting FVIII population pharmacokinetic (popPK) model, such as that of Example 9 or 11 or 16, e.g., Table 18, 24, 25, or 33, and a Bayesian estimation program, (c) receiving from the web based server and program, individualized patient long-acting FVIII PK information calculated using the popPK model, the Bayesian estimation program, and the transmitted information of (b), and (d) outputting, by the one or more electronic devices, the estimated patient PK information. In some embodiments, the method also comprises selecting a dosing regimen based on the output estimated patient PK information output of (d), and administering the long-acting FVIII polypeptide to the patient according to the selected regimen.
[0284] In some embodiments (a) further comprises receiving, by the electronic device patient information and (b) further comprises transmitting, by a processing device, the patient information to the web-based application program. In some embodiments (a) further comprises receiving information, by the electronic device information relating to diagnostic (baseline) factor level, dosing history (if PK samples were taken from multiple doses), actual dose, actual time of PK sampling or factor activity level and (b) further comprises transmitting, by a processing device, the information to the web-based application program. In some embodiments the individualized patient PK includes a PK curve or a PK parameter selected from incremental recovery (Cmax/Dose), mean residence time, terminal t1/2, clearance, Vss and AUC/Dose.
[0285] In another embodiment, the invention includes a web-based method of estimating individual patient long-acting FVIII PK, that comprises: (a) receiving information regarding individual body weight and (i) desired rise of plasma factor activity level following the dose or (ii) desired dose or desired dose interval, wherein the received information is transmitted by one or more electronic devices, (c) estimating, by the web-based program, individualized patient long-acting FVIII PK information using the popPK model, the Bayesian estimation program, and the received information, based on population median, and (c) transmitting, by a processing device, the estimated patient PK information of (b) to one or more electronic devices for output of the information. In some embodiments, the method also comprises selecting a dosing regimen based on the estimated patient PK information transmitted in (c), and administering the long-acting FVIII polypeptide to the patient according to the selected regimen.
[0286] In some embodiments (a) further comprises receiving, by the electronic device additional patient information and (b) further comprises transmitting, by a processing device, the additional patient information to the web-based application program. In some embodiments (a) further comprises receiving information, by the electronic device information relating to diagnostic (baseline) factor level, dosing history (if PK samples were taken from multiple doses), actual dose, actual time of PK sampling or factor activity level and (b) further comprises transmitting, by a processing device, the information to the web-based application program.
[0287] In another embodiment, the invention includes a web-based method of estimating individual patient long-acting FVIII PK, the method comprising: (a) receiving, by one or more electronic devices, patient information regarding individual body weight and (i) desired rise of plasma factor activity level following the dose or (ii) desired dose or desired dose interval, (b) transmitting, by a processing device, the information of (a) to a web-based application program accessible through a web server, and programmed to implement a long-acting FVIII population pharmacokinetic (popPK) model, such as that of Example 9 or 11 or 16, e.g., Table 18, 24, 25, or 33, and, optionally, a Bayesian estimation program, (c) estimating, by the web-based program, individualized patient long-acting FVIII PK information using the popPK model, the optional Bayesian estimation program, and the received information, based on population medium, (d) transmitting, by a processing device, the estimated patient PK information of (c) to one or more electronic devices, and (e) outputting, by the one or more electronic devices, the estimated patient PK information. In some embodiments, the method also comprises selecting a dosing regimen based on the estimated patient PK information of (c), and administering the long-acting FVIII polypeptide to the patient according to the selected regimen.
[0288] In some embodiments, a processor (processing device) is an electronic device. In some embodiments, the electronic device is selected from a digital pen, a smart phone, a tablet computer, a personal digital assistant, a handheld computer, a laptop computer, a point-of-sale transaction device, a scanner, a camera, and a fax machine.
[0289] In some embodiments (a) further comprises receiving, by the electronic device patient information and (b) further comprises transmitting, by a processing device, the patient information to the web-based application program. In some embodiments (a) further comprises receiving information, by the electronic device information relating to diagnostic (baseline) factor level, dosing history (if PK samples were taken from multiple doses), actual dose, actual time of PK sampling or factor activity level and (b) further comprises transmitting, by a processing device, the information to the web-based application program. In some embodiments the individualized patient PK includes a PK curve or a PK parameter selected from incremental recovery (Cmax/Dose), mean residence time, terminal t1/2, clearance, Vss and AUC/Dose.
[0290] In some embodiments, the electronic device is selected from a digital pen, a smart phone, a tablet computer, a personal digital assistant, a handheld computer, a laptop computer, a point-of-sale transaction device, a scanner, a camera, and a fax machine.
[0291] The electronic device can be a general-purpose computer with a processor, local memory, display, and one or more computer input devices such as a keyboard, a mouse and/or a joystick. Alternatively, the electronic device can be a specialized computing device such as, for example, a mobile handset. The electronic device communicates with one or more network-based (e.g., web-based) application programs over one or more networks, such as the Internet. Similar to the electronic device, the network-based (e.g., web-based) application program can be implemented using any general-purpose computer capable of serving data to the electronic device.
[0292] Each of the client, authority, or transmitter may be implemented on any electronic device. Such electronic device can include, but is not limited to, a personal computer, mobile device such as a mobile phone, workstation, embedded system, game console, television, set-top box, or any other computing device. Further, an electronic device can include, but is not limited to, a device having a processor and memory for executing and storing instructions. Software may include one or more applications and an operating system. Hardware can include, but is not limited to, a processor, memory and graphical user interface display. The electronic device may also have multiple processors and multiple shared or separate memory components. For example, the electronic device may be a clustered computing environment or server farm.
[0293] Network 116 can be any network or combination of networks that can carry data communication, and may be referred to herein as a computer network. Such network 116 can include, but is not limited to, a local area network, medium area network, and/or wide area network such as the Internet. Network 116 can support protocols and technology including, but not limited to, World Wide Web protocols and/or services. Intermediate web servers, gateways, or other servers may be provided between components of system 100 depending upon a particular application or environment.
[0294] In one embodiment of the present invention, the web-based application allows contemporaneously updating the popPK model based on the individual clotting factor pharmacokinetic information. In another embodiment, the web-based application continuously updates the popPK model based on newly input clotting factor pharmacokinetic information. By contemporaneously updating the popPK model based on the individual clotting factor pharmacokinetic information and/or by continuously updating the popPK model, the user of the application can have an access to the most updated popPK model, thereby obtaining the most accurate dosing information from the web-based application system. In addition, the web-based application allows the user to pool a large amount of information quickly and utilize the information in order to calculate the dosing information of the subject. This type of pooling and analyzing a large amount of information quickly and efficiently for the next user is not available routinely and by human hand.
IV. Exemplary Computing Environments for FVIII and FIX
[0295] Various modeling techniques, dosage calculations, and estimations described herein can be implemented by software, firmware, hardware, or a combination thereof. FIG. 17 illustrates an example computer system 1900 in which the embodiments, or portions thereof, can be implemented as computer-readable code. In one embodiment, for long-acting FIX polypeptide, the modeling of Examples 5 and 7, and/or the patient treatment simulation of Example 6 can be implemented in system 1900. In another embodiment, for long-acting FVIII polypeptide, the modeling of Examples 9 and 11, and/or the patient treatment simulation of Example 10 can be implemented in system 1900.
[0296] Computer system 1900 includes one or more processors, such as processor 1904. Processor 1904 is connected to a communication infrastructure 1906 (for example, a bus or network).
[0297] Computer system 1900 also includes a main memory 1908, preferably random access memory (RAM), and may also include a secondary memory 1910. In accordance with implementations, user interface data may be stored, for example and without limitation, in main memory 1908. Main memory 1908 may include, for example, cache, and/or static and/or dynamic RAM. Secondary memory 1910 may include, for example, a hard disk drive and/or a removable storage drive. Removable storage drive 1914 may include a floppy disk drive, a magnetic tape drive, an optical disk drive, a flash memory, or the like. The removable storage drive 1914 reads from and/or writes to removable storage unit 1916 in a well-known manner. Removable storage unit 1916 may include a floppy disk, magnetic tape, optical disk, etc. which is read by and written to by removable storage drive 1914. As will be appreciated by persons skilled in the relevant art(s), removable storage unit 1916 includes a computer readable storage medium having stored therein computer software and/or data.
[0298] Computer system 1900 may also include a display interface 1902. Display interface 1902 may be adapted to communicate with display unit 1930. Display unit 1930 may include a computer monitor or similar means for displaying graphics, text, and other data received from main memory 1908 via communication infrastructure 1906. In alternative implementations, secondary memory 1910 may include other similar means for allowing computer programs or other instructions to be loaded into computer system 1900. Such means may include, for example, a removable storage unit 1922 and an interface 1920. Examples of such means may include a program cartridge and cartridge interface (such as that found in video game devices), a removable memory chip (such as an EPROM, or PROM) and associated socket, and other removable storage units 1922 and interfaces 1920 which allow software and data to be transferred from the removable storage unit 1922 to computer system 1900.
[0299] Computer system 1900 may also include a communications interface 1924. Communications interface 1924 allows software and data to be transferred between computer system 1900 and external devices. Communications interface 1924 may include a modem, a network interface (such as an Ethernet card), a communications port, a PCMCIA slot and card, or the like. Software and data transferred via communications interface 1924 are in the form of signals which may be electronic, electromagnetic, optical, or other signals capable of being received by communications interface 1924. These signals are provided to communications interface 1924 via a communications path 1926. Communications path 1926 carries signals and may be implemented using wire or cable, fiber optics, a phone line, a cellular phone link, an RF link or other communications channels.
[0300] In this document, the term "computer readable storage medium" is used to generally refer to non-transitory storage media such as removable storage unit 1916, removable storage unit 1922, and a hard disk installed in hard disk drive 1912. Computer readable storage medium can also refer to one or more memories, such as main memory 1908 and secondary memory 1910, which can be memory semiconductors (e.g. DRAMs, etc.). These computer program products are means for providing software to computer system 1900.
[0301] Computer programs (also called computer control logic) are stored in main memory 1908 and/or secondary memory 1910. Computer programs may also be received via communications interface 1924 and stored on main memory 1908 and/or secondary memory 1910. Such computer programs, when executed, enable computer system 1900 to implement embodiments as discussed herein. In particular, the computer programs, when executed, enable processor 1904 to implement processes of the present disclosure, such as certain methods discussed above. Accordingly, such computer programs represent controllers of the computer system 1900. Where embodiments use software, the software may be stored in a computer program product and loaded into computer system 1900 using removable storage drive 1914, interface 1920, or hard drive 1912.
[0302] Embodiments may be directed to computer program products comprising software stored on any computer readable medium. Such software, when executed in one or more data processing device, causes a data processing device(s) to operate as described herein. Embodiments may employ any computer useable or readable medium. Examples of computer readable storage media include, but are not limited to, non-transitory primary storage devices (e.g., any type of random access memory), and non-transitory secondary storage devices (e.g., hard drives, floppy disks, CD ROMS, ZIP disks, tapes, magnetic storage devices, and optical storage devices, MEMS, nano-technological storage device, etc.). Other computer readable media include communication mediums (e.g., wired and wireless communications networks, local area networks, wide area networks, intranets, etc.).
[0303] FIG. 45 illustrates an example of a network-based system 2000 for a long-acting FIX polypeptide or a long-acting FVIII polypeptide, in which the embodiments, or portions thereof, can be implemented as computer-readable code. In one embodiment, for long-acting FIX polypeptide, the modeling of Examples 5 and 7, and/or the patient treatment simulation of Example 6 can be implemented in system 2000. In another embodiment, for long-acting FVIII polypeptide, the modeling of Examples 9 and 11, and/or the patient treatment simulation of Example 10 can be implemented in system 2000.
[0304] Network-based system 2000 includes network 2004 that can be any network or combination of networks that can carry data communication, and may be referred to herein as a computer network. Such network 2004 can include, but is not limited to, a local area network, medium area network, and/or wide area network such as the Internet. Network 2004 can support protocols and technology including, but not limited to, World Wide Web protocols and/or services. Intermediate web servers, gateways, or other servers may be provided between components of system 2000 depending upon a particular application or environment.
[0305] FIG. 45 shows a block diagram of an exemplary network-based system 2000 for obtaining an estimated patient individualized dosing information, patient individualized PK information, and patient median PK information. System 2000 includes an electronic device 2008 that can communicate over network 2004. Electronic device 2008 includes a transmitting engine 2012, and receiving engine 2016. Transmitting engine 2012 may transmit messages over network 2004. For example, transmitting engine 2012 may transmit information associated with dosing information individualized for a patient. Receiving engine 2016 may receive messages over network 2004 (e.g., from server 2020). For example, receiving engine 2016 may receive a response associated with individualized calculated dosing information transmitted over network 2004 by server 2020.
[0306] Electronic device 2008 can include computer system 1900 and can include, but is not limited to, a personal computer, mobile device such as a mobile phone, workstation, embedded system, game console, television, set-top box, or any other computing device. Further, electronic device 2008 can include, but is not limited to, a device having a processor and memory 2017 for executing and storing instructions.
[0307] Server 2020 is web-based or fixed (physical) and includes a receiving engine 2026 and a communications interface 2028. Receiving engine 2026 may receive messages over network 2004 (e.g., from electronic device 2008) and communicate the received message to application program 2032. In one embodiment, application program 2032 can be web-based or computer-based and is programmed to implement a long-acting FIX population pharmacokinetic (popPK) model such as that of Example 5 or 7, and, optionally, a Bayesian estimation program. In another embodiment, application program 2032 is web-based or computer-based and is programmed to implement a long-acting FVIII population pharmacokinetic (popPK) model such as that of Example 9 or 11 or 16, and, optionally, a Bayesian estimation program. Output of application program 2032 may be communicated by communications interface 2028 over network 2004. For example, transmitting engine 2030 may transmit output information associated with dosing information individualized for a patient over network 2004 to electronic device 2008.
V. Administering Long-Acting FIX Polypeptide
[0308] The present invention further comprises administering a dose of a long-acting FIX polypeptide to a human subject in need thereof at a dosing interval, wherein the dose and/or the dosing interval is identified by the web-based or computer based program. Administration of the long-acting FIX polypeptide is a replacement therapy by adding a recombinant FIX to a subject with FIX deficiency. Administration of the long-acting FIX polypeptide can reduce or prevent a number of bleeding or bleeding episodes in the subject.
[0309] The subject for the methods of the invention includes those in need of control or prevention of bleeding or bleeding episodes. The subject can be bleeding at the time of administration or be expected to be bleeding, or can be susceptible to bleeding in minor hemorrhage, hemarthroses, superficial muscle hemorrhage, soft tissue hemorrhage, moderate hemorrhage, intramuscle or soft tissue hemorrhage with dissection, mucous membrane hemorrhage, hematuria, major hemorrhage, hemorrhage of the pharynx, hemorrhage of the retropharynx, hemorrhage of the retroperitonium, hemorrhage of the central nervous system, bruises, cuts, scrapes, joint hemorrhage, nose bleed, mouth bleed, gum bleed, intracranial bleeding, intraperitoneal bleeding, minor spontaneous hemorrhage, bleeding after major trauma, moderate skin bruising, or spontaneous hemorrhage into joints, muscles, internal organs or the brain. Such subjects also include those in need of peri-operative management, such as management of bleeding associated with surgery or dental extraction. In one embodiment, the subject is in need of prophylaxis of one or more bleeding episodes. In another embodiment, the subject is in need of individualized interval prophylaxis. In other embodiments, the subject is in need of on-demand treatment of one or more bleeding episodes. In still other embodiments, the subject is in need of perioperative management of one or more bleeding episodes.
[0310] The present invention also identifies the appropriate dosing amount and the dosing interval that can treat or prevent one or more bleeding episodes. Administration of the appropriate dosing amount for the dosing interval can achieve a plasma trough level of a FIX activity at least about 1 IU/dl or above 1 IU/dl during the interval in a subject administered with a long-acting FIX polypeptide. In one embodiment, the invention includes a dosing amount (or ranges of the dosing amount) and a dosing interval (or ranges of the dosing interval) that can maintain a plasma trough level of a FIX activity at least about 1 IU/dl (1%) or above 1 IU/dl (1%), at least about 2 IU/dl (2%) or above 2 IU/dl (2%), at least about 3 IU/dl (3%) or above 3 IU/dl (3%), at least about 4 IU/dl (4%) or above 4 IU/dl (4%), or at least about 5 IU/dl (5%) or above 5 IU/dl (5%) throughout the interval. In another embodiment, a dosing amount (or ranges of the dosing amount) and a dosing interval (or ranges of the dosing interval) that reduces or decreases frequency of bleeding or bleeding disorder. In other embodiments, the dosing amount (or ranges of the dosing amount) and the dosing interval (or ranges of the dosing interval) of a long-acting FIX polypeptide stops on-going, uncontrollable bleeding or bleeding episodes in a subject administered with the dosing amount during the dosing interval. In still other embodiments, the dosing amount (or ranges of the dosing amount) and the dosing interval (or ranges of the dosing interval) of a long-acting FIX polypeptide prevents spontaneous bleeding or bleeding episodes in a subject susceptible to such spontaneous bleeding or bleeding episodes. Various dosing amounts and dosing intervals are described in International Appl. No. PCT/US2011/043569 filed Jul. 11, 2011 and published as WO 2012/006624 on Jan. 12, 2012, which is incorporated herein by reference in its entirety.
[0311] The doses that can be used in the methods of the invention are about 10 IU/kg to about 200 IU/kg, about 10 IU/kg to about 180 IU/kg, or about 25 IU/kg to about 200 IU/kg. In one embodiment, the dose of a long-acting FIX polypeptide is about 10 IU/kg to about 50 IU/kg, about 10 IU/kg to about 100 IU/kg, about 25 IU/kg to about 75 IU/kg, about 25 IU/kg to about 100 IU/kg, about 25 IU/kg to about 125 IU/kg, about 25 IU/kg to about 150 IU/kg, about 25 IU/kg to about 50 IU/kg, about 50 IU/kg to about 100 IU/kg, about 50 IU/kg to about 150 IU/kg, about 100 IU/kg to about 150 IU/kg, about 150 IU/kg to about 200 IU/kg, or any combinations thereof.
[0312] The dosing interval can, alternatively, be an individualized interval that is determined for each subject based on the population pharmacokinetic data or other information about that subject. The individualized dose/dosing interval combination can be the same as those for fixed interval regimens in the preceding paragraphs, or can differ. The regimen can initially be at a fixed dosing interval, and then it can change to an individualized dosing interval.
[0313] In some embodiments, a dose of a long-acting FIX polypeptide is an amount sufficient for individualized interval prophylaxis of a bleeding episode. In one example, the individualized interval is every nine days, every 10 days, every 11 days, every 12 days, every 13 days, every 14 days, every 15 days, every 16 days, every 17 days, every 18 days, every 19 days or two times monthly.
[0314] In some embodiments, a dose of a long-acting FIX polypeptide is sufficient for on-demand treatment of one or more bleeding episodes. The doses for the on-demand treatment can vary depending on the various factors, e.g., subject's baseline FIX activity, subject's body weight, subject's likelihood of experiencing bleeding episode, and etc. In one example, the doses for the on-demand treatment can be about 10 to about 50, about 15 to about 100, about 20 to about 100, about 20 to about 50, about 50 to about 100, about 10, about 20, about 40, about 50, and about 100 IU/kg.
[0315] In certain embodiments, a dosing amount and a dosing interval combination for a subject is 20 IU/kg once weekly, 40 IU/kg once weekly, 50 IU/kg once weekly, 100 IU/kg every 10 days, and 100 IU/kg every two weeks (or twice monthly). In one embodiment, a dosing frequency for a long-acting FIX polypeptide is about every two weeks or twice monthly. In another embodiment, the dosing frequency is every 7 days for 25-50 IU/kg, every 10-13 days for 50-100 IU/kg, or every 14 days for 100-150 IU/kg. The interval (or frequency) and dose are determined such that the combination of interval (or frequency) and dose will result in a trough level of at least about 1-5 or at least about 1-3, or at least about 1, at least about 2, at least about 3 IU/dl FIX activity in the subject.
[0316] In some embodiments of the invention, an annualized bleeding rate (ABR) of a bleeding episode is controlled by the present methods. For example, the dosing amount and dosing interval can be administered to reduce or decrease an annualized bleeding rate to a certain level. In one embodiment, administration of a long-acting FIX polypeptide at a dose and a dosing interval for prophylaxis of a bleeding episode results in an annual bleeding rate of less than 2, less than 2.5, less than 3, less than 3.5, less than 4, less than 4.5, less than 5, less than 5.5, less than 6, less than 6.5, less than 7, less than 7.5, less than 8, less than 8.5, less than 9, less than 9.5, or less than 10. For example, ABR of weekly prophylaxis of a bleeding episode can be 2.95.
[0317] The long-acting FIX polypeptide of the invention can provide a half-life, e.g., T.sub.1/2beta (activity) or T.sub.1/2beta (antigen), that is longer than wild-type FIX (e.g., a polypeptide consisting of amino acids 1 to 415 of SEQ ID NO: 2; BENEFIX.RTM.; or pdFIX). In one embodiment, a T.sub.1/2beta (activity) of a long-acting FIX polypeptide is at least about 40 hours, at least about 45 hours, at least about 50 hours, at least about 55 hours, at least about 60 hours, at least about 65 hours, at least about 70 hours, at least about 75 hours, at least about 80 hours, at least about 85 hours, at least about 90 hours, at least about 95 hours, at least about 100 hours, at least about 105 hours, at least about 110 hours, at least about 115, at least about 120, at least about 125, at least about 130, at least about 135, at least about 140, at least about 145, at least about 150, at least about 155, at least about 160, at least about 165, at least about 170, at least about 175, at least about 180, at least about 185, at least about 190, or at least about 193 hours.
[0318] In some embodiments, the T.sub.1/2 beta (activity) of a long-acting FIX polypeptide is expressed as a mean. For example, a mean of the T.sub.1/2 beta (activity) of a long-acting FIX polypeptide is at least about 76 hours, at least about 77 hours, at least about 78 hours, at least about 79 hours, at least about 80 hours, at least about 81 hours, at least about 82 hours, at least about 83 hours, at least about 84 hours, at least about 85 hours, at least about 86 hours, at least about 87 hours, at least about 88 hours, at least about 89 hours, at least about 90 hours, at least about 91 hours, or at least about 92 hours. In a specific embodiment, a mean of the T.sub.1/2 beta (activity) of a long-acting FIX polypeptide is 82 hours.
[0319] In other embodiments, the T.sub.1/2 beta (activity) of a long-acting FIX polypeptide is shown as a comparison to a T.sub.1/2 beta (activity) of wild-type mature FIX. In one example, the mean of the T.sub.1/2 beta (activity) is at least about 2.0 fold higher than wild-type mature FIX (a polypeptide consisting of amino acids 1 to 415 of SEQ ID NO: 2, BENEFIX.RTM., or pdFIX). In another example, the mean of the T.sub.1/2 beta (activity) is at least about 2.0 fold, at least about 2.1 fold, at least about 2.2 fold, at least about 2.3 fold, at least about 2.4 fold, at least about 2.5 fold, at least about 2.6 fold, at least about 2.7 fold, at least about 2.8 fold, at least about 2.9 fold, at least about 3.0 fold, at least about 3.1 fold, or at least about 3.2 fold higher than wild-type mature FIX (a polypeptide consisting of amino acids 1 to 415 of SEQ ID NO: 2, BENEFIX.RTM., or pdFIX).
[0320] In certain embodiments of the invention, the method of the invention further comprises measuring a baseline FIX activity of a subject prior to the initial administration of a long-acting FIX polypeptide. Measuring of a baseline FIX activity can employ any known clotting assays in the art, e.g., one step aPTT assay, two step chromogenic assay, ROTEM, TGA, or etc.
[0321] In some embodiments, the method of the invention further comprises measuring a T.sub.1/2beta (activity) or T.sub.1/2beta (antigen) of the long-acting FIX polypeptide in the subject after administration of a long-acting FIX polypeptide.
[0322] Long-Acting FIX Polypeptide
[0323] A long-acting FIX polypeptide useful for the invention is a chimeric polypeptide comprising a FIX polypeptide and a second portion. In one embodiment, the second portion comprises albumin or an FcRn binding partner. Non-limiting examples for the second portion is described elsewhere herein. In certain embodiments, the long-acting FIX is a fusion protein comprising a single molecule of human recombinant coagulation FIX (rFIX) covalently linked to the dimeric Fc domain of immunoglobulin G1 (IgG1) with no intervening sequence. The FIX polypeptide of the invention comprises a functional Factor IX polypeptide in its normal role in coagulation, unless otherwise specified. Thus, the FIX polypeptide includes variant polypeptides that are functional and the polynucleotides that encode such functional variant polypeptides. In one embodiment, the FIX polypeptides are the human, bovine, porcine, canine, feline, and murine FIX polypeptides. The full length polypeptide and polynucleotide sequences of FIX are known, as are many functional variants, e.g., fragments, mutants and modified versions. FIX polypeptides include full-length FIX, full-length FIX minus Met at the N-terminus, full-length FIX minus the signal sequence, mature FIX (minus the signal sequence and propeptide), and mature FIX with an additional Met at the N-terminus. FIX can be made by recombinant means ("recombinant Factor IX" or "rFIX"), i.e., it is not naturally occurring or derived from plasma.
[0324] A great many functional FIX variants are known. International publication number WO 02/040544 A3, which is herein incorporated by reference in its entirety, discloses mutants that exhibit increased resistance to inhibition by heparin at page 4, lines 9-30 and page 15, lines 6-31. International publication number WO 03/020764 A2, which is herein incorporated by reference in its entirety, discloses FIX mutants with reduced T cell immunogenicity in Tables 2 and 3 (on pages 14-24), and at page 12, lines 1-27. International publication number WO 2007/149406 A2, which is herein incorporated by reference in its entirety, discloses functional mutant FIX molecules that exhibit increased protein stability, increased in vivo and in vitro half-life, and increased resistance to proteases at page 4, line 1 to page 19, line 11. WO 2007/149406 A2 also discloses chimeric and other variant FIX molecules at page 19, line 12 to page 20, line 9. International publication number WO 08/118507 A2, which is herein incorporated by reference in its entirety, discloses FIX mutants that exhibit increased clotting activity at page 5, line 14 to page 6, line 5. International publication number WO 09/051717 A2, which is herein incorporated by reference in its entirety, discloses FIX mutants having an increased number of N-linked and/or O-linked glycosylation sites, which results in an increased half-life and/or recovery at page 9, line 11 to page 20, line 2. International publication number WO 09/137254 A2, which is herein incorporated by reference in its entirety, also discloses Factor IX mutants with increased numbers of glycosylation sites at page 2, paragraph [006] to page 5, paragraph [011] and page 16, paragraph [044] to page 24, paragraph [057]. International publication number WO 09/130198 A2, which is herein incorporated by reference in its entirety, discloses functional mutant FIX molecules that have an increased number of glycosylation sites, which result in an increased half-life, at page 4, line 26 to page 12, line 6. International publication number WO 09/140015 A2, which is herein incorporated by reference in its entirety, discloses functional FIX mutants that an increased number of Cys residues, which can be used for polymer (e.g., PEG) conjugation, at page 11, paragraph [0043] to page 13, paragraph [0053]. The FIX polypeptides described in International Application No. PCT/US2011/043569 filed Jul. 11, 2011 and published as WO 2012/006624 on Jan. 12, 2012 are also incorporated herein by reference in its entirety.
[0325] In addition, hundreds of non-functional mutations in FIX have been identified in hemophilia subjects, many of which are disclosed in Table 5, at pages 11-14 of International publication number WO 09/137254 A2, which is herein incorporated by reference in its entirety. Such non-functional mutations are not included in the invention, but provide additional guidance for which mutations are more or less likely to result in a functional FIX polypeptide.
[0326] In one embodiment, the Factor IX (or Factor IX portion of a chimeric polypeptide) can be at least 70%, at least 80%, at least 85%, at least 90%, at least 95%, at least 96%, at least 97%, at least 98%, at least 99%, or 100% identical to a FIX amino acid sequence shown in Table 34A without a signal sequence and propeptide sequence (amino acids 1 to 415 of SEQ ID NO: 2), or alternatively, with a propeptide sequence, or with a propeptide and signal sequence (full length FIX).
[0327] A long-acting FIX polypeptide can be a hybrid FIX polypeptide. Hybrid FIX polypeptide means a combination of a FIX chimeric polypeptide with a second polypeptide. The chimeric polypeptide and the second polypeptide in a hybrid can be associated with each other via non-covalent protein-protein interactions, such as charge-charge or hydrophobic interactions. The chimeric polypeptide and the second polypeptide in a hybrid can be associated with each other via covalent bond(s) such as disulfide bonds. The chimeric peptide and the second peptide can be associated with each other via more than one type of bond, such as non-covalent and disulfide bonds. Hybrids are described in WO 2004/101740, WO 2005/001025, U.S. Pat. Nos. 7,404,956, 7,348,004, and WO 2006/074199, each of which is incorporated herein by reference in its entirety. The second polypeptide can be a second copy of the same chimeric polypeptide or it can be a non-identical chimeric polypeptide. In other embodiments, the second polypeptide is a polypeptide comprising an FcRn BP, e.g., Fc. In some embodiments, the chimeric polypeptide is a Factor IX-FcRn BP, e.g., Factor IX-Fc chimeric polypeptide, and the second polypeptide consists essentially of Fc. See, e.g., Table 34 (SEQ ID NOs: 2 and 4). See, e.g., U.S. Pat. No. 7,404,956, which is incorporated herein by reference in its entirety.
VI. Administering Long-Acting FVIII Polypeptide
[0328] The present invention further comprises administering a dose of a long-acting FVIII polypeptide to a human subject in need thereof at a dosing interval, wherein the dose and/or the dosing interval is identified by the web-based or computer based program. Administration of the long-acting FVIII polypeptide is a replacement therapy by adding a recombinant FVIII to a subject with FVIII deficiency. Administration of the long-acting FVIII polypeptide can reduce or prevent a number of bleeding or bleeding episodes in the subject.
[0329] Treatment of hemophilia A is a replacement therapy targeting restoration of FVIII activity to 1 to 5% of normal levels to prevent spontaneous bleeding (Mannucci, P. M. et al., N. Engl. J. Med. 344:1773-9 (2001), herein incorporated by reference in its entirety).
[0330] In one embodiment, the long-acting FVIII polypeptide is administered at a dosing interval of every three days or longer. In another embodiment, the effective dose is between about 20 IU/kg and about 90 IU/kg. In other embodiments, the effective dose is 20-30 IU/kg, 30-40 IU/kg, 40-50 IU/kg, 50-60 IU/kg, 60-70 IU/kg, 70-80 IU/kg, or 80-90 IU/kg.
[0331] In certain embodiments, administration of a long-acting FVIII polypeptide is for individualized (tailored) prophylaxis and results in an ABR of less than about 5.5, less than about 5.4, less than about 5.3, less than about 5.2, less than about 5.1, less than about 5.0, less than about 4.9, less than about 4.8, less than about 4.7, less than about 4.6, or less than about 4.5.
[0332] In some embodiments, administration of a long-acting FVIII polypeptide is for weekly prophylaxis and results in an ABR of less than about 9.0, less than about 8.9, less than about 8.8, less than about 8.7, less than about 8.6, less than about 8.5, or less than about 8.4.
[0333] In other embodiments, administration of a long-acting FVIII polypeptide is for episodic or on-demand treatment and results in an ABR of less than about 55, less than about 54, less than about 53, less than about 52, less than about 51, less than about 50, less than about 49, less than about 48, or less than about 47.
[0334] In some embodiments, the effective dose for individualized prophylaxis, weekly prophylaxis, or episodic treatment is a fixed dose or a stratified dose. In one aspect, the fixed dose is about 2,000 IU per dose, about 2,500 IU per dose, about 3,000 IU per dose, about 3,500 IU per dose, or about 4,000 IU per dose.
[0335] The dosing interval suitable for administration of a long-acting FVIII polypeptide can be at least about one and one-half times longer than the dosing interval required for an equivalent dose of the Factor VIII without the non-Factor VIII portion (a polypeptide consisting of the Factor VIII portion).
[0336] The dosing interval can be at least about one and one-half to six times longer, one and one-half to five times longer, one and one-half to four times longer, one and one-half to three times longer, or one and one-half to two times longer, than the dosing interval required for an equivalent dose of the Factor VIII without the non-Factor VIII portion (a polypeptide consisting of the Factor VIII portion), e.g., without the Fc portion. The dosing interval can be at least about one and one-half, two, two and one-half, three, three and one-half, four, four and one-half, five, five and one-half or six times longer than the dosing interval required for an equivalent dose of the Factor VIII without the non-Factor VIII portion (a polypeptide consisting of the Factor VIII portion), e.g., without the Fc portion. The dosing interval can be about every three, four, five, six, seven, eight, nine, ten, eleven, twelve, thirteen, or fourteen days or longer.
[0337] The dosing interval can be at least about one and one-half to 5, one and one-half, 2, 3, 4, or 5 days or longer.
[0338] The methods of the invention can be practiced on a subject in need of prophylactic treatment or on-demand treatment.
[0339] The bleeding condition can be caused by a blood coagulation disorder. A blood coagulation disorder can also be referred to as a coagulopathy. In one example, the blood coagulation disorder, which can be treated with a pharmaceutical composition of the current disclosure, is hemophilia. In another example, the blood coagulation disorder that can be treated with a pharmaceutical composition of the present disclosure is hemophilia A.
[0340] In some embodiments, the type of bleeding associated with the bleeding condition is selected from hemarthrosis, muscle bleed, oral bleed, hemorrhage, hemorrhage into muscles, oral hemorrhage, trauma, trauma capitis, gastrointestinal bleeding, intracranial hemorrhage, intra-abdominal hemorrhage, intrathoracic hemorrhage, bone fracture, central nervous system bleeding, bleeding in the retropharyngeal space, bleeding in the retroperitoneal space, and bleeding in the illiopsoas sheath.
[0341] In other embodiments, the subject suffering from bleeding condition is in need of treatment for surgery, including, e.g., surgical prophylaxis or pen-operative management. In one example, the surgery is selected from minor surgery and major surgery. Exemplary surgical procedures include tooth extraction, tonsillectomy, inguinal herniotomy, synovectomy, craniotomy, osteosynthesis, trauma surgery, intracranial surgery, intra-abdominal surgery, intrathoracic surgery, joint replacement surgery (e.g., total knee replacement, hip replacement, and the like), heart surgery, and caesarean section.
[0342] Long-Acting FVIII Polypeptide
[0343] A "B domain" of Factor VIII, as used herein, is the same as the B domain known in the art that is defined by internal amino acid sequence identity and sites of proteolytic cleavage by thrombin, e.g., residues Ser741-Arg1648 of full length mature human factor VIII. The other human factor VIII domains are defined by the following amino acid residues: A1, residues Ala1-Arg372; A2, residues Ser373-Arg740; A3, residues Ser1690-Ile2032; C1, residues Arg2033-Asn2172; C2, residues Ser2173-Tyr2332. The A3-C1-C2 sequence includes residues Ser1690-Tyr2332. The remaining sequence, residues Glu1649-Arg1689, is usually referred to as the factor VIII light chain activation peptide. The locations of the boundaries for all of the domains, including the B domains, for porcine, mouse and canine factor VIII are also known in the art. In one embodiment, the B domain of Factor VIII is deleted ("B domain deleted factor VIII" or "BDD FVIII"). An example of a BDD FVIII is REFACTO.RTM. (recombinant BDD FVIII), which has the same sequence as the Factor VIII portion of the sequence in Table 36A(i) (amino acids 1 to 1457 of SEQ ID NO: 6 or 20 to 1457 of SEQ ID NO: 10). In another embodiment, the B domain deleted Factor VIII contains an intact intracellular processing site, which corresponds to Arginine at residue 754 of B domain deleted Factor VIII, which corresponds to Arginine residue 773 of SEQ ID NO: 6, or residue 1648 of full-length Factor VIII, which corresponds to Arginine residue 1667 of SEQ ID NO: 10. The sequence residue numbers used herein without referring to any SEQ ID Numbers correspond to the Factor VIII sequence without the signal peptide sequence (19 amino acids) unless otherwise indicated. For example, 5743/Q1638 of full-length Factor VIII corresponds to 5762/Q1657 of SEQ ID NO: 10 due to the 19 amino acid signal peptide sequence. In other embodiments, the B domain deleted FVIII comprises a substitution or mutation at an amino acid position corresponding to Arginine 1645, a substitution or mutation at an amino acid position corresponding to Arginine 1648, or a substitution or mutation at amino acid positions corresponding to Arginine 1645 and Arginine 1648 in full-length Factor VIII. In some embodiments, the amino acid substituted at the amino acid position corresponding to Arginine 1645 is a different amino acid from the amino acid substituted at the amino acid position corresponding to Arginine 1648. In certain embodiments, the substitution or mutation is an amino acid other than arginine, e.g., alanine.
[0344] A "B domain deleted factor VIII" can have the full or partial deletions disclosed in U.S. Pat. Nos. 6,316,226, 6,346,513, 7,041,635, 5,789,203, 6,060,447, 5,595,886, 6,228,620, 5,972,885, 6,048,720, 5,543,502, 5,610,278, 5,171,844, 5,112,950, 4,868,112, and 6,458,563, each of which is incorporated herein by reference in its entirety. In some embodiments, a B domain deleted factor VIII sequence of the present invention comprises any one of the deletions disclosed at col. 4, line 4 to col. 5, line 28 and examples 1-5 of U.S. Pat. No. 6,316,226 (also in U.S. Pat. No. 6,346,513). In some embodiments, a B domain deleted factor VIII of the present invention has a deletion disclosed at col. 2, lines 26-51 and examples 5-8 of U.S. Pat. No. 5,789,203 (also U.S. Pat. Nos. 6,060,447, 5,595,886, and 6,228,620). In some embodiments, a B domain deleted factor VIII has a deletion described in col. 1, lines 25 to col. 2, line 40 of U.S. Pat. No. 5,972,885; col. 6, lines 1-22 and example 1 of U.S. Pat. No. 6,048,720; col. 2, lines 17-46 of U.S. Pat. No. 5,543,502; col. 4, line 22 to col. 5, line 36 of U.S. Pat. No. 5,171,844; col. 2, lines 55-68, FIG. 2, and example 1 of U.S. Pat. No. 5,112,950; col. 2, line 2 to col. 19, line 21 and Table 2 of U.S. Pat. No. 4,868,112; col. 2, line 1 to col. 3, line 19, col. 3, line 40 to col. 4, line 67, col. 7, line 43 to col. 8, line 26, and col. 11, line 5 to col. 13, line 39 of U.S. Pat. No. 7,041,635; or col. 4, lines 25-53, of U.S. Pat. No. 6,458,563. In some embodiments, a B domain deleted factor VIII has a deletion of most of the B domain, but still contains amino-terminal sequences of the B domain that are essential for in vivo proteolytic processing of the primary translation product into two polypeptide chain (i.e., intracellular processing site), as disclosed in WO 91/09122, which is incorporated herein by reference in its entirety. In some embodiments, a B domain deleted factor VIII is constructed with a deletion of amino acids 747-1638, i.e., virtually a complete deletion of the B domain. Hoeben R. C., et al. J. Biol. Chem. 265 (13): 7318-7323 (1990), incorporated herein by reference in its entirety. A B domain deleted factor VIII can also contain a deletion of amino acids 771-1666 or amino acids 868-1562 of factor VIII. Meulien P., et al. Protein Eng. 2(4): 301-6 (1988), incorporated herein by reference in its entirety. Additional B domain deletions that are part of the invention include, e.g., deletion of amino acids 982 through 1562 or 760 through 1639 (Toole et al., Proc. Natl. Acad. Sci. U.S.A. 83:5939-5942 (1986)), 797 through 1562 (Eaton et al., Biochemistry 25:8343-8347 (1986)), 741 through 1646 (Kaufman (PCT published application No. WO 87/04187)), 747-1560 (Sarver et al., DNA 6:553-564 (1987)), 741 through 1648 (Pasek (PCT application No. 88/00831)), 816 through 1598 or 741 through 1689 (Lagner (Behring Inst. Mitt. (1988) No 82:16-25, EP 295597)), each of which is incorporated herein by reference in its entirety. In some embodiments, B domain deleted FVIII comprises a partial deletion in B domain, i.e., having 21 amino acids from B domain (i.e., SFSQNSRHPSQNPPVLKRHQR, which is SEQ ID NO: 11) disclosed in US Publication No. 20100286067 and US Publication No. US 20120093840, both of which are incorporated herein by reference in their entireties. Each of the foregoing deletions can be made in any Factor VIII sequence. Each of the foregoing deletions can be made in any Factor VIII sequence.
[0345] In one embodiment, the B domain deleted Factor VIII portion in the long-acting FVIII polypeptide is processed into two chains connected (or associated) by a metal bond, the first chain comprising a heavy chain (A1-A2-partial B) and a second chain comprising a light chain (A3-C1-C2). In another embodiment, the B domain deleted Factor VIII portion is a single chain Factor VIII. The single chain Factor VIII can comprise an intracellular processing site, which corresponds to Arginine at residue 754 of B domain deleted Factor VIII (residue 773 of SEQ ID NO: 6) or at residue 1648 of full-length Factor VIII (residue 1657 of SEQ ID NO: 10).
[0346] The metal bond between the heavy chain and the light chain can be any metal known in the art. For example, the metals useful for the invention can be a divalent metal ion. The metals that can be used to associate the heavy chain and light chain include, but not limited to, Ca.sup.2+, Mn.sup.2+, or Cu.sup.2+. Fatouros et al., Intern. J. Pharm. 155(1): 121-131 (1997); Wakabayashi et al., JBC. 279(13): 12677-12684 (2004).
[0347] The long-acting FVIII polypeptide can comprise a sequence at least 60%, 70%, 80%, 90%, 95%, 96%, 97%, 98%, 99%, or 100% identical to the Factor VIII and Fc amino acid sequence shown in Table 36A(i) without a signal sequence (amino acids 20 to 1684 of SEQ ID NO: 6) or at least 60%, 70%, 80%, 90%, 95%, 96%, 97%, 98%, 99%, or 100% identical to the Factor VIII and Fc amino acid sequence shown in Table 36A(i) with a signal sequence (amino acids 1 to 1684 of SEQ ID NO: 6), wherein the sequence has Factor VIII activity. The Factor VIII activity can be measured by activated Partial Thromboplastin Time (aPPT) assay, chromogenic assay, or other known methods. The chimeric polypeptide can comprise a sequence identical to the Factor VIII and Fc amino acid sequence shown in Table 36A(i) without a signal sequence (amino acids 20 to 1684 of SEQ ID NO: 6) or identical to the Factor VIII and Fc amino acid sequence shown in Table 36A(i) with a signal sequence (amino acids 1 to 1684 of SEQ ID NO: 6).
[0348] The Factor VIII polypeptide as used herein is functional factor VIII polypeptide in its normal role in coagulation, unless otherwise specified. Thus, the term Factor VIII includes variant polypeptides that are functional. Factor VIII proteins can be the human, porcine, canine, and murine factor VIII proteins. As described in the Background Art section, the full length polypeptide and polynucleotide sequences are known, as are many functional fragments, mutants and modified versions. Examples of human factor VIII sequences are shown as subsequences in SEQ ID NOs: 6 or 10 (Table 36). Factor VIII polypeptides include, e.g., full-length factor VIII, full-length factor VIII minus Met at the N-terminus, mature factor VIII (minus the signal sequence), mature factor VIII with an additional Met at the N-terminus, and/or factor VIII with a full or partial deletion of the B domain. Factor VIII variants include B domain deletions, whether partial or full deletions.
[0349] A great many functional factor VIII variants are known, as is discussed above and below. In addition, hundreds of nonfunctional mutations in factor VIII have been identified in hemophilia patients, and it has been determined that the effect of these mutations on factor VIII function is due more to where they lie within the 3-dimensional structure of factor VIII than on the nature of the substitution (Cutler et al., Hum. Mutat. 19:274-8 (2002)), incorporated herein by reference in its entirety. In addition, comparisons between factor VIII from humans and other species have identified conserved residues that are likely to be required for function (Cameron et al., Thromb. Haemost. 79:317-22 (1998); U.S. Pat. No. 6,251,632), incorporated herein by reference in its entirety.
[0350] The human factor VIII gene was isolated and expressed in mammalian cells (Toole, J. J., et al., Nature 312:342-347 (1984); Gitschier, J., et al., Nature 312:326-330 (1984); Wood, W. I., et al., Nature 312:330-337 (1984); Vehar, G. A., et al., Nature 312:337-342 (1984); WO 87/04187; WO 88/08035; WO 88/03558; U.S. Pat. No. 4,757,006), each of which is incorporated herein by reference in its entirety, and the amino acid sequence was deduced from cDNA. Capon et al., U.S. Pat. No. 4,965,199, incorporated herein by reference in its entirety, discloses a recombinant DNA method for producing factor VIII in mammalian host cells and purification of human factor VIII. Human factor VIII expression in CHO (Chinese hamster ovary) cells and BHK (baby hamster kidney cells) has been reported. Human factor VIII has been modified to delete part or all of the B domain (U.S. Pat. Nos. 4,994,371 and 4,868,112, each of which is incorporated herein by reference in its entirety), and replacement of the human factor VIII B domain with the human factor V B domain has been performed (U.S. Pat. No. 5,004,803, incorporated herein by reference in its entirety). The cDNA sequence encoding human factor VIII and predicted amino acid sequence are shown in SEQ ID NOs: 1 and 2, respectively, of US Application Publ. No. 2005/0100990, incorporated herein by reference in its entirety.
[0351] U.S. Pat. No. 5,859,204, Lollar, J. S., incorporated herein by reference in its entirety, reports functional mutants of factor VIII having reduced antigenicity and reduced immunoreactivity. U.S. Pat. No. 6,376,463, Lollar, J. S., incorporated herein by reference in its entirety, also reports mutants of factor VIII having reduced immunoreactivity. US Application Publ. No. 2005/0100990, Saenko et al., incorporated herein by reference in its entirety, reports functional mutations in the A2 domain of factor VIII.
[0352] A number of functional factor VIII molecules, including B-domain deletions, are disclosed in the following patents U.S. Pat. Nos. 6,316,226 and 6,346,513, both assigned to Baxter; U.S. Pat. No. 7,041,635 assigned to In2Gen; U.S. Pat. Nos. 5,789,203, 6,060,447, 5,595,886, and 6,228,620 assigned to Chiron; U.S. Pat. Nos. 5,972,885 and 6,048,720 assigned to Biovitrum, U.S. Pat. Nos. 5,543,502 and 5,610,278 assigned to Novo Nordisk; U.S. Pat. No. 5,171,844 assigned to Immuno Ag; U.S. Pat. No. 5,112,950 assigned to Transgene S. A.; U.S. Pat. No. 4,868,112 assigned to Genetics Institute, each of which is incorporated herein by reference in its entirety.
[0353] The porcine factor VIII sequence is published, (Toole, J. J., et al., Proc. Natl. Acad. Sci. USA 83:5939-5942 (1986)), incorporated herein by reference in its entirety, and the complete porcine cDNA sequence obtained from PCR amplification of factor VIII sequences from a pig spleen cDNA library has been reported (Healey, J. F. et al., Blood 88:4209-4214 (1996), incorporated herein by reference in its entirety). Hybrid human/porcine factor VIII having substitutions of all domains, all subunits, and specific amino acid sequences were disclosed in U.S. Pat. No. 5,364,771 by Lollar and Runge, and in WO 93/20093, incorporated herein by reference in its entirety. More recently, the nucleotide and corresponding amino acid sequences of the A1 and A2 domains of porcine factor VIII and a chimeric factor VIII with porcine A1 and/or A2 domains substituted for the corresponding human domains were reported in WO 94/11503, incorporated herein by reference in its entirety. U.S. Pat. No. 5,859,204, Lollar, J. S., also discloses the porcine cDNA and deduced amino acid sequences. U.S. Pat. No. 6,458,563, incorporated herein by reference in its entirety assigned to Emory discloses a B-domain deleted porcine Factor VIII.
[0354] The Factor VIII (or Factor VIII portion of a chimeric polypeptide) can be at least 60%, 70%, 80%, 90%, 95%, 96%, 97%, 98%, 99%, or 100% identical to a Factor VIII amino acid sequence shown in Table 36 without a signal sequence (amino acids 20 to 1457 of SEQ ID NO: 6; and amino acids 20 to 2351 of SEQ ID NO: 10), wherein the Factor VIII portion has Factor VIII activity. The Factor VIII (or Factor VIII portion of a chimeric polypeptide) can be identical to a Factor VIII amino acid sequence shown in Table 36 without a signal sequence (amino acids 20 to 1457 of SEQ ID NO: 6; and amino acids 20 to 2351 of SEQ ID NO: 10).
[0355] The Factor VIII (or Factor VIII portion of a chimeric polypeptide) can be at least 60%, 70%, 80%, 90%, 95%, 96%, 97%, 98%, 99%, or 100% identical to a Factor VIII amino acid sequence shown in Table 36 with a signal sequence (amino acids 1 to 1457 of SEQ ID NO: 6 and amino acids 1 to 2351 of SEQ ID NO: 10), wherein the Factor VIII portion has Factor VIII activity. The Factor VIII (or Factor VIII portion of a chimeric polypeptide) can be identical to a Factor VIII amino acid sequence shown in Table 36 with a signal sequence (amino acids 1 to 1457 of SEQ ID NO: 6 and amino acids 1 to 2351 of SEQ ID NO: 10).
[0356] As stated above, polypeptide variants include, e.g., modified polypeptides. Modifications include, e.g., acetylation, acylation, ADP-ribosylation, amidation, covalent attachment of flavin, covalent attachment of a heme moiety, covalent attachment of a nucleotide or nucleotide derivative, covalent attachment of a lipid or lipid derivative, covalent attachment of phosphotidylinositol, cross-linking, cyclization, disulfide bond formation, demethylation, formation of covalent cross-links, formation of cysteine, formation of pyroglutamate, formylation, gamma-carboxylation, glycosylation, GPI anchor formation, hydroxylation, iodination, methylation, myristoylation, oxidation, pegylation (Mei et al., Blood 116:270-79 (2010), which is incorporated herein by reference in its entirety), proteolytic processing, phosphorylation, prenylation, racemization, selenoylation, sulfation, transfer-RNA mediated addition of amino acids to proteins such as arginylation, and ubiquitination. In some embodiments, Factor VIII is modified, e.g., pegylated, at any convenient location. In some embodiments, Factor VIII is pegylated at a surface exposed amino acid of Factor VIII, e.g., a surface exposed cysteine, which can be an engineered cysteine. Id.
[0357] The long-acting FVIII polypeptide used herein can comprise processed Factor VIII or single chain Factor VIII or a combination thereof "Processed Factor VIII," as used herein means Factor VIII that has been cleaved at Arginine 1648 (for full-length Factor VIII) or Arginine 754 (for B-domain deleted Factor VIII), i.e., intracellular processing site. Due to the cleavage at the intracellular processing site, processed Factor VIII comprises two polypeptide chains, the first chain being a heavy chain and the second chain being a light chain. For example, the processed Factor VIII-Fc fusion protein (i.e., Heavy chain and Light chain fused to Fc) run at approximately 90 kDa and 130 kDa on a non-reducing SDS-PAGE, respectively, and 90 kDa and 105 kDa on a reducing SDS-PAGE, respectively. Therefore, in one embodiment, at least about 50%, about 60%, about 70%, about 75%, about 80%, about 85%, about 90%, about 95%, about 96%, about 97%, about 98%, about 99%, or about 100% of the Factor VIII portion in the long-acting FVIII polypeptide is processed Factor VIII. In another embodiment, about 50%, about 60%, about 70%, about 75%, about 80%, about 85%, about 90%, about 95%, about 96%, about 97%, about 98%, about 99%, or about 100% of the Factor VIII portion in the long-acting FVIII polypeptide is processed Factor VIII. In a particular embodiment, the long-acting FVIII polypeptide comprising processed Factor VIII is purified (or isolated) from the chimeric polypeptide comprising single chain Factor VIII, and at least about 75%, about 80%, about 85%, about 90%, about 95%, about 96%, about 97%, about 98%, about 99%, or about 100% of the Factor VIII portion in the long-acting FVIII polypeptide is processed Factor VIII. In some embodiments, the long-acting FVIII polypeptide comprises about 15% to 25% of single chain FVIII polypeptide and about 75% to about 85% of processed FVIII polypeptide.
[0358] "Single chain Factor VIII," "SC Factor VIII," or "SCFVIII" as used herein means Factor VIII that has not been cleaved at the Arginine site (residue 1648 for full-length Factor VIII (i.e., residue 1667 of SEQ ID NO: 10) or residue 754 for B-domain deleted Factor VIII (i.e., residue 773 of SEQ ID NO: 6). Therefore, single chain Factor VIII in the long-acting FVIII polypeptide used herein comprises a single chain. In one embodiment, the single chain Factor VIII contains an intact intracellular processing site. In another embodiment, the single chain Factor VIII of the invention comprises a substitution or mutation at an amino acid position corresponding to Arginine 1645, a substitution or mutation at an amino acid position corresponding to Arginine 1648, or a substitution or mutation at amino acid positions corresponding to Arginine 1645 and Arginine 1648 in full-length Factor VIII. In other embodiments, the amino acid substituted at the amino acid position corresponding to Arginine 1645 is a different amino acid from the amino acid substituted at the amino acid position corresponding to Arginine 1648. In certain embodiments, the substitution or mutation is an amino acid other than arginine, e.g., isoleucine, leucine, lysine, methionine, phenylalanine, threonine, tryptophan, valine, alanine, asparagine, aspartic acid, cysteine, glutamic acid, glutamine, glycine, proline, selenocysteine, serine, tyrosine, histidine, ornithine, pyrrolysine, or taurine. The single chain Factor VIII-Fc fusion protein can run at approximately 220 kDa on a non-reducing SDS-PAGE and at approximately 195 kDa on a reducing SDS-PAGE.
[0359] The Factor VIII portion in the long-acting FVIII polypeptide used herein has Factor VIII activity. Factor VIII activity can be measured by any known methods in the art. For example, one of those methods can be a chromogenic assay. The chromogenic assay mechanism is based on the principles of the blood coagulation cascade, where activated Factor VIII accelerates the conversion of Factor X into Factor Xa in the presence of activated Factor IX, phospholipids and calcium ions. The Factor Xa activity is assessed by hydrolysis of a p-nitroanilide (pNA) substrate specific to Factor Xa. The initial rate of release of p-nitroaniline measured at 405 nM is directly proportional to the Factor Xa activity and thus to the Factor VIII activity in the sample. The chromogenic assay is recommended by the Factor VIII and Factor IX Subcommittee of the Scientific and Standardization Committee (SSC) of the International Society on Thrombosis and Hemostasis (ISTH). Since 1994, the chromogenic assay has also been the reference method of the European Pharmacopoeia for the assignment of FVIII concentrate potency. Thus, in one embodiment, the long-acting FVIII polypeptide comprising single chain Factor VIII has Factor VIII activity comparable to a long-acting FVIII polypeptide comprising processed Factor VIII (e.g., a chimeric polypeptide consisting essentially of or consisting of two Fc portions and processed Factor VIII, wherein said processed Factor VIII is fused to one of the two Fc portions), when the Factor VIII activity is measured in vitro by a chromogenic assay.
[0360] Second Portion
[0361] In some embodiments, the long-acting FIX or FVIII polypeptide comprises a FIX or FVIII portion and a non-FIX portion or a non-Factor VIII portion, respectively, e.g., a heterologous moiety. In one embodiment, the heterologous moiety is capable of extending in vivo or in vitro half-life of the FIX or FVIII polypeptide. Exemplary non-FIX or FVIII portions include, e.g., Fc, albumin, a PAS sequence, transferrin, CTP (28 amino acid C-terminal peptide (CTP) of human chorionic gonadotropin (hCG) with its 4 O-glycans), polyethylene glycol (PEG), hydroxyethyl starch (HES), albumin binding polypeptide, albumin-binding small molecules, or any combination thereof. Exemplary long-acting FVIII polypeptides of the invention include, e.g., Factor VIII-Fc polypeptides, Factor VIII-albumin polypeptides, Factor VIII-PAS polypeptides, Factor VIII-transferrin polypeptides, Factor VIII-CTP polypeptides, Factor VIII-PEG polypeptides, Factor VIII-HES polypeptides, Factor VIII-albumin binding polypeptide polypeptides, or Factor VIII-albumin-binding small molecule polypeptides. Exemplary long-acting FIX polypeptides of the invention include, e.g., Factor IX-Fc polypeptides, Factor IX-albumin polypeptides, Factor IX-PAS polypeptides, Factor IX-transferrin polypeptides, Factor IX-CTP polypeptides, Factor IX-PEG polypeptides, Factor IX-HES polypeptides, Factor IX-albumin binding polypeptide polypeptides, or Factor IX-albumin-binding small molecule polypeptides.
[0362] In one embodiment, the second portion fused to FIX or FVIII is an FcRn binding partner. In another embodiment, an FcRn binding partner fused to FIX or FVIII is an Fc fragment. An FcRn binding partner is any molecule that can be specifically bound by the FcRn receptor with consequent active transport by the FcRn receptor of the FcRn binding partner. Thus, the term Fc includes any variants of IgG Fc that are functional. The region of the Fc portion of IgG that binds to the FcRn receptor has been described based on X-ray crystallography (Burmeister et al., Nature 372:379 (1994), incorporated herein by reference in its entirety). The major contact area of the Fc with the FcRn is near the junction of the CH2 and CH3 domains. Fc-FcRn contacts are all within a single Ig heavy chain. The FcRn binding partners include, e.g., whole IgG, the Fc fragment of IgG, and other fragments of IgG that include the complete binding region of FcRn. The major contact sites include amino acid residues 248, 250-257, 272, 285, 288, 290-291, 308-311, and 314 of the CH2 domain and amino acid residues 385-387, 428, and 433-436 of the CH3 domain. References made to amino acid numbering of immunoglobulins or immunoglobulin fragments, or regions, are all based on Kabat et al. 1991, Sequences of Proteins of Immunological Interest, U. S. Department of Public Health, Bethesda; MD, incorporated herein by reference in its entirety. (The FcRn receptor has been isolated from several mammalian species including humans. The sequences of the human FcRn, rat FcRn, and mouse FcRn are known (Story et al., J. Exp. Med. 180: 2377 (1994), incorporated herein by reference in its entirety.) An Fc can comprise the CH2 and CH3 domains of an immunoglobulin with or without the hinge region of the immunoglobulin. Exemplary Fc variants are provided in WO 2004/101740 and WO 2006/074199, incorporated herein by reference in its entirety.
[0363] Fc (or Fc portion of a chimeric polypeptide) can contain one or more mutations, and combinations of mutations.
[0364] Fc (or Fc portion of a chimeric polypeptide) can contain mutations conferring increased half-life such as M252Y, S254T, T256E, and combinations thereof, as disclosed in Oganesyan et al., Mol. Immunol. 46:1750 (2009), which is incorporated herein by reference in its entirety; H433K, N434F, and combinations thereof, as disclosed in Vaccaro et al., Nat. Biotechnol. 23:1283 (2005), which is incorporated herein by reference in its entirety; the mutants disclosed at pages 1-2, paragraph [0012], and Examples 9 and 10 of US 2009/0264627 A1, which is incorporated herein by reference in its entirety; and the mutants disclosed at page 2, paragraphs [0014] to [0021] of US 20090163699 A1, which is incorporated herein by reference in its entirety.
[0365] Fc (or Fc portion of a chimeric polypeptide) can also include, e.g., the following mutations: The Fc region of IgG can be modified according to well recognized procedures such as site directed mutagenesis and the like to yield modified IgG or Fc fragments or portions thereof that will be bound by FcRn. Such modifications include, e.g., modifications remote from the FcRn contact sites as well as modifications within the contact sites that preserve or even enhance binding to the FcRn. For example the following single amino acid residues in human IgG1 Fc (Fcy1) can be substituted without significant loss of Fc binding affinity for FcRn: P238A, S239A, K246A, K248A, D249A, M252A, T256A, E258A, T260A, D265A, S267A, H268A, E269A, D270A, E272A, L274A, N276A, Y278A, D280A, V282A, E283A, H285A, N286A, T289A, K290A, R292A, E293A, E294A, Q295A, Y296F, N297A, S298A, Y300F, R301A, V303A, V305A, T307A, L309A, Q311A, D312A, N315A, K317A, E318A, K320A, K322A, S324A, K326A, A327Q, P329A, A330Q, A330S, P331A, P331S, E333A, K334A, T335A, S337A, K338A, K340A, Q342A, R344A, E345A, Q347A, R355A, E356A, M358A, T359A, K360A, N361A, Q362A, Y373A, S375A D376A, A378Q, E380A, E382A, S383A, N384A, Q386A, E388A, N389A, N390A, Y391F, K392A, L398A, S400A, D401A, D413A, K414A, R416A, Q418A, Q419A, N421A, V422A, S424A, E430A, N434A, T437A, Q438A, K439A, S440A, S444A, and K447A, where for example P238A represents wildtype proline substituted by alanine at position number 238. In addition to alanine other amino acids can be substituted for the wildtype amino acids at the positions specified above. Mutations can be introduced singly into Fc giving rise to more than one hundred FcRn binding partners distinct from native Fc. Additionally, combinations of two, three, or more of these individual mutations can be introduced together, giving rise to hundreds more FcRn binding partners. Certain of these mutations can confer new functionality upon the FcRn binding partner. For example, one embodiment incorporates N297A, removing a highly conserved N-glycosylation site. The effect of this mutation is to reduce immunogenicity, thereby enhancing circulating half-life of the FcRn binding partner, and to render the FcRn binding partner incapable of binding to FcyRI, FcyRIIA, FcyRIIB, and FcyRIIIA, without compromising affinity for FcRn (Routledge et al. 1995, Transplantation 60:847, which is incorporated herein by reference in its entirety; Friend et al. 1999, Transplantation 68:1632, which is incorporated herein by reference in its entirety; Shields et al. 1995, J. Biol. Chem. 276:6591, which is incorporated herein by reference in its entirety). Additionally, at least three human Fc gamma receptors appear to recognize a binding site on IgG within the lower hinge region, generally amino acids 234-237. Therefore, another example of new functionality and potential decreased immunogenicity can arise from mutations of this region, as for example by replacing amino acids 233-236 of human IgG1 "ELLG" to the corresponding sequence from IgG2 "PVA" (with one amino acid deletion). It has been shown that FcyRI, FcyRII, and FcyRIII which mediate various effector functions will not bind to IgG1 when such mutations have been introduced (Ward and Ghetie, Therapeutic Immunology 2:77 (1995), which is incorporated herein by reference in its entirety; and Armour et al., Eur. J. Immunol. 29:2613 (1999), which is incorporated herein by reference in its entirety). As a further example of new functionality arising from mutations described above affinity for FcRn can be increased beyond that of wild type in some instances. This increased affinity can reflect an increased "on" rate, a decreased "off" rate or both an increased "on" rate and a decreased "off" rate. Mutations believed to impart an increased affinity for FcRn include, e.g., T256A, T307A, E380A, and N434A (Shields et al., J. Biol. Chem. 276:6591 (2001), which is incorporated herein by reference in its entirety).
[0366] The Fc (or Fc portion of a chimeric polypeptide) can be at least 60%, 70%, 80%, 90%, 95%, 96%, 97%, 98%, 99%, or 100% identical to the Fc amino acid sequence shown in Table 36 (amino acids 1458 to 1684 of SEQ ID NO: 6 or amino acids 2352 to 2578 of SEQ ID NO: 10). The Fc (or Fc portion of a chimeric polypeptide) can be identical to the Fc amino acid sequence shown in Table 36 (amino acids 1458 to 1684 of SEQ ID NO: 6 and amino acids 2352 to 2578 of SEQ ID NO: 10).
[0367] As discussed above, exemplary long-acting polypeptides also include FIX or FVIII fused to one or more albumin polypeptides, albumin binding polypeptides, or albumin-binding small molecules. In one embodiment, the albumin is human albumin. The albumin or albumin binding protein can be fused to either the N-terminal end of FIX or FVIII or to the C-terminal end of FIX or FVIII or inserted between two amino acids in FIX or FVIII. Examples of albumin, e.g., fragments thereof, that can be used in the present invention are known. e.g., U.S. Pat. Nos. 7,592,010; 6,686,179; and Schulte, Thrombosis Res. 124 Suppl. 2:S6-S8 (2009), each of which is incorporated herein by reference in its entirety.
[0368] The albumin binding polypeptides can compromise, without limitation, bacterial albumin-binding domains, albumin-binding peptides, or albumin-binding antibody fragments that can bind to albumin. Domain 3 from streptococcal protein G, as disclosed by Kraulis et al., FEBS Lett. 378:190-194 (1996) and Linhult et al., Protein Sci. 11:206-213 (2002) is an example of a bacterial albumin-binding domain. Examples of albumin-binding peptides include a series of peptides having the core sequence DICLPRWGCLW (SEQ ID NO: 12). See, e.g., Dennis et al., J. Biol. Chem. 2002, 277: 35035-35043 (2002). Examples of albumin-binding antibody fragments are disclosed in Muller and Kontermann, Curr. Opin. Mol. Ther. 9:319-326 (2007); Rooverset et al., Cancer Immunol. Immunother. 56:303-317 (2007), and Holt et al., Prot. Eng. Design Sci., 21:283-288 (2008), which are incorporated herein by reference in their entireties.
[0369] In certain aspects, a recombinant FIX or FVIII polypeptide of the invention comprises at least one attachment site for a non-polypeptide small molecule, variant, or derivative that can bind to albumin thereof. An example of such albumin binding moieties is 2-(3-maleimidopropanamido)-6-(4-(4-iodophenyl)butanamido)hexanoate ("Albu" tag) as disclosed by Trusselet et al., Bioconjugate Chem. 20:2286-2292 (2009).
[0370] As discussed above, exemplary long-acting polypeptides also include FIX or FVIII fused to at least one C-terminal peptide (CTP) of the .beta. subunit of human chorionic gonadotropin or fragment, variant, or derivative thereof. The CTP can be fused to FIX or FVIII either the N-terminal end of FIX or FVIII or to the C-terminal end of FIX or FVIII or inserted between two amino acids in FIX or FVIII. One or more CTP peptides fused to or inserted into a recombinant protein is known to increase the in vivo half-life of that protein. See, e.g., U.S. Pat. No. 5,712,122, incorporated by reference herein in its entirety. Exemplary CTP peptides include DPRFQDSSSSKAPPPSLPSPSRLPGPSDTPIL (SEQ ID NO: 13) or SSSSKAPPPSLPSPSRLPGPSDTPILPQ. (SEQ ID NO: 14). See, e.g., U.S. Patent Application Publication No. US 2009/0087411 A1, incorporated by reference.
[0371] As discussed above, exemplary long-acting polypeptides also include FIX or FVIII fused to at least one PAS sequence or fragment, variant, or derivative thereof. The PAS sequence can be fused to either the N-terminal end of FIX or FVIII or to the C-terminal end of FIX or FVIII or inserted between two amino acids in FVIII. A PAS peptide or PAS sequence, as used herein, means an amino acid sequence comprising mainly alanine and serine residues or comprising mainly alanine, serine, and proline residues, the amino acid sequence forming random coil conformation under physiological conditions. Accordingly, the PAS sequence is a building block, an amino acid polymer, or a sequence cassette comprising, consisting essentially of, or consisting of alanine, serine, and proline which can be used as a part of the heterologous moiety in the chimeric protein. An amino acid polymer also can form random coil conformation when residues other than alanine, serine, and proline are added as a minor constituent in the PAS sequence. By "minor constituent" is meant that that amino acids other than alanine, serine, and proline can be added in the PAS sequence to a certain degree, e.g., up to about 12%, i.e., about 12 of 100 amino acids of the PAS sequence, up to about 10%, up to about 9%, up to about 8%, about 6%, about 5%, about 4%, about 3%, i.e. about 2%, or about 1%, of the amino acids. The amino acids different from alanine, serine and proline can be selected from the group consisting of Arg, Asn, Asp, Cys, Gln, Glu, Gly, His, Ile, Leu, Lys, Met, Phe, Thr, Trp, Tyr, and Val. Under physiological conditions, a PAS peptide forms a random coil conformation and thereby can mediate an increased in vivo and/or in vitro stability to a recombinant protein of the invention, and has procoagulant activity.
[0372] Non-limiting examples of the PAS peptides include ASPAAPAPASPAAPAPSAPA (SEQ ID NO: 15), AAPASPAPAAPSAPAPAAPS (SEQ ID NO: 16), APSSPSPSAPSSPSPASPSS (SEQ ID NO: 17), APSSPSPSAPSSPSPASPS (SEQ ID NO: 18), SSPSAPSPSSPASPSPSSPA (SEQ ID NO: 19), AASPAAPSAPPAAASPAAPSAPPA (SEQ ID NO: 20), ASAAAPAAASAAASAPSAAA (SEQ ID NO: 21) or any variants, derivatives, fragments, or combinations thereof. Additional examples of PAS sequences are known from, e.g., US Pat. Publ. No. 2010/0292130 A1 and PCT Appl. Publ. No. WO 2008/155134 A1. European issued patent EP2173890.
[0373] As discussed above, exemplary long-acting polypeptides also include FIX or FVIII fused to at least one transferrin peptide or fragment, variant, or derivative thereof. At least one transferrin peptide can be fused to either the N-terminal end of FIX or FVIII or to the C-terminal end of FIX or FVIII or inserted between two amino acids in FIX or FVIII. Any transferrin can be fused to or inserted into a recombinant FIX or FVIII protein of the invention. As an example, wild-type human Tf (Tf) is a 679 amino acid protein, of approximately 75 KDa (not accounting for glycosylation), with two main domains, N (about 330 amino acids) and C (about 340 amino acids), which appear to originate from a gene duplication. See GenBank accession numbers NM001063, XM002793, M12530, XM039845, XM 039847 and S95936 (www.ncbi.nlm.nih.gov), all of which are herein incorporated by reference in their entirety.
[0374] Transferrin transports iron through transferrin receptor (TfR)-mediated endocytosis. After the iron is released into an endosomal compartment and Tf-TfR complex is recycled to cell surface, the Tf is released back extracellular space for next cycle of iron transporting. Tf possesses a long half-life that is in excess of 14-17 days (Li et al., Trends Pharmacol. Sci. 23:206-209 (2002)). Transferrin fusion proteins have been studied for half-life extension, targeted deliver for cancer therapies, oral delivery and sustained activation of proinsulin (Brandsma et al., Biotechnol. Adv., 29: 230-238 (2011); Bai et al., Proc. Natl. Acad. Sci. USA 102:7292-7296 (2005); Kim et al., J. Pharmacol. Exp. Ther., 334:682-692 (2010); Wang et al., J. Controlled Release 155:386-392 (2011)).
[0375] As discussed above, exemplary long-acting polypeptides also include FIX or FVIII fused to at least one polyethylene glycol (PEG) moieties.
[0376] PEGylated FVIII can refer to a conjugate formed between FIX or FVIII and at least one polyethylene glycol (PEG) molecule. PEG is commercially available in a large variety of molecular weights and average molecular weight ranges. Typical examples of PEG average molecular weight ranges include, but are not limited to, about 200, about 300, about 400, about 600, about 1000, about 1300-1600, about 1450, about 2000, about 3000, about 3000-3750, about 3350, about 3000-7000, about 3500-4500, about 5000-7000, about 7000-9000, about 8000, about 10000, about 8500-11500, about 16000-24000, about 35000, about 40000, about 60000, and about 80000 daltons. These average molecular weights are provided merely as examples and are not meant to be limiting in any way.
[0377] A recombinant long-acting FIX or FVIII protein of the invention can be PEGylated to include mono- or poly (e.g., 2-4) PEG moieties. PEGylation can be carried out by any of the PEGylation reactions known in the art. Methods for preparing a PEGylated protein product will generally include (i) reacting a polypeptide with polyethylene glycol (such as a reactive ester or aldehyde derivative of PEG) under conditions whereby the peptide of the invention becomes attached to one or more PEG groups; and (ii) obtaining the reaction product(s). In general, the optimal reaction conditions for the reactions will be determined case by case based on known parameters and the desired result.
[0378] There are a number of PEG attachment methods available to those skilled in the art, for example Malik F et al., Exp. Hematol. 20:1028-35 (1992); Francis, Focus on Growth Factors 3(2):4-10 (1992); European Pat. Pub. Nos. EP0401384, EP0154316, and EP0401384; and International Pat. Appl. Pub. Nos. WO92/16221 and WO95/34326. As a non-limiting example, FIX or FVIII variants can contain cysteine substitutions in one or more insertion sites in FIX or FVIII, and the cysteines can be further conjugated to PEG polymer. See Mei et al., Blood 116:270-279 (2010) and U.S. Pat. No. 7,632,921, which are incorporated herein by reference in their entireties.
[0379] As discussed above, exemplary long-acting polypeptides also include FIX or FVIII fused to at least one hydroxyethyl starch (HES) polymer. HES is a derivative of naturally occurring amylopectin and is degraded by alpha-amylase in the body. HES exhibits advantageous biological properties and is used as a blood volume replacement agent and in hemodilution therapy in the clinics. See, e.g., Sommermeyer et al., Krankenhauspharmazie 8:271-278 (1987); and Weidler et al., Arzneim.-Forschung/Drug Res. 41: 494-498 (1991).
[0380] HES is mainly characterized by the molecular weight distribution and the degree of substitution. HES has a mean molecular weight (weight mean) of from 1 to 300 kD, from 2 to 200 kD, from 3 to 100 kD, or from 4 to 70 kD. Hydroxyethyl starch can further exhibit a molar degree of substitution of from 0.1 to 3, from 0.1 to 2, from 0.1 to 0.9, or from 0.1 to 0.8, and a ratio between C2:C6 substitution in the range of from 2 to 20 with respect to the hydroxyethyl groups. HES with a mean molecular weight of about 130 kD is VOLUVEN.RTM. from Fresenius. VOLUVEN.RTM. is an artificial colloid, employed, e.g., for volume replacement used in the therapeutic indication for therapy and prophylaxis of hypovolaemia. There are a number of HES attachment methods available to those skilled in the art, e.g., the same PEG attachment methods described above.
[0381] Pharmaceutical Composition
[0382] A long-acting FIX polypeptide or a long-acting FVIII polypeptide can be formulated as a pharmaceutical composition. The pharmaceutical composition can be formulated for administration to humans. The pharmaceutical compositions used in the methods of this invention comprise pharmaceutically acceptable carriers, including, e.g., ion exchangers, alumina, aluminum stearate, lecithin, serum proteins, such as human serum albumin, buffer substances such as phosphates, glycine, sorbic acid, potassium sorbate, partial glyceride mixtures of saturated vegetable fatty acids, water, salts or electrolytes, such as protamine sulfate, disodium hydrogen phosphate, potassium hydrogen phosphate, sodium chloride, zinc salts, colloidal silica, magnesium trisilicate, polyvinyl pyrrolidone, cellulose-based substances, polyethylene glycol, sodium carboxymethylcellulose, polyacrylates, waxes, polyethylene-polyoxypropylene-block polymers, polyethylene glycol and wool fat. Various methods of formulating the invention is well known in the art.
[0383] A long-acting FIX polypeptide or a long-acting FVIII polypeptide can be formulated as a pharmaceutical composition or formulation. In certain formulations provided herein, a long-acting FIX polypeptide or a long-acting FVIII polypeptide is formulated as a sterile, preservative-free, non-pyrogenic, lyophilized, white to off-white powder to cake, for intravenous (IV) administration. The formulation can be provided in a single-use vial.
[0384] In certain embodiments the first container of a pharmaceutical kit provided herein is a glass vial comprising a rubber stopper. In certain embodiments, the second container a pharmaceutical kit provided herein is a syringe body, associated with a plunger. In certain embodiments, the syringe is a pre-filled syringe containing the diluent. In certain embodiments, a pharmaceutical kit provided herein further comprises an adaptor to connect the glass vial to the syringe body. In certain embodiments a pharmaceutical kit provided herein further comprises infusion tubing associated with a needle to be connected to the syringe, suitable for intravenous infusion.
[0385] In certain embodiments, a desired dose of a long-acting FIX polypeptide or a long-acting FVIII polypeptide can be achieved through the use of one pharmaceutical kit as provided herein. In certain embodiments, more than one pharmaceutical kit can be used to achieve a desired dose. Provided herein is a method of combining or pooling the formulations contained in two or more pharmaceutical kits as provided herein in order to achieve a desired dose.
[0386] The pharmaceutical composition of the invention can be formulated as a liquid formulation, lyophilized powder, or suspension. A container comprising the pharmaceutical compositions can be a vial, a cartridge, or a syringe. In a particular embodiment, a syringe comprising the pharmaceutical composition is a dual chamber syringe.
[0387] In certain embodiments, the pharmaceutical composition of the invention or the reconstitution solution for the lyophilized powder comprises a preservative in an amount sufficient to provide antimicrobial activity. Pharmaceutically acceptable preservatives that are useful for pharmaceutical composition are well known in the art. For example, examples of the pharmaceutically acceptable preservatives include, but are not limited to, phenol, m-cresol, benzyl alcohol, chlorobutanol, methyl paraben, propylparaben, phenoxyethanol, any other pharmaceutically acceptable preservative, and any combinations thereof. In a particular embodiment, the preservative is benzyl alcohol. In some embodiments, the pharmaceutical composition comprises benzyl alcohol at a concentration between 0.5% and 0.9%.
[0388] Having now described the present invention in detail, the same will be more clearly understood by reference to the following examples, which are included herewith for purposes of illustration only and are not intended to be limiting of the invention. All patents and publications referred to herein are expressly incorporated by reference.
EXAMPLES
Example 1. Product Description
[0389] rFIXFc is a long-acting, fully recombinant fusion protein consisting of human coagulation Factor IX (FIX) covalently linked to the Fc domain of human immunoglobulin G1 (IgG1). The Factor IX portion of rFIXFc has a primary amino acid sequence that is identical to the Thr.sup.148 allelic form of plasma derived Factor IX and has structural and functional characteristics similar to endogenous Factor IX. The Fc domain of rFIXFc contains the hinge, CH2 and CH3 regions of IgG1. rFIXFc contains 869 amino acids with a molecular weight of approximately 98 kilodaltons.
[0390] rFIXFc is produced by recombinant DNA technology in a human embryonic kidney (HEK) cell line, which has been extensively characterized. The cell line expresses rFIXFc into a defined cell culture medium that does not contain any proteins derived from animal or human sources. rFIXFc is purified by a series of chromatography steps that does not require use of a monoclonal antibody. The process includes multiple viral clearance steps including 15 nm virus-retaining nano-filtration. No human or animal additives are used in the cell culture, purification, and formulation processes.
Example 2: Dosage and Method of Administration/Method of Calculating Initial Estimated Dose
[0391] rFIXFc is long-acting anti-hemophilic factor (recombinant) indicated in adults and children (.gtoreq.12 years) with hemophilia B (congenital Factor IX deficiency) for, e.g., control and prevention of bleeding episodes, routine prophylaxis to prevent or reduce the frequency of bleeding episodes, and perioperative management (surgical prophylaxis).
[0392] Dosing of rFIXFc, formulated as described in Example 1, can be estimated as described in this example, but can also be determined by standard tests such as FIX activity assays described elsewhere herein.
[0393] 1 IU of rFIXFc per kg body weight is expected to increase the circulating level of Factor IX by 1% [IU/dL]. rFIXFc has been shown to have a prolonged circulating half-life.
[0394] No dose adjustment for recovery is generally required. Since subjects can vary in their pharmacokinetic (e.g., half-life, in vivo recovery) and clinical responses to rFIXFc, the expected in vivo peak increase in Factor IX level expressed as IU/dL (or % of normal) or the required dose can be estimated using the following formulas:
IU/dL (or % of normal)=[Total Dose (IU)/body weight (kg)].times.recovery (IU/dL per IU/kg) (D)
OR
Dose (IU)=body weight (kg).times.Desired Factor IX Rise (IU/dL or % of normal).times.reciprocal of recovery (IU/kg per IU/dL) (E)
[0395] The following table (Table 1) can be used to guide dosing in bleeding episodes:
TABLE-US-00001 TABLE 1 Guide to rFIXFc Dosing for Treatment of Bleeding Factor IX Level Required Dose (IU/dL or % (IU/kg)/Frequency Severity of Bleed of normal) of Doses (hrs) Minor and Moderate 30-60 30-60 IU/kg For example: joint, Repeat every 48 hours if superficial muscle/no there is further evidence of neurovascular compromise bleeding (except iliopsoas), superficial soft tissue, mucous membranes Major 80-120 For repeat dosing, follow For example: iliopsoas and guidelines for major deep muscle with surgery [see Table 2] neurovascular injury, or substantial blood loss, retroperitoneum, CNS Adapted from: Roberts and Eberst, WFH 2008, and WFH 2012
[0396] Subsequent dosage and duration of treatment depends on the individual clinical response, the severity of the Factor IX deficiency, and the location and extent of bleeding.
[0397] The following table (Table 2) can be used to guide dosing for and perioperative management (surgical prophylaxis):
TABLE-US-00002 TABLE 2 Guide to rFIXFc Dosing for Perioperative Management (Surgical Prophylaxis)* Initial Factor IX Level Required Dose (IU/dL or % (IU/kg)/Frequency Type of Surgery of normal) of Doses (hrs) Minor 50 to 80 50-80 IU/kg Minor operations A single infusion may be including sufficient. Repeat as needed uncomplicated after 24-48 hours. dental extraction Major 60 to 120 100 IU/kg (initial dose) (initial level) A repeat dose at 80 IU/kg Days 1-3: should be considered after 6-10 maintain level hours and then every 24 hours 40-60% for the first 3 days. Days 4-6: Based on the long half-life of maintain level rFIXFc, the dose may be 30-50% reduced and frequency of Days 7-14: dosing in the post-surgical maintain level setting may be extended after 20-40% day 3 to every 48 hours. Adapted from: Roberts and Eberst, WFH 2008, and WFH 2012 *See Pharmacokinetics (Example 5 below)
[0398] For routine prophylaxis, the recommended starting regimens are either: 50 IU/kg once weekly, or 100 IU/kg once every 10-14 days. Either regimen can be adjusted based on subject response.
[0399] rFIXFc is contraindicated in subjects who have manifested severe hypersensitivity reactions, including anaphylaxis, to the product or its components.
[0400] The clinical response to rFIXFc may vary. If bleeding is not controlled with the recommended dose, the plasma level of Factor IX can be determined, and a sufficient dose of rFIXFc can be administered to achieve a satisfactory clinical response. If the subject's plasma Factor IX level fails to increase as expected or if bleeding is not controlled after rFIXFc administration, the subject's plasma can be tested for the presence of an inhibitor, e.g., neutralizing antibodies. Subjects using rFIXFc can be monitored for the development of Factor IX inhibitors by appropriate clinical observations and laboratory tests known to those of ordinary skill in the art.
[0401] Subject's plasma can be monitored for Factor IX activity levels by performing, e.g., the one-stage clotting assay to confirm adequate Factor IX levels have been achieved and maintained, when clinically indicated. Subject's plasma can further be monitored for the development of Factor IX inhibitors.
Example 3. The Clinical Implications of Population Pharmacokinetics of rFIXFc in Routine Prophylaxis, Control of Bleeding and Perioperative Management for Hemophilia B Subjects
[0402] BACKGROUND: Clinical dosing of factor IX (FIX) in treatment of hemophilia B is well established based on empirical practice and clinical outcomes. Since pharmacokinetics (PK) of FIX activity is the surrogate efficacy marker, we utilized population PK (popPK) modeling and simulation to evaluate dosing regimens of long-acting recombinant FIX Fc fusion protein (rFIXFc). The PK of rFIXFc, from 135 single-dose and 21 repeat-dose profiles in subjects .gtoreq.12 years old (body weight (BW): 45-186.7 kg), was best described by a 3-compartmental model, which showed modest inter-individual variability (IIV) of 17.7% for clearance (CL) and 21.7% for volume of central compartment (V1). The proportional residue error of 10.6% approximates the variability of the one-stage clotting assay for FIX activity. The only covariate that showed a weak association with rFIXFc PK is BW, which accounted for .about.3% of IIV for CL and V1, suggesting that BW-independent flat dosing of rFIXFc may be feasible for treating adult hemophilia B subjects.
[0403] AIMS: To simulate the BW-based and flat dosing regimens for routine prophylaxis, control of bleeding and perioperative management in the hemophilia B population.
[0404] METHOD: The validated 3-compartmental popPK model, including inter-occasion variability and BW as the covariate on CL and V1, was used for dosing simulations. For BW-based dosing regimen, PK profiles were simulated for 1000 subjects with BW distribution representative of the phase 3 study. BW distribution was simulated using a power function Z=BW-0.5. The generated BW (1000 values) distribution has a median of 74.9 kg and a range of 38.9 to 172.6 kg, which is similar to our studies (median, 73.3 kg; min and max, 45 and 186.7 kg). For fixed dosing regimen, three populations (n=1000 each) were stratified based on low (.ltoreq.10th percentile), typical (10th-90th percentile) and high (.gtoreq.90th percentile) BW. Variability of exposure parameters, percentage of population maintaining target Cmax and trough, and deviations of median exposure parameters in extreme BW groups were compared with BW-based and flat dosing regimens. To simulate steady-state in prophylaxis regimen, six doses were applied for all dosing regimens (once weekly, every 10 days, or every 14 days), with each dosing interval assigned as one occasion. To simulate the PK profile following an episodic treatment, a single dose was applied.
[0405] RESULT: Consistent with the observations from the phase 3 study, popPK simulation of 50 IU/kg once weekly or 100 IU/kg every 10-14 days predicted peak FIX activity within the physiologic range (Cmax <150%) and trough .gtoreq.1% in majority of the population. All simulated regimens predicted that the majority of the population will maintain trough activity at or above 1% (Table 3).
TABLE-US-00003 TABLE 3 Predicted percentage of population with steady-state trough at or above 1% for various prophylaxis dosing regimens % of population Regimen Total weekly dose with trough .gtoreq.1% 50 IU/kg weekly 50 95.4 100 IU/kg weekly 100 99.6 100 IU/kg every 10 days 70 89.2 100 IU/kg every 14 days 50 52.8
[0406] A plot showing a population simulation of steady-state FIX activity vs. time is shown in FIG. 11. Table 4 shows the predicted steady state FIX activity over the course of 14 days for two dosing regimens: 50 IU/kg weekly and 100 IU/kg every 14 days.
TABLE-US-00004 TABLE 4 Predicted steady state FIX activity EOI Day 1 Day 3 Day 5 Day 7 Day 10 Day 14 median median median median median median median [5th, [5th, [5th, [5th, [5th, [5th, [5th, Dose, IU/kg 95th] 95th] 95th] 95th] 95th] 95th] 95th] 50 IU/kg weekly 52.6 16.9 7.17 4.16 2.67 NA NA [32.1, [11.2, [3.85, [1.93, [1.02, 89.3] 26.1] 12.3] 7.83] 5.49] 100 102 30.0 12.0 6.78 4.28 2.29 1.07 100 IU/kg [60.0, [19.6, [6.62, [3.24, [1.82, [0.688, [0.0758, every 14 days 166] 46.7] 19.9] 12.2] 8.06] 5.33] 3.23]
[0407] Furthermore, BW-based and flat dosing resulted in comparable PK profiles with comparable exposure parameters, e.g., 50 IU/kg and 4000 IU once weekly predicted a median (5th, 95th percentile) Cmax of 52.6 (32.1, 89.3) IU/dL and 56.1 (36.2, 90.9) IU/dL, respectively. Both dosing regimens predicted that >95% of the population maintains Cmax <150% and trough .gtoreq.1% (FIG. 12). However, BW-based and flat dosing showed differential effects on the exposure parameters in extreme (.ltoreq.10th or .gtoreq.90th percentile) BW populations. This suggests that BW-independent flat dosing may be feasible for patients 12 years and older.
[0408] The popPK model was used to simulate dosing regimens for episodic treatment. The model predicts that for the control of bleeding episodes, a single dose of 50 or 100 IU/kg of rFIXFc is sufficient to maintain the plasma FIX peak activity levels at 40 to 80 IU/dL (Table 5) as recommended by the World Federation of Hemophilia (WFH) guidelines.
TABLE-US-00005 TABLE 5 Predicted FIX activity profile after a single dose of rFIXFc in the 5th to 95th percentile of the population rFIXFc dose, median [5th, 95th] 50 IU/kg 100 IU/kg End of infusion 50.8 [30.4, 84.5] 102 [60.8, 169] 12 hours 21.1 [13.5, 33.6] 42.3 [26.8, 67.3] 24 hours (day 1) 14.8 [9.78, 22.7] 29.5 [19.6, 45.5] 36 hours 10.9 [6.79, 17.1] 21.8 [13.7, 34.1] 48 hours (day 2) 8.51 [5.14, 13.2] 17.0 [10.5, 26.6] 72 hours (day 3) 5.57 [3.05, 9.27] 11.1 [6.22, 18.5] Day 5 3.07 [1.44, 5.62] 6.14 [3.05, 11.0] Day 7 1.93 [0.795, 3.71] 3.88 [1.82, 7.28] Day 10 1.1 [0.277, 2.33] 2.19 [0.775, 4.56] Day 14 0.559 [0, 1.38] 1.08 [0.125, 2.58]
[0409] Analysis of 12 major surgeries and 2 minor surgeries found that the FIX activities measured during the perioperative period were largely consistent with the prediction by popPK based on subjects' pre-surgery baseline PK, indicating no substantial factor consumption in these surgeries. A representative plot of observed and predicted perioperative FIX activity is shown in FIG. 10. Simulated and observed FIX activities were compared within the first 21 days after the first rFIXFc surgical dose (n=14; 12 major surgeries, 2 minor surgeries). There was good correlation between the observed FIX activity data and that predicted by the PK model (relative prediction error [95% CI], 0.332% [-2.08%, 1.42%]).
[0410] CONCLUSION: PopPK provides a robust and effective means to evaluate potential dosing regimens. The predictions by popPK simulation for rFIXFc corroborate the results from the phase 3 study. The simulations of BW-based and flat dosing of rFIXFc achieved similar PK profiles. Considering the wide therapeutic range for factor replacement therapy, flat dosing of rFIXFc and rFIX products may be a potentially viable approach in adult hemophilia B subjects that warrants further clinical investigation. Furthermore, using a population PK model, it is feasible to develop a general dosing guidance to achieve target FIX levels recommended for perioperative management in patients with hemophilia B.
Example 4. Population Pharmacokinetic Analysis of a Long-Acting Recombinant Factor IX-Fc Fusion Protein (rFIXFc) in Subjects with Severe Hemophilia B
[0411] BACKGROUND: Clinical dosing of factor IX (FIX) in treatment of hemophilia B is well established based on empirical practice and clinical outcomes. Since pharmacokinetics (PK) of FIX activity is the surrogate efficacy marker, we utilized population PK (popPK) modeling and simulation to evaluate dosing regimens of long-acting recombinant FIX Fc fusion protein (rFIXFc). The PK of rFIXFc, from 135 single-dose and 21 repeat-dose profiles in subjects .gtoreq.12 years old (body weight (BW): 45-186.7 kg), was best described by a 3-compartmental model, which showed modest inter-individual variability (IIV) of 17.7% for clearance (CL) and 21.7% for volume of central compartment (V1). The proportional residue error of 10.6% approximates the variability of the one-stage clotting assay for FIX activity. The only covariate that showed a weak association with rFIXFc PK is BW, which accounted for .about.3% of IIV for CL and V1, suggesting that BW-independent flat dosing of rFIXFc may be feasible for treating adult hemophilia B subjects.
[0412] AIMS: To simulate the BW-based and flat dosing regimens for routine prophylaxis, control of bleeding and perioperative management in the hemophilia B population.
[0413] METHOD: The validated 3-compartmental popPK model, including inter-occasion variability and BW as the covariate on CL and V1, was used for dosing simulations. For BW-based dosing regimen, PK profiles were simulated for 1000 subjects with BW distribution representative of the phase 3 study. BW distribution was simulated using a power function Z=BW-0.5. The generated BW (1000 values) distribution has a median of 74.9 kg and a range of 38.9 to 172.6 kg, which is similar to our studies (median, 73.3 kg; min and max, 45 and 186.7 kg). For fixed dosing regimen, three populations (n=1000 each) were stratified based on low (.ltoreq.10th percentile), typical (10th-90th percentile) and high (>90th percentile) BW. Variability of exposure parameters, percentage of population maintaining target Cmax and trough, and deviations of median exposure parameters in extreme BW groups were compared with BW-based and flat dosing regimens. To simulate steady-state in prophylaxis regimen, six doses were applied for all dosing regimens (once weekly, every 10 days, or every 14 days), with each dosing interval assigned as one occasion. To simulate the PK profile following an episodic treatment, a single dose was applied.
[0414] RESULT: Consistent with the observations from the phase 3 study, popPK simulation of 50 IU/kg once weekly or 100 IU/kg every 10-14 days predicted peak FIX activity within the physiologic range (Cmax <150%) and trough .gtoreq.1% in majority of the population. All simulated regimens predicted that the majority of the population will maintain trough activity at or above 1% (Table 6).
TABLE-US-00006 TABLE 6 Predicted percentage of population with steady-state trough at or above 1% for various prophylaxis dosing regimens % of population Regimen Total weekly dose with trough .gtoreq.1% 50 IU/kg weekly 50 95.4 100 IU/kg weekly 100 99.6 100 IU/kg every 10 days 70 89.2 100 IU/kg every 14 days 50 52.8
[0415] A plot showing a population simulation of steady-state FIX activity vs. time is shown in FIG. 11. Table 7 shows the predicted steady state FIX activity over the course of 14 days for two dosing regimens: 50 IU/kg weekly and 100 IU/kg every 14 days.
TABLE-US-00007 TABLE 7 Predicted steady state FIX activity EOI Day 1 Day 3 Day 5 Day 7 Day 10 Day 14 median median median median median median median [5th, [5th, [5th, [5th, [5th, [5th, [5th, Dose, IU/kg 95th] 95th] 95th] 95th] 95th] 95th] 95th] 50 IU/kg weekly 52.6 16.9 7.17 4.16 2.67 NA NA [32.1, [11.2, [3.85, [1.93, [1.02, 89.3] 26.1] 12.3] 7.83] 5.49] 100 102 30.0 12.0 6.78 4.28 2.29 1.07 100 IU/kg [60.0, [19.6, [6.62, [3.24, [1.82, [0.688, [0.0758, every 14 days 166] 46.7] 19.9] 12.2] 8.06] 5.33] 3.23]
[0416] Furthermore, BW-based and flat dosing resulted in comparable PK profiles with comparable exposure parameters, e.g., 50 IU/kg and 4000 IU once weekly predicted a median (5th, 95th percentile) Cmax of 52.6 (32.1, 89.3) IU/dL and 56.1 (36.2, 90.9) IU/dL, respectively. Both dosing regimens predicted that >95% of the population maintains Cmax <150% and trough .gtoreq.1% (FIG. 12). However, BW-based and flat dosing showed differential effects on the exposure parameters in extreme (.ltoreq.10th or 90th percentile) BW populations. This suggests that BW-independent flat dosing may be feasible for patients 12 years and older.
[0417] The popPK model was used to simulate dosing regimens for episodic treatment. The model predicts that for the control of bleeding episodes, a single dose of 50 or 100 IU/kg of rFIXFc is sufficient to maintain the plasma FIX peak activity levels at 40 to 80 IU/dL (Table 8) as recommended by the World Federation of Hemophilia (WFH) guidelines.
TABLE-US-00008 TABLE 8 Predicted FIX activity profile after a single dose of rFIXFc in the 5th to 95th percentile of the population rFIXFc dose, median [5th, 95th] 50 IU/kg 100 IU/kg End of infusion 50.8 [30.4, 84.5] 102 [60.8, 169] 12 hours 21.1 [13.5, 33.6] 42.3 [26.8, 67.3] 24 hours (day 1) 14.8 [9.78, 22.7] 29.5 [19.6, 45.5] 36 hours 10.9 [6.79, 17.1] 21.8 [13.7, 34.1] 48 hours (day 2) 8.51 [5.14, 13.2] 17.0 [10.5, 26.6] 72 hours (day 3) 5.57 [3.05, 9.27] 11.1 [6.22, 18.5] Day 5 3.07 [1.44, 5.62] 6.14 [3.05, 11.0] Day 7 1.93 [0.795, 3.71] 3.88 [1.82, 7.28] Day 10 1.1 [0.277, 2.33] 2.19 [0.775, 4.56] Day 14 0.559 [0, 1.38] 1.08 [0.125, 2.58]
[0418] Analysis of 12 major surgeries and 2 minor surgeries found that the FIX activities measured during the perioperative period were largely consistent with the prediction by popPK based on subjects' pre-surgery baseline PK, indicating no substantial factor consumption in these surgeries. A representative plot of observed and predicted perioperative FIX activity is shown in FIG. 10. Simulated and observed FIX activities were compared within the first 21 days after the first rFIXFc surgical dose (n=14; 12 major surgeries, 2 minor surgeries). There was good correlation between the observed FIX activity data and that predicted by the PK model (relative prediction error [95% CI], 0.332% [-2.08%, 1.42%]).
[0419] CONCLUSION: PopPK provides a robust and effective means to evaluate potential dosing regimens. The predictions by popPK simulation for rFIXFc corroborate the results from the phase 3 study. The simulations of BW-based and flat dosing of rFIXFc achieved similar PK profiles. Considering the wide therapeutic range for factor replacement therapy, flat dosing of rFIXFc and rFIX products may be a potentially viable approach in adult hemophilia B subjects that warrants further clinical investigation. Furthermore, using a population PK model, it is feasible to develop a general dosing guidance to achieve target FIX levels recommended for perioperative management in patients with hemophilia B.
Example 5. Population Pharmacokinetic Analysis of a Long-Acting Recombinant Factor IX-Fc Fusion Protein (rFIXFc) in Subjects with Severe Hemophilia B
[0420] BACKGROUND: Population pharmacokinetic (PK) models are developed to understand the sources of variability in dose requirements (covariates) and to help individualize dosing regimens if necessary. Dosing histories and subject-specific data are used to gain an understanding of drug disposition in order to discern specific demographic and/or clinical factors that may be predictors of PK parameters. By characterizing the population PK (popPK) of long-acting FIX-Fc (rFIXFc) in subjects with severe hemophilia B (.ltoreq.2 IU/dL plasma FIX activity), a model of estimated population PK parameters of rFIXFc can be established. This model may assist physicians who wish to tailor dosing for individual subjects with sparse PK samples.
[0421] METHODS: Male subjects with severe hemophilia B were included from a phase 1/2a study (n=12) and the phase 3 study (B-LONG, n=123) described above. The subjects ranged in age from 12 to 76 years and in body weight from 45 to 186 kg. The modeling dataset included 135 baseline PK profiles at Week 1, as well as 21 repeat PK profiles at Week 26, with a total of 1400 measured FIX activity records. The final population PK model was validated using 1027 trough/peak FIX activity records from 119 subjects.
[0422] In the popPK analysis, plasma FIX activity was measured by the one-stage (activated partial thromboplastin time) clotting assay. Corrected FIX activity was calculated using the formula:
Corrected FIX activity=Measured FIX activity-Baseline-Residual decay. (F)
[0423] Baseline FIX activity was defined as the lowest level of activity (LLACT) recorded at screening, predose, postdose, or from historical clinical records. When the baseline is equal to 0, the LLACT is less than 1% (lower limit of quantification). When the baseline FIX activity is equal to LLACT, LLACT is greater than or equal to 1% and less than or equal to 2%.
[0424] Prestudy residual decay was performed using terminal half-life obtained from a noncompartmental analysis of the individual data by the following formula:
Residual decay=(predose-baseline).times.e.sup.-decay rate.times.time. (G)
[0425] For the popPK model development, NONMEM VII version 1.0 (ICON Development Solutions, Ellicott City, Md.) was used. The modeling and qualification steps are presented below in Table 9.
TABLE-US-00009 TABLE 9 Modeling and Qualification Steps Steps Model selection Base model and Inter-individual Base Model, IIV on CL/V1/Q2/V2/Q3 variability (IIV) evaluation Inter-occasion variability Base Model with IOV on CL and V1 (IOV) evaluation Covariate Modelling Final model, body weight as covariate on CL and V1 Internal qualification (bootstrap and VPC) External qualification using trough/peak records CL, clearance; V, volume of distribution; Q, inter-compartmental clearance; VPC, visual predictive check
[0426] A first order conditional estimation with interaction method (FOCEI) was used to estimate the popPK parameters. Residual errors were modeled as combined proportional and additive errors. Stepwise forward addition (p<0.005) and backward elimination (p<0.001) covariate modeling was performed. Potential covariates assessed in this analysis included: body weight (BW), Age, Race, Blood type, Human Immunodeficiency Virus status, Hepatitis C Virus status, haematocrit, IgG.sub.1 and albumin concentration, and FIX genotype.
[0427] Model qualifications included bootstrap, visual predictive check (VPC) and validation with trough/peak records. The mean relative prediction error (an indicator of accuracy) was calculated as:
1 N i = 1 i = N [ DV - IPRED ] DV ( H ) ##EQU00002##
[0428] RESULTS: The rFIXFc disposition was best described by a three-compartment base model (FIG. 4). The model was further improved by including intra-subject random changes at different occasions (i.e., inter-occasion variability, IOV) for CL and V1 (FIG. 5). IOV was smaller than inter-individual variability (IIV), indicating that individual PK was more accurate than the mean popPK for individual PK prediction.
[0429] Body weight was found to be a significant covariate for rFIXFc disposition (FIG. 6), although the impact of BW was limited. For example, the BW exponent on CL and V1 was 0.436 and 0.396, respectively, and inclusion of BW reduced inter-individual variability (IIV) for both CL and V1 only by 3.4% and 2.5%, respectively. None of the other covariates assessed, including age, race, blood type or genotype, were significant covariates in this model.
[0430] The final popPK model is summarized below in Table 10.
TABLE-US-00010 TABLE 10 Summary of the final rFIXFc population pharmacokinetic model. Population 95% non-parametric IIV.sup.b IOV Parameter Estimate CI from bootstrap.sup.a (%) (%) CL = Typical CL .times. (BW/73).sup.0.436 Typical CL for a 73 kg 2.39 2.29, 2.49 17.7 15.1 subject (dL/h) BW exponent on CL 0.436 0.272, 0.584 V1 = Typical V1 .times. (BW/73).sup.0.396 Typical V1 for a 73 kg 71.4 58.5, 76.0 21.7 17.4 subject (dL) BW exponent on V1 0.396 0.169, 0.580 Q2 (dL/h) 1.67 1.35, 1.89 35.8 -- V2 (dL) 87.0 79.0, 95.5 46.2 -- Q3 (dL/h) 39.3 16.6, 141 -- -- V3 (dL) 39.9 36.6, 52.4 37.7 -- Residual Error: Proportional 10.6% Additive 0.24 IU/dL CI, confidence interval; IIV, inter-individual variability; IOV, inter occasion variability; CL, clearance; BW, body weight; V, volume of distribution; Q, inter-compartmental clearance
[0431] For a typical 73 kg subject, the predicted popPK values for clearance, volume of central compartment, and volume of distribution at steady state are 2.39 dL/h, 71.4 dL, and 198 dL, respectively. Goodness-of-fit plots show that the predicted popPK data generated by the model closely mimic the observed FIX activity data (FIG. 7).
[0432] The results of the popPK model were validated using the observed FIX activity data. The median and 80% interval for observed and predicted FIX activity time profiles nearly overlapped, indicating that the final model was able to reproduce both the central tendency and variability of the observed FIX activity data on the time scale (FIG. 8). The strong correlation between observed and predicted FIX activities in the trough/peak dataset suggested that the final popPK model is predictive (FIG. 9).
[0433] Finally, the overall relative prediction error was -3.23% with a 95% confidence interval of -5.27% to -1.23%. Post hoc estimates from this popPK analysis were very similar to the results from the conventional PK analysis shown below in Table 11.
TABLE-US-00011 TABLE 11 Post hoc empirical Bayesian estimates of key PK parameters. Phase 3 Phase 1/2a Parameter Mean (SD) Mean (SD) Clearance (CL), mL/h/kg 3.42 (0.89) 2.82 (0.58) Volume of central compartment 102 (29.6) 96.2 (24.7) (V1), mL Incremental in vivo recovery, 1.02 (0.45) 1.04 (0.19) IU/dL per IU/kg Volume of distribution at 297 (90.5) 234 (70.8) steady-state (Vss), mL/kg Terminal Half-life, h 86.7 (27.9) 70.9 (13.9) Mean residence time (MRT), h 89.4 (25.9) 82.5 (15.5) SD, standard deviation
[0434] CONCLUSIONS: The three-compartment popPK model predicted disposition of rFIXFc with modest inter-individual variability (IIV). Individual PK parameters derived from the three-compartment popPK model were similar to those derived from the two-compartment conventional PK analysis, indicating a limited 3rd compartment contribution. For a typical 73 kg subject, the popPK model predicted a clearance of 2.39 dL/h; volume of central compartment of 71.4 dL; and volume of distribution at steady state of 198 dL. The only significant covariate assessed in the popPK model was BW, although its impact on rFIXFc PK variability was limited.
[0435] The final popPK model can be used to simulate dosing regimens and intervals for routine prophylaxis, control and prevention of bleeding episodes, and peri-operative management. This model may assist physicians who wish to tailor dosing for individual subjects with sparse PK samples.
Example 6. Use of the Population Pharmacokinetic Model of rFIXFc to Simulate or Estimate Individualized and Median Patient Treatment Information
[0436] As is discussed in Examples 5 and 7, a model of estimated population PK parameters of rFIXFc has been established that can assist physicians and other healthcare practitioners who wish to tailor dosing for individual subjects with, e.g., sparse PK samples. Alternatively, the model can be used to determine dosing based on PK data for the whole population (median PK).
[0437] Thus, individualized patient treatment, e.g., pharmacokinetics (PK) and dosing regimens, can be selected using Bayesian estimation (or similar machine learning algorithm) based on the population pharmacokinetic (popPK) model described in Example 5 and 7, above (e.g., Table 10, 13, or 14). In this way, one can determine alternative prophylactic dosing regimens and optimized dosing regimens for pen-operative management that have not previously been studied in the B-LONG trials. Alternatively, the selected dosing regimen is based on population PK (median PK) rather than making an individualized selection.
[0438] In some embodiments, the rFIXFc popPK model of Example 5 and 7 (e.g., Table 10, 13, or 14) is used without the Bayesian or similar machine learning algorithm.
[0439] In some embodiments of this aspect of the invention, the method is carried out on a computer-based system, e.g., a server, a desk top computer, a lap top computer, a tablet, a hand held device, or a smart phone. In some embodiments, the computer-based system is a computer application. The computer-based system includes a storage medium for the rFIXFc popPK model discussed in Example 5 and 7, e.g., the parameters of Table 10, 13, or 14. In some embodiments, the storage medium can also contain a Bayesian estimating program, e.g., NONMEM or Phoenix NLME. E.g., Example 5 and 7 (e.g., Table 10, 13, or 14); Kiang et al., Clin. Pharmacokinet 51:515-525 (2012).
[0440] In some embodiments, the system comprises two or more computer-based systems. In some embodiments, the user can input information into a first computer-based system that communicates with a second computer-based system, and the second computer-based system carries out calculations and communicates output information to the first computer-based system. This output information can include recommendations about individualized or non-individualized dosing regimens.
[0441] In some embodiments, the user inputs information into the system and the system calculates and outputs one or more PK or dosing regimens. In some embodiments, the system uses the received information to calculate and output individualized or median PK information. In some embodiments, the system calculates individualized dosing or interval information.
[0442] Information that can be input by a user and received by the system includes patient information and desired treatment outcome information. Based on the type and value of the received information, the computer-based system calculates output information based on the rFIXFc popPK model and optional machine learning algorithm on the storage medium.
[0443] Patient information includes, e.g., age, body weight, diagnostic (baseline) FIX level, PK determinations, time of PK sampling, dosing history if PK samples were taken from multiple doses, actual dose, FIX activity level, etc.
[0444] Desired treatment outcome information includes desired PK or desired regimen outcome, e.g., desired rise in plasma FIX activity level following dose, desired dosing interval, and desired dose.
[0445] Based on the information that was input and received by the system, the system can output various information, e.g., PK curve, PK parameter such as incremental recovery (Cmax/dose), mean residence time, terminal t1/2, clearance, Vss, AUC/dose, doses and associated troughs, and intervals and associated troughs.
[0446] For example, for assessing individualized patient PK, the system can recommend that the user input 2-3 optimized PK sampling time points. In this case, system output can include PK curve and one or more selected PK parameters, e.g., incremental recovery (Cmax/Dose), mean residence time, terminal t1/2, clearance, Vss, AUC, and time to 1 or X %, etc. E.g., FIG. 13.
[0447] As additional examples, to select an individualized dosing regimen using the output individual PK parameters discussed in the preceding paragraph, (i) the dose selected for acute treatment can be based on user input of the desired rise in plasma FIX activity level following the dose, (ii) the dose selected for prophylaxis can be based on user input of the desired dosing interval, or (iii) the selected interval for prophylaxis can be based on user input for the desired dose. In the first case, the system can output the dose (IU) based in the patient's incremental recovery. E.g., FIG. 14. In the second case, system output can be a table of doses and associated troughs, e.g., x IU/kg, 1% trough, y IU/kg, 2% trough, etc. e.g., FIG. 15, top. In the third case, system output can be a table of intervals and associated troughs, e.g., x days, 1% trough, y IU/kg, 2% trough, etc., E.g., FIG. 15, bottom.
[0448] The user may wish to use the system without inputting any individualized PK data. In this case, the dosing output would be based on the population median rather than being individualized for the particular patient. E.g., FIG. 16. In this way, the user inputs, e.g., body weight and age, and (i) the desired rise in plasma FIX activity level following the dose, (ii) the desired dose interval for prophylaxis, or (iii) the desired dose for prophylaxis. In the first case, the system can output the dose. In the second case, the system can output the dose and associated trough, e.g., Table 16. In the third case, the system can output the interval and associated trough, e.g., Table 16.
[0449] Age can be input to determine if the system is suitable for the patient because the current version of the popPK model was built for patients 12 years and older.
[0450] In some embodiments, the system is compliant with patient privacy laws. In some embodiments, the system is encrypted, e.g., with SSL. In some embodiments, input patient information is made anonymous.
[0451] In some embodiments, the system includes a user help function.
[0452] The user can be, e.g., a physician, a nurse, or another healthcare practitioner.
[0453] In some embodiments, the method further includes selecting a dosing regimen based on the system's output information and administering rFIXFc to the patient according to the selected regimen.
Example 7. Population Pharmacokinetic Modeling of Long-Acting Recombinant Factor IX Fc Fusion Protein (rFIXFc) in Patients with Hemophilia B
[0454] Background and Objectives: Recombinant factor IX Fc fusion protein (rFIXFc) is a clotting factor developed using monomeric Fc fusion technology resulting in a longer circulating half-life. The objective of this analysis is to elucidate the pharmacokinetic characteristics of recombinant factor IX Fc fusion protein (rFIXFc) in patients with hemophilia B and identify covariates that affect rFIXFc disposition.
[0455] Methods: Population pharmacokinetic analysis using NONMEM.RTM. was performed with clinical data from two completed trials in previously treated patients with severe to moderate hemophilia B. Twelve patients from a phase 1/2a study and 123 patients from a registrational phase 3 study were included in this population pharmacokinetic analysis.
[0456] Results: A three-compartmental model was found to best describe the pharmacokinetics of rFIXFc. For a typical 73-kg patient, population predicted clearance (CL), volume of central compartment (V.sub.1), and volume of distribution at steady state (V.sub.ss) were 2.39 dL/h, 71.4 dL and 198 dL, respectively. Because of repeat pharmacokinetic profiles at week 26 for patients in a subgroup, inclusion of inter-occasion variability (IOV) on CL and V.sub.1 were evaluated and significantly improved the model. The magnitude of IOV on CL and V.sub.1 were both low to moderate (<20%) and less than the corresponding inter-individual variability. Body weight (BW) was found to be the only significant covariate for rFIXFc disposition. However, the impact of BW was limited, as the BW power exponents on CL and V.sub.1 were 0.436 and 0.396, respectively.
[0457] Conclusions: This is the first population pharmacokinetic analysis that systematically characterized the pharmacokinetics of long-acting rFIXFc in patients with hemophilia B. The population pharmacokinetic model for rFIXFc can be utilized to evaluate and optimize dosing regimens for the treatment of patients with hemophilia B.
[0458] 1. Background
[0459] Hemophilia B is a rare bleeding disorder caused by a deficiency of coagulation factor IX (FIX). The disease is caused by a mutation on the X chromosome and affects approximately 1 in 30,000 males. Hemophilia B results in abnormal clot formation, causing prolonged and abnormal bleeding, including bleeding into joints, soft tissue, muscle and body cavities. Bleeding episodes may be associated with trauma or occur in the absence of trauma (spontaneous bleeding). If not treated appropriately, bleeding can be life-threatening or result in significant morbidity. The current mainstay of treatment is FIX replacement therapy.
[0460] Recombinant factor IX Fc fusion protein (rFIXFc) is a recombinant protein consisting of a single molecule of FIX covalently fused to the Fc domain of human immunoglobulin G1 (IgG1) with no intervening sequence. The Fc domain is responsible for the long circulating half-life of IgG1 through interaction with the neonatal Fc receptor (FcRn) that is expressed in many different cell types. rFIXFc was therefore designed as a long-acting version of recombinant FIX. rFIXFc has the potential to fulfill an unmet medical need by providing a long-acting therapy for control and prevention of bleeding episodes, routine prophylaxis and perioperative management in patients with hemophilia B. Two clinical trials with rFIXFc have been completed in previously treated patients with severe to moderate hemophilia B (with .ltoreq.2 IU/dL [%] endogenous FIX): one single dose phase 1/2a study in 14 patients (12 of them who received doses .gtoreq.12.5 IU/kg had pharmacokinetic assessment) [6], and one registrational phase 3 study in 123 patients [8]. rFIXFc was shown to be well tolerated and efficacious in the treatment of bleeding, routine prophylaxis and perioperative management.
[0461] The purpose of this analysis is to characterize the population pharmacokinetics of rFIXFc in patients with hemophilia B and to identify demographic and clinical factors that are potential determinants of rFIXFc pharmacokinetic variability. The population pharmacokinetic model of rFIXFc can be used to evaluate and guide dosing regimens of rFIXFc in the treatment of patients with hemophilia B.
[0462] 2 Methods
[0463] 2.1 Clinical Studies
[0464] FIX activity data were obtained from two completed clinical trials in previously treated patients with severe to moderate hemophilia B. Twelve evaluable patients from the phase 1/2a study and 123 patients from the phase 3 study (B-LONG) who had measurable FIX activities were included in this population pharmacokinetic analysis. The clinical studies are summarized in FIGS. 2A and 2B. All subjects were patients with severe to moderate hemophilia B previously treated with FIX products, from 12.1 to 76.8 years of age. All patients, or patient guardians, gave informed written consent. The studies were approved by the Ethics committee and conducted in accordance with the International Conference on Harmonisation guidelines for Good Clinical Practice.
[0465] 2.2 Pharmacokinetic Sampling and Bioanalytical Methods
[0466] In the phase 1/2a study, 12 patients underwent rFIXFc pharmacokinetic sampling up to 14 days. In the phase 3 study, pharmacokinetic samples were collected for rFIXFc in all patients according to the schedule in FIG. 2C. Pharmacokinetic profiles of rFIXFc were assessed at week 1 (baseline) for all patients and at week 26 for the Arm 1 sequential pharmacokinetic subgroup. For patients on prophylaxis in Arms 1 and 2, additional trough and peak samples were collected at clinical visits throughout the study.
[0467] The population pharmacokinetic modeling was performed using plasma FIX activity data as measured by the one-stage activated partial thromboplastin time (aPTT) clotting assay using commercially available aPTT reagents (Trinity Biotech) and normal reference plasma (Precision BioLogic). Lower limit of quantitation (LLOQ) was 1 IU/dL (%). The accuracy of the assay was within 95-104%, and the intra- and inter-assay precision was approximately 10%.
[0468] 2.3 Data Handling
[0469] A total of 11 data post-infusion were below the limit of quantification (BLQ, below LLOQ of 1%). Since those post-infusion BLQ values represent <0.5% of the observations, they were excluded from the analysis as the first step of data handling.
[0470] The one-stage clotting assay does not distinguish between FIX activities resulting from endogenous baseline residual activity and incomplete washout of the pre-study FIX product or the input study drug, rFIXFc. Therefore, the baseline and residual activity corrections were applied to the observed FIX activity data (formulas (I) and (J)). The corrected FIX activities were recorded as the dependent variable (DV) in the population pharmacokinetic dataset. Similar baseline and residual activity corrections were reported previously for the pharmacokinetic analyses of other FIX products [12-15]. See Bjorkman et al., Eur J Clin Pharmacol. 2012; 68(6):969-77; Bjorkman et al., Eur J Clin Pharmacol. 1994; 46(4):325-32; Bjorkman et al., Haemophilia. 2001; 7(2):133-9; and Carlsson et al., Haemophilia. 1998; 4(2):83-8.
Residual decay correction=(Predose-baseline).times.e.sup.decay rate.times.time (I)
Corrected FIX activity=Measured FIX activity-baseline-residual decay correction (J)
[0471] The endogenous baseline FIX activity level is dictated by the defective FIX genotype and thus is stable in each individual subject, yet could be overestimated in patients receiving FIX replacement therapy who underwent incomplete washout. Therefore the baseline FIX activity was defined as the lowest FIX activity observed throughout the study, including all the screening, pre-dose, and post-dose records. For patients whose lowest observed FIX activity was <1% (LLOQ), the baseline FIX activity was set at 0; for patients whose lowest observed FIX activity was between 1-2%, the baseline FIX activity was set at the lowest observed FIX activity. The study enrollment was limited to subjects with baseline FIX activity .ltoreq.2%.
[0472] For each individual subject, baseline activity was first subtracted from observed FIX activity and then residual activity, if any, was decayed from baseline-corrected FIX activity to obtain the corrected FIX activity. Residual activity was defined as pre-dose activity minus baseline FIX activity. For subjects in the Arm 1 sequential pharmacokinetic subgroup who underwent pharmacokinetic assessment with the comparator FIX product (BENEFIX.RTM., Pfizer Inc, New York, N.Y.) prior to rFIXFc pharmacokinetic assessment, the residual activity was decayed using the individual subject's BENEFIX.RTM. terminal first-order decay rate estimated by the non-compartmental analysis in PHOENIX.TM. WinNonlin 6.2 (Pharsight, Sunnyvale, Calif.). For any subjects who did not have a BENEFIX.RTM. pharmacokinetic assessment, the residual activity was decayed from the rFIXFc pharmacokinetic profiles using the average BENEFIX.RTM. terminal first-order decay rate from the Arm 1 sequential pharmacokinetic subgroup.
[0473] 2.4 Modeling Strategy and Datasets
[0474] Demographic and clinical factors collected and examined in the analysis included age, body weight (BW), race, height, human immunodeficiency virus (HIV) and hepatitis C virus (HCV) status, IgG1 and albumin concentration, hematocrit (HCT) level, FIX genotype and blood type.
[0475] The pharmacokinetic dataset was split into the modeling dataset, which was used to build the population pharmacokinetic model and validation dataset, which was used to qualify the final model. The modeling dataset for rFIXFc included 1400 FIX activity records from 135 baseline pharmacokinetic profiles in both phase 1/2a and 3 studies, as well as 21 repeat pharmacokinetic profiles that were collected at week 26 from the Arm 1 sequential pharmacokinetic subgroup in the phase 3 study. The validation dataset included 1027 trough/peak FIX activity records from the phase 3 study, excluding the records during and after surgeries. Peak/trough collection times were recorded by patients retrospectively into their electronic diary following the clinic visit. A summary of the modeling and validation datasets is listed in Table 12.
TABLE-US-00012 TABLE 12 Summary of modeling and validation datasets No. of FIX Median age Median body weight Dataset No. of patients activity records (year [range]) (kg [range]) Modeling dataset 12 (Phase 1/2a) 1,400 31.3 (12.1-76.8) 73.3 (45.0-186.7) 123 (Phase 3) Validation dataset 100 (Phase 3) 1,027 30.7 (12.1-71.6) 72.5 (45.2-186.7)
FIX Factor IX
[0476] The modeling strategy was a two-step approach. The first step was to build the population pharmacokinetic model using the modeling dataset and the second step was to validate the model with goodness-of-fit plots, bootstrapping, visual prediction check (VPC) and the trough/peak validation dataset. As a comparison, the rFIXFc model using the full dataset, which combined the modeling and validation dataset, was also developed.
[0477] 2.5 Population Pharmacokinetic Modeling
[0478] NONMEM.RTM. 7 version 1.0 (ICON Development Solutions, Ellicott City, Md., USA) with an Intel Fortran compiler (version 12) was used for the population pharmacokinetic model development. Statistical program R (version 2.15.0, R Foundation for Statistical Computing, Vienna, Austria) was used to compile NONMEM datasets and generate graphics. Perl Speaks NONMEM (PsN, version 3.5.3) (Lindbom et al., Comput Methods Programs Biomed. 2004; 75(2): 85-94) was used to conduct bootstrapping. PsN and Xpose 4 (Jonsson et al., Comput Methods Programs Biomed. 1999; 58(1): 51-64) were used to perform VPC.
[0479] A first-order conditional estimation with interaction method (FOCEI) was used to estimate population pharmacokinetic parameters. Inter-individual variability (IIV) was modeled using exponential function. The inclusion of IIV terms on pharmacokinetic parameters was tested sequentially, with the most significant objective function value (OFV) reduction (P<0.005) entering the model first. Inter-occasion variability (IOV) (Karlsson et al., J. Pharmacokinet-Biopharm. 1993: 21(6): 735-50) was also evaluated. For the modeling dataset, two occasions were defined including baseline pharmacokinetic profiling at week 1 and repeat pharmacokinetic profiling at week 26. For the full dataset, six occasions were defined according to the data density. Residual errors were modeled as combined proportional and additive errors.
[0480] Plots of IIV versus covariates were used to screen for potential demographic and clinical factors that affect rFIXFc pharmacokinetics. For continuous covariates, scatter plots of ETA (IIV code used in NONMEM) versus covariates were overlaid with a non-parametric locally weighted smoother LOESS line to determine functional relationships; for categorical covariates, box and whisker plots were used to identify potential differences between groups (data not shown). A clear trend of positive or negative slopes and noteworthy correlation coefficients (data not shown) would suggest a possible influence by the continuous covariates; pronounced differences among the groups would suggest a possible influence by the categorical covariates. After identifying potential covariates, a full stepwise forward addition (P<0.005) and backward elimination (P<0.001) procedure was conducted for covariate modeling.
[0481] Besides statistical considerations, model selection was also aided by goodness-of-fit plots, including DV (observed FIX activity adjusted for baseline activity and residual decay) versus population prediction (PRED), DV versus individual prediction (IPRED), conditional weighted residual (CWRES) versus TIME and PRED plots. See Wade et al., AAPS J. 2005; 7(2): 45; and Ette et al., Pharm Res. 1995; 12(12); 1845-55. Other diagnostics also helped to select the proper model, including parameter precision, ETA, and CWRES distribution and shrinkage. See Savic et al., AAPS J. 2009; 11(3): 558-69; and Xu et al., AAPS J. 2012; 14(4); 927-36.
[0482] 2.6 Model Qualification
[0483] Bootstrapping was conducted with 1,000 datasets generated by random sampling through replacement. Non-parametric median and 95% (2.5.sup.th and 97.5.sup.th percentiles) confidence intervals (CIs) of pharmacokinetic parameters were obtained and compared with final model estimates.
[0484] To check the predictive performance of the model, VPC was performed to obtain 1,000 simulated pharmacokinetic profiles. Median, 10th, and 90th percentile of simulated and observed FIX activities, stratified by dose (50 and 100 IU/kg), were plotted.
[0485] The trough/peak validation dataset was used to check the predictability of the model. Specifically, the model was used to derive Bayesian feedback predictions of FIX activities at trough/peak time points by setting MAXEVAL=0 in NONMEM control stream. The mean relative prediction error (an indicator of accuracy) was calculated using formula:
1 N i = 1 i = N DV - IPRED DV ( K ) ##EQU00003##
[0486] 3. Results
[0487] 3.1 Structural Model and Evaluation of IIV
[0488] Based on previous conventional pharmacokinetic analyses of rFIXFc, a two-compartment model appropriately described individual pharmacokinetics, hence a two-compartment model was evaluated first followed by a three-compartment model. IIV (ETA, values) was assumed for clearance (CL) and volume of compartment 1 (V.sub.1). A covariance between CL and V.sub.1 was also included. The three-compartment model resulted in a reduction of OFV by over 400 units (for additional four parameters) compared with the two-compartment model, thus was selected as the base model (FIG. 4). Primary pharmacokinetic parameters included CL, V.sub.1, volume of compartment 2 (V.sub.2) and 3 (V.sub.3), inter-compartmental clearance between compartments 1 and 2 (Q.sub.2), as well as between 1 and 3 (Q.sub.3). The inclusion of IIV for the rest of the pharmacokinetic parameters (V.sub.2, V.sub.3, Q.sub.2 and Q.sub.3) led to further improvement in the model fitting. However, IIV on Q.sub.3 was associated with a high standard error (87%), indicating that the data cannot support a precise estimation of IIV on Q.sub.3, which was thus not included in the model. No additional covariance between IIV of pharmacokinetic parameters could be estimated with precision, thus the only covariance between IIV retained in the model was the covariance between IIV on CL and V.sub.1.
[0489] 3.2 Evaluation of IOV
[0490] Since the Arm 1 sequential pharmacokinetic subgroup had repeat pharmacokinetic profiles at week 26 in addition to baseline pharmacokinetic profiles at week 1, IOV was evaluated with baseline pharmacokinetics as occasion 1 and repeat pharmacokinetics as occasion 2. The inclusion of IOV on CL significantly improved the model with a reduction of OFV by 171.6 units. The inclusion of IOV on both CL and V.sub.1 achieved an additional OFV drop of 41.6 units, whereas IOV on V.sub.2 or Q.sub.2 did not improve the model fit (P>0.05). The IOV on V.sub.3 improved the model fit at P<0.005 but with a large percentage of relative standard error (78.4%); Therefore, IOV was only included for CL and V.sub.1.
[0491] Pairwise comparisons of CL and V.sub.1 estimates for baseline and repeat pharmacokinetics, derived from the base model with IOV, were plotted in FIG. 5. The changes of either CL or V.sub.1 between the two occasions were random and small with only one exception, and the mean CL or V.sub.1 for the two occasions were similar.
[0492] Overall, the inclusion of IOV reduced the corresponding IIV on CL and V.sub.1 from 24.0% and 29.6% to 21.1% and 24.2%, respectively. The inclusion of IOV also reduced proportional and additive residual errors from 12.1% and 0.30 IU/dL, to 10.5% and 0.24 IU/dL, respectively. The base model with IOV provided a reasonable fit to the data, and explained the random as well as small pharmacokinetic changes between occasions studied in the trial, therefore was chosen for further covariate modeling.
[0493] 3.3 Covariate Modeling
[0494] Based on ETA versus covariate plots, BW, albumin and race on CL, and "study" on V.sub.2 were speculated to be potential covariates. Covariate modeling included BW on all pharmacokinetic parameters, albumin on CL, and "study" on V.sub.2 and CL. BW was assessed for all pharmacokinetic parameters because it is an important physiology factor. "Study" was assessed on CL because of the importance of CL.
[0495] A full stepwise forward addition and backward elimination procedure was performed. Following the forward covariate inclusion, the full covariate model was identified with BW on CL and V.sub.1, and "study" on V.sub.2. However, "study" on V.sub.2 was removed following the backward elimination procedure (P>0.001).
[0496] Further, the potential residual variability difference between the phase 1/2a and 3 studies was tested by including two sets of proportional and additive errors for two studies in the residual error model. No significant reduction in OFV was observed (13.7 units, df=2).
[0497] Therefore, although the phase 1/2a and phase 3 studies have different dosing and sampling schemes, the population pharmacokinetic modeling did not suggest a PK difference between the two studies.
[0498] 3.4 Final Model
[0499] The final model of rFIXFc had IIV on CL/V.sub.1/Q.sub.2/V.sub.2/V.sub.3 but not Q.sub.3, IOV on CL and V.sub.1 and BW as a covariate on CL and V.sub.1. The model described the data well (FIG. 4). There were no outstanding trends observed in the CWRES plots and most CWRES were randomly distributed between -2 and 2, indicating overall small discrepancies between measured FIX activities and population predictions (FIGS. 7C and 7D). Population pharmacokinetic parameter estimates, IIV and IOV, as well as residual errors were estimated with precision, evidenced by narrow 95% CIs for each pharmacokinetic parameter (Table 3). The IIV for CL and V.sub.1 were 17.7 and 21.7%, respectively, which are low to moderate, and IOV for CL and V.sub.1 were low at 15.1 and 17.4%, respectively.
[0500] The magnitude of ETA shrinkage on the IIVs was moderate (<30% for all pharmacokinetic parameters with IIV terms), while the magnitude of ETA shrinkage on the IOV was occasion-specific, moderate at first occasion (around 30% on CL and V.sub.1) and higher at occasion 2 (around 70%) because there were fewer pharmacokinetic profiles for the second occasion (21 for occasion 2 repeat pharmacokinetics vs. 135 for occasion 1 baseline pharmacokinetics). The distributions of ETAs and CWRES showed approximate normal distribution centered around zero without apparent skewness (data not shown). This was consistent with the ETABAR P values, all of which were non-significant (P>0.05).
[0501] 3.5 Model Qualification
[0502] Non-parametric bootstrapping was applied to the final model to assess the model stability. Bootstrapping generated medians and CIs for the pharmacokinetic parameters, IIV and IOV estimates (Table 13). The median values from the bootstrapping were very similar to the model estimates for all the pharmacokinetic parameters.
TABLE-US-00013 TABLE 13 Summary of rFIXFc population pharmacokinetic final model Model Bootstrap median Parameter estimate (95% CI.sup.a) CL = Typical CL .times. ( BW 73 ) 0.436 ##EQU00004## Typical CL for a 73-kg patient 2.39 2.39 (2.29, 2.49) (dL/h) BW exponent on CL 0.436 0.437 (0.272, 0.584) V 1 = Typical V 1 .times. ( BW 73 ) 0.396 ##EQU00005## Typical V.sub.1 = for a 73-kg 71.4 71.2 (58.5, 76.0) patient (dL) BW exponent on V.sub.1 0.396 0.390 (0.169, 0.580) Q.sub.2 (dL/h) 1.67 1.66 (1.35, 1.89) V.sub.2 (dL) 87.0 87.0 (79.0, 95.5) Q.sub.3 (dL/h) 39.3 39.0 (16.6, 141) V.sub.3 (dL) 39.9 41.2 (36.6, 52.4) IIV.sup.b on CL, % 17.7 17.5 (11.8, 22.4) IOV.sup.c on CL, % 15.1 15.0 (10.7, 19.1) IIV on V.sub.1, % 21.7 22.4 (15.5, 32.1) IOV on V.sub.1, % 17.4 16.5 (8.7, 22.8) IIV on Q.sub.2, % 35.8 35.0 (22.6, 45.8) IIV on V.sub.2, % 46.2 45.9 (38.0, 55.3) IIV on V.sub.3, % 37.7 37.9 (30.2, 54.3) Correlation between IIV on 75.6 74.8 CL and V.sub.1, %. Proportional residual error, % 10.6 10.4 (8.64, 12.0) Additive residual error, IU/dL 0.24 0.24 (0.17, 0.31) .sup.a95% CI: Non-parametric 95% CI from bootstrap results with 1,000 datasets .sup.bIIV calculated as {square root over (variance)} .times. 100 .sup.cIOV calculated as {square root over (variance)} .times. 100 BW body weight, CI confidence interval, CL clearance, IIV inter-individual variability, IOV inter-occasion variability, Q.sub.2 inter-compartmental clearance of compartment 2, Q.sub.3 inter-compartmental clearance of compartment 3, rFIXFc recombinant factor IX Fc, V.sub.1 volume of compartment 1, V.sub.2 volume of compartment 2, V.sub.3 volume of compartment 3
[0503] The graphic results of the VPC of the final model stratified by the dose are presented in FIG. 8. The median and 80% interval (10.sup.th to 90.sup.th percentile) time-activity observed and predicted profiles nearly overlapped, indicating that the final model was able to reproduce both the central tendency and variability of the observed FIX activity time profiles.
[0504] The predictive capability of the final model was further evaluated using a validation dataset, which contains the trough/peak FIX activity records that were not included in the modeling dataset. The final model was used to derive the individual predictions for the trough and peak observations. Individual predictions showed good correlation (R.sup.2=0.9857, P<0.001) with the observations (FIG. 9). The mean relative prediction error was low at -3.23%, indicating that the final model was qualified to predict rFIXFc pharmacokinetics in the hemophilia B patient population.
[0505] 3.6 Full Dataset Model
[0506] Further, a population pharmacokinetic model of rFIXFc was also built based on the full dataset, including both pharmacokinetic profile and trough/peak data. The population parameter estimates of the resulting model, as well as IIV and IOV (Table 14 below), were comparable with those of the final model derived from the modeling dataset (Table 13 above). The goodness-of-fit plots indicated that the model also described the data adequately (FIG. 20). A slightly greater over-prediction of FIX activity in the lower range (<10 IU/dL) was observed for the VPC of the full dataset model. (FIGS. 8C and 8D).
TABLE-US-00014 TABLE 14 Summary of rFIXFc population pharmacokinetic model derived from the full dataset Parameter Population estimate (95% CI).sup.a CL = Typical CL .times. ( BW 73 ) 0.432 ##EQU00006## Typical CL for a 73-kg patient (dL/h) 2.21 (2.10, 2.32) BW exponent on CL 0.432 (0.251, 0.613) V 1 = Typical V 1 .times. ( BW 73 ) 0.517 ##EQU00007## Typical V.sub.1 = for a 73-kg patient (dL) 70.6 (66.3, 74.9) BW exponent on V.sub.1 0.517 (0.282, 0.752) Q.sub.2 (dL/h) 163.(1.39, 1.87) V.sub.2 (dL) 991. (84.6, 114) Q.sub.3 (dL/h) 45.6 (35.6, 55.6) V.sub.3 (dL) 40.7 (38.3, 43.1) IIV.sup.b on CL, % 19.7 (16.6, 22.8) IOV.sup.c on CL, % 17.8 (17.0, 18.7) IIV on V.sub.1, % 21.7 (17.9, 25.6) IOV on V.sub.1, % 13.8 (12.3, 15.3) IIV on Q.sub.2, % 48.1 (38.5, 57.6) IIV on V.sub.2, % 51.0 (40.6, 61.3) Correlation between IIV on CL and V.sub.1, % 60.7 Proportional residual error, % 14.8 (9.56, 20.1) Additive residual error, IU/dL 0.279 (0.112, 0.445) .sup.a95% CI: The lower and upper limits for 95% CI were calculated asymptotically using the standard errors estimated by the covariance step in NONMEM .sup.bIIV calculated as {square root over (variance)} .times. 100 .sup.cIOV calculated as {square root over (variance)} .times. 100 BW body weight, CI confidence interval, CL clearance, IIV inter-individual variability, IOV inter-occasion variability, rFIXFc recombinant factor IX FC, RSE relative standard error, Q.sub.2 inter-compartmental clearance of compartment 2, Q.sub.3 inter-compartmental clearance of compartment 3, V.sub.1 volume of compartment 1, V.sub.2 volume of compartment 2, V.sub.3 volume of compartment 3.
[0507] 4 Discussion
[0508] This is the first systematic population pharmacokinetic modeling of rFIXFc in patients with hemophilia B. A three-compartment model described the pharmacokinetics of rFIXFc well. For a typical 73-kg patient, V.sub.1 for rFIXFc at 71.4 dL is larger than the plasma volume, which is around 30 dL for a typical adult, indicating that rFIXFc is not limited in the plasma for the initial distribution phase after intravenous administration, similar to that of FIX which is known to bind to collagen IV in the subendothelium. The IIV for CL and V.sub.1 were low to moderate at 17.7% and 21.7%, respectively, which are consistent with those reported for plasma-derived FIX (23% for CL and 19% for V.sub.1). Residual errors were small with a proportional error of 10.6% and additive error of 0.24 IU/dL. The proportional residual error is similar to the inter-assay variability of the one-stage aPTT clotting assay. The small IIV and residual errors indicate that the model described the data adequately and rFIXFc pharmacokinetics do not vary substantially among patients. The estimated IOVs for CL and V.sub.1 were 15.1% and 17.4%, respectively, similar to those reported for plasma-derived FIX (15% for CL and 12% for V.sub.1). The small and randomly distributed IOV on CL and V.sub.1 indicate that rFIXFc pharmacokinetics is relatively stable at different occasions.
[0509] The approach of using the model to estimate baseline and differentiate baseline from pre-dose residual activity for each individual was investigated. However, population modeling cannot reliably separate baseline from residual activity because not every FIX activity profile returned to baseline at the last sampling time point (i.e., the baseline [endogenous] and exogenous signals were confounded). We also investigated setting baseline activity at 0, 0.5, or an individualized baseline. The individualized baseline resulted in relatively conservative pharmacokinetic estimates and more accurate prediction of the trough levels in individual subjects. Therefore, an individualized baseline was chosen to handle the activity data in the population pharmacokinetic modeling, which was also utilized in the conventional pharmacokinetic analysis.
[0510] BW on CL and V.sub.1 was the only covariate that showed a statistically significant impact on rFIXFc pharmacokinetics. It was suggested that the exponent of a physiological or pharmacokinetic parameter shall not revolve around a fixed number. Hence, the exponents of BW on CL and V.sub.1 were estimated during the modeling instead of fixed at presumed values, e.g., 0.75 for CL and 1 for V.sub.1. The estimated BW exponents for CL and V.sub.1 in the final model were markedly lower at 0.436 and 0.396, respectively. Furthermore, inclusion of BW as a covariate decreased IIV for CL by only 3.4% and for V.sub.1 by only 2.5%, suggesting that a considerable portion of the variability was not explained by BW.
[0511] The limited impact of BW was not unique to rFIXFc pharmacokinetics, which was also observed for BENEFIX.RTM. in the phase 3 study (data not shown). The weak correlation between BW and pharmacokinetics in our studies differs from a previous report, which showed that BW, with an exponent of 0.7 on CL, accounted for a significant portion of the variability in BENEFIX.RTM. pharmacokinetics in a two-compartment population pharmacokinetic model. The discrepancy probably can be explained by the different populations studied, i.e., the adult patients (>19 years) in our study versus pooled data from 111 children (.ltoreq.15 years), including 53 infants (<2 years) and 80 adults (>15 years). This previous report represents a wider range for age and BW than in our study. See Bjorkman et al., Haemophilia. 2013; 19(5): 753-7. A recently published paper reported that BeneFIX pharmacokinetics in 56 patients aged 4-56 years and weighing 18-133 kg, described also by a three-compartment model, had allometric exponent of CL terms of 0.66 and volume terms of 0.64. See Id. The slightly reduced allometric exponent of CL compared with the previous report might also be explained by the difference of age and BW range studied. See Udata et al., Blood. 2008; 112(11): 443-4.
[0512] Data splitting is a useful internal model validation approach in population pharmacokinetic modeling. See Sherwin et al., Clin. Pharmacokinet. 2012; 51(9); 573-90. Because in the clinic intensive pharmacokinetic profile data are used to predict subsequent trough/peak sparse data, the data were split into a modeling dataset including the intensive pharmacokinetic profile data from all subjects at week 1 and week 26 and a validation dataset including the sparse peak and trough data throughout the phase 3 study. To verify that our modeling strategy was robust, i.e., building the model with the baseline/repeat pharmacokinetic profiles without additional trough/peak FIX activity records, we also built the model using the full dataset consisting of all the FIX activity records from both the modeling and validation datasets. The two models were highly comparable with <10% difference in the pharmacokinetic parameters, IIV and IOV estimates (Table 13 and Table 14). The comparability between the two models was also demonstrated by the similar VPC plots for the two models (FIG. 8). FIX activities in the lower range (<10 IU/dL) were slightly more over-predicted by the full dataset model. This difference might be attributed to the imprecise recordings of the peak/trough collection time in the full dataset, which was recorded by patients retrospectively into their electronic diary following the clinic visit. The final model derived from the modeling dataset is slightly more accurate in predicting trough levels, which is essential for maintenance of the therapeutic efficacy. Therefore, the final model derived from the modeling dataset is robust and predictive to be used for simulation of the dosing regimens for rFIXFc.
[0513] Finally, the population pharmacokinetic predictions were largely consistent with the results derived from the conventional two-stage pharmacokinetic analysis, which used a two-compartment model, despite a minority (.about.14%) of the pharmacokinetic profiles could also be described by a three-compartmental model. The ambiguity in the model selection in the conventional pharmacokinetic analysis was at least partially due to the different sampling schemes in different study arms. Such ambiguity was avoided using population pharmacokinetic modeling. The post-hoc estimates from this population pharmacokinetic analysis were very similar to the results from the conventional pharmacokinetic analysis (Table 15).
TABLE-US-00015 TABLE 15 Comparison of pharmacokinetic parameters derived from population pharmacokinetic post hoc analysis and conventional pharmacokinetic analysis for phase III study Population Conventional pharmacokinetics post hoc pharmacokinetics analysis Parameter (n = 123) (n = 22).sup.a (units) Geometric mean (95% CI) Geometric mean (95% CI) CL (mL/h/kg) 3.3 (3.2, 3.5) 3.2 (2.8, 3.6) V.sub.ss (mL/kg) 280.8 (266.4, 296) 314.8 (277.8, 356.8) Terminal 81.1 (76.5, 86.1) 82.1 (71.4, 94.5) half-life (h) MRT (h) 84.1 (79.8, 88.6) 98.6 (88.2, 110.3) .sup.aPharmacokinetic parameters derived from 22 patients with intensive sampling schedule in Arm 1 sequential pharmacokinetic subgroup CI confidence interval, CL clearance, MRT mean residual time, V.sub.ss volume of distribution at steady state
[0514] For example, the geometric mean t.sub.1/2 estimated in population pharmacokinetic and conventional pharmacokinetic are 81.1 h and 82.1 h, respectively. The highly comparable pharmacokinetic parameters derived from a two-compartment conventional pharmacokinetic analysis and a three-compartment population pharmacokinetic analysis suggests that the contribution of the third compartment to rFIXFc PK was probably limited, but nevertheless provided better profile definition for the more complex population modeling. The advantage of developing a population pharmacokinetic model for rFIXFc is that the model can be utilized for dosing regimen simulation taking into account IIV and IOV, because FIX activity is considered as a surrogate for efficacy; Further, the population pharmacokinetic model combined with individual sparse pharmacokinetic data can be used to derive an individualized dosing regimen through Bayesian estimation, which can alleviate the requirement for extensive sampling. Since hemophilia is a lifelong disease impacting children as well as adults, the benefit of pharmacokinetics-tailored dosing regimens based on data from limited blood sampling is of great interest to the hemophilia community.
[0515] 5 Conclusion
[0516] This is the first population pharmacokinetic analysis that systematically characterized the pharmacokinetics of the long-acting rFIXFc in patients with hemophilia B. The disposition of rFIXFc was well described by a three-compartment model with low to moderate IIV and IOV. Body weight was found to be the only statistically significant but weak covariate on CL and with limited impact. The qualified population pharmacokinetic model for rFIXFc is appropriate and predictive, providing a valuable tool to evaluate and optimize dosing regimens of rFIXFc for the treatment of patients with hemophilia B.
Example 8. Dosage and Method of Administration/Method of Calculating Initial Estimated Dose
[0517] rFVIIIFc is long-acting anti-hemophilic factor (recombinant) indicated in adults and children (.gtoreq.12 years) with hemophilia A (congenital Factor FVIII deficiency) for, e.g., control and prevention of bleeding episodes, routine prophylaxis to prevent or reduce the frequency of bleeding episodes, and perioperative management (surgical prophylaxis).
[0518] Dosing of rFVIIIFc can be estimated as described in this example, but can also be determined by standard tests such as FVIII activity assays described elsewhere herein.
[0519] 1 IU of rFVIIIFc per kg body weight is expected to increase the circulating level of Factor VIII by 2 [IU/dL]. rFVIIIFc has been shown to have a prolonged circulating half-life.
[0520] Since patients can vary in their pharmacokinetic (e.g., half-life, in vivo recovery) and clinical responses to rFVIIIFc, the expected in vivo peak increase in Factor VIII level expressed as IU/dL (or % of normal) or the required dose can be estimated using the following formulas:
IU/dL (or % of normal)=[Total Dose (IU)/body weight (kg)].times.2 (IU/dL per IU/kg) (L)
OR
Dose (IU)=body weight (kg).times.Desired Factor VIII Rise (IU/dL or % of normal).times.0.5 (IU/kg per IU/dL) (M)
[0521] The following table (Table 16) can be used to guide dosing in bleeding episodes:
TABLE-US-00016 TABLE 16 Guide to rFVIIIFc Dosing for Treatment of Bleeding Desired Factor VIII Level Dose (IU/dL or % (IU/kg)/Frequency Severity of Bleed of normal) of Doses (hrs) Minor and Moderate 40-60 20-30 IU/kg For example: joint, Repeat every 24-48 hours superficial muscle/no until bleeding is resolved neurovascular compromise (except iliopsoas), deep laceration and renal, superficial soft tissue, mucous membranes Major 80-100 40-50 IU/kg For example: iliopsoas Repeat every 12-24 hours and deep muscle with until bleeding is resolved neurovascular injury, or substantial blood loss, retroperitoneum, CNS, throat and neck, gastrointestinal. Adapted from WFH 2012
[0522] Subsequent dosage and duration of treatment depends on the individual clinical response, the severity of the Factor VIII deficiency, and the location and extent of bleeding.
[0523] The following table (Table 17) can be used to guide dosing for perioperative management (surgical prophylaxis):
TABLE-US-00017 TABLE 17 Guide to rFVIIIFc Dosing for Perioperative Management (Surgical Prophylaxis) Target Factor VIII Level Dose (IU/dL or % (IU/kg)/Frequency Type of Surgery of normal) of Doses (hrs) Minor 50 to 80 25-40 IU/kg Minor operations A single infusion can be including uncomplicated sufficient. Repeat every dental extraction 24 hours as needed to control bleeding. Major 80 to 120 An initial preoperative Major operations dose of 40-60 IU/kg including intra- followed by a repeat dose abdominal, joint of 40-50 IU/kg after 8-24 replacement surgery hours and then every 24 hours to maintain FVIII activity within the target range. rFVIIIFc has a longer half-life than plasma and recombinant FVIII products
[0524] For routine prophylaxis, the recommended regimen is 50 IU/kg every 3-5 days. The dose can be adjusted based on patient response in the range of 25-65 IU/kg.
[0525] For weekly prophylaxis, the recommended dose is 65 IU/kg.
[0526] rFVIIIFc is contraindicated in patients who have manifested severe hypersensitivity reactions, including anaphylaxis, to the product or its components. Severe hypersensitivity reactions were not observed in clinical trials; however, these have been known to occur with use of other factor VIII replacement factors.
[0527] The clinical response to rFVIIIFc can vary. If bleeding is not controlled with the recommended dose, the plasma level of Factor VIII can be determined, and a sufficient dose of rFVIIIFc can be administered to achieve a satisfactory clinical response. If the patient's plasma Factor VIII level fails to increase as expected or if bleeding is not controlled after rFVIIIFc administration, the presence of an inhibitor (neutralizing antibodies) should be suspected, and appropriate testing performed. Patients using rFVIIIFc can be monitored for the development of Factor VIII inhibitors by appropriate clinical observations and laboratory tests known to those of ordinary skill in the art.
[0528] Patient's plasma can be monitored for Factor VIII activity levels, e.g., the one-stage clotting assay to confirm adequate Factor VIII levels have been achieved and maintained, when clinically indicated. Patient's plasma can further be monitored for the development of Factor VIII inhibitors.
Example 9. Population Pharmacokinetic Analysis of Long-Acting Recombinant Factor VIII-Fc Fusion Protein (rFVIIIFc) in Patients with Severe Haemophilia A
[0529] Introduction: In a recently completed Phase 3 clinical study (A-LONG), rFVIIIFc, a recombinant fusion protein composed of a single molecule of B domain deleted human coagulation factor VIII (FVIII) attached to the Fc domain of human immunoglobulin G1 (IgG1), was well-tolerated and effective in the treatment of bleeding, routine prophylaxis, and perioperative management. The duration of activity of rFVIIIFc was prolonged, compared to another recombinant FVIII product (ADVATE.RTM.).
[0530] Objectives: To characterize the activity-time profiles of rFVIIIFc in hemophilia A patients as measured by the one-stage clotting assay by population PK analysis; to identify intrinsic and extrinsic covariates that can affect the variability of rFVIIIFc PK; and to simulate the rFVIIIFc dosing scenarios of interest using the model developed.
[0531] Methods: The modeling dataset included activity-time profiles in a total of 180 subjects (16 from a Phase 1/2a study and 164 from A-LONG) taken over up to 52 weeks of treatment.
[0532] The Phase 1/2a study was an open-label, multicenter, dose-escalation study that included 2 dose levels. A total of 16 subjects received either 25 IU/kg (n=6) or 65 IU/kg (n=10) of ADVATE.RTM. followed 3 or 4 days later, respectively, by an equal dose of rFVIIIFc with an extensive PK sampling scheme following each dose administration.
[0533] A-LONG was an open-label, multinational, multicenter study that included 3 treatment arms.
[0534] Subjects were 12 to 65 years old and weighing between 41 kg and 132 kg. The analysis was done with NONMEM 7 software, and included model building, covariate search, and model qualification steps. The data were analyzed using mixed-effects modeling with maximal likelihood parameter estimation methods. Covariate-parameter relationships were explored for parameters with inter-individual variability (IIV) terms, and model diagnostics were performed to guide model selection. rFVIIIFc dosing regimens of therapeutic interest were simulated using the current model.
[0535] Results: A 2-compartmental model was found to describe adequately the activity of rFVIIIFc, described by the formulas (M), (N), and (O) below:
CL = TVCL [ VWF 118 ] .THETA. 10 ##EQU00008## V 1 = TVV 1 [ WT 73 ] .THETA. 5 [ HCT 45 ] .THETA. 3 ##EQU00008.2## add = STUD .THETA. 5 + ( 1 - STUD ) .THETA. 6 ##EQU00008.3## STUD = { 1 for Phase 1 0 for Phase 3 ##EQU00008.4##
[0536] The tight confidence intervals (Cis) indicate that the parameters are estimated with very good precision (Table 18).
TABLE-US-00018 TABLE 18 rFVIIIFc Population PK parameters and bootstrap- derived 95% Confidence Intervals Population Nonparametric Parameter Symbol Estimate 95% CI Clearance, CL, [dL/h] .THETA.1 1.65 1.57-1.74 Exponent on VWF .THETA.10 -0.343 -0.439--0.247 Central Volume, V1, [dL] .THETA.2 37.5 36.5-38.4 Allometric exponent on V1 .THETA.8 0.382 0.271-0.499 Exponent on HCT .THETA.9 -0.419 -0.656--0.208 Intercompartmental .THETA.3 0.0746 0.0594-0.184 Clearance, Q, [dL/h] Peripheral Volume, V2, .THETA.4 6.92 3.80-13.8 [dL] IIV on CL, [%] .eta.1 24.3 20.5-27.7 IIV on V1, [%] .eta.2 13.4 11.0-15.5 Correlation between IIV on .eta.12 0.548 Not calculated CL and V1 IOV on CL, [%] .eta.3 20.6 16.7-25.1 IOV on V1, [%] .eta.4 12.0 7.46-16.3 Correlation between IOV .eta.34 0.639 Not calculated on CL and V1 Additive error, Phase .THETA.5 0.421 0.172-0.612 1/2A study, [IU/dL] Additive error, Phase 3 .THETA.6 0.208 0.126-0.275 study, [IU/dL] Proportional error, [%] .THETA.7 13.6 12.0-15.3
[0537] The IIV and the residual errors are very low. The goodness of fit diagnostics (FIG. 24) indicate that the model adequately describes the data.
[0538] The population estimate for the clearance (CL) is 1.65 dL/h, and Vss is 44.4 dL. The inter-individual variability (IIV) of CL is moderate (CV=24.3%) and of central volume of distribution (V1) is low (CV=13.4%). The inter-occasional variability (IOV) of both CL and V1 is low (20.6 and 12.0% respectively). The additive residual error is very low (0.208 IU/dL), and so is the proportional residual error (13.6%), approximating the precision of the one-stage clotting assay for FVIII activity. Von Willebrand Factor (VWF) level was identified as the major covariate for CL. Consistent with mechanistic knowledge (Lillicrap 2008), higher levels of VWF yielded lower clearance values, reflecting the protective role that VWF has on FVIII activity. This is reflected in the negative exponent on VWF. Body Weight (BW) and Hematocrit (HCT) were identified as weak covariates on V1. This is the first population PK analysis that systematically describes and characterizes the prolonged activity profile of the long-acting rFVIIIFc.
[0539] Conclusion: The population PK model of rFVIII activity adequately describes the observed activity-time profiles after long term administration. The clearance of rFVIIIFc activity is lower than the clearance reported for ADVATE.RTM., resulting in longer duration of activity. The low IIV underlines the consistency and homogeneity of the activity profiles. The low IOV indicates that rFVIIIFc maintains stable and predictable activity with long term administration over time. The set of covariates identified is physiologically relevant. Therefore, the population model developed can be used to simulate various dosing scenarios in support of dosing regimen selection and other decision making related to rFVIIIFc therapy.
[0540] The model was used to predict the activity time profile following a single dose of rFVIIIFc in patients with severe hemophilia A. In addition the model was used to predict trough activity for three different prophylaxis regimens.
[0541] Table 19 presents the model-predicted steady state peaks and troughs of the rFVIIIFc activity-time profiles with 50 IU/kg dose administered every 3, 4, or 5 days. The simulated steady-state activity profiles are presented in FIG. 25.
TABLE-US-00019 TABLE 19 Predicted Steady-State Peaks and Troughs of rFVIIIFc Activity-Time Profiles with 50 IU/kg Dose Administered Every 3, 4, or 5 Days Dosing Frequency Percentile of Every 3 Days Every 4 Days Every 5 Days Subjects Peak Trough Peak Trough Peak Trough Median (5.sup.th, 95.sup.th 102 5.27 100 2.32 98.5 1.10 prediction (70.4, (0.774, (69.9, (<0.5a, (69.1, (<0.5, interval) 149) 20.4) 141) 11.4) 139) 6.17)
[0542] A dosing regimen of 50 IU/kg every 5 days is predicted to yield troughs above 1 IU/dL in 53.4% of individuals and a dosing regimen of 65 IU/kg administered weekly is predicted to yield troughs above 1 IU/dL in 26.6% of the individuals treated.
[0543] The population PK models for rFVIIIFc and ADVATE.RTM. adequately described the combined activity data from the two clinical studies. The major covariate for rFVIIIFc activity identified by the population PK analysis was VWF level on CL. Weight and hematocrit were identified as minor covariates on the central volume of distribution. The results from the simulations support the dosing recommendations derived from the Phase 3 study results and can be used to aid dosing regimen selection and adjustment.
[0544] Simulation of Regimens for Perioperative Management
[0545] According to the WFH Guidelines, minor surgical procedures may require the attainment of target factor levels of 50 to 80 IU/dL, which can be achieved with a single rFVIIIFc infusion of 25 to 40 IU/kg. If a finer adjustment of the target is desirable, the required rFVIIIFc dose can be determined based on the predicted activity profiles in Table 20, below:
TABLE-US-00020 TABLE 20 Predicted rFVIIIFc Activity-Time Profiles (in IU/dL) After a Single Administration Time (h) Dose EOI 12 24 36 48 72 96 (IU/kg) Median (5.sup.th, 95.sup.th Prediction Interval) 20 38.7 22.7 13.4 7.92 4.72 1.79 0.763 (27.3, 54.5) (13.5, 35.0) (5.79, 23.8) (2.44, 16.7) (1.06, 12.0) (<0.5*-6.52) (<0.5*-3.63) 25 48.4 28.3 16.8 9.90 5.90 2.24 0.953 (34.2, 68.1) (16.9, 43.7) (7.24, 29.8) (3.05, 20.8) (1.32, 15.0) (<0.5*-8.15) (<0.5*-4.54) 30 58.1 34.0 20.2 11.9 7.07 2.69 1.14 (41.0, 81.7) (20.2, 52.5) (8.69, 35.8) (3.66, 25.0) (1.59, 18.0) (<0.5*-9.78) (<0.5*-5.44) 40 77.5 45.3 26.9 15.8 9.43 3.58 1.53 (54.7, 109) (27.0, 70.0) (11.6, 47.7) (4.88, 33.3) (2.11, 24.0) (<0.5*-13.0) (<0.5*-7.26) 50 96.8 56.6 33.6 19.8 11.8 4.48 1.91 (68.3, 136) (33.7, 87.5) (14.5, 59.6) (6.10, 41.7) (2.64, 30.0) (0.615-16.3) (<0.5*-9.07) 65 126 73.6 43.7 25.7 15.3 5.82 2.48 (88.9, 177) (43.8, 114) (18.8, 77.5) (7.94, 54.2) (3.44, 38.9) (0.800-21.2) (<0.5*-11.8) EOI = end of infusion. *BLQ values were set at <0.5.
[0546] For major surgery, WFH recommends a stricter control of Factor VIII dosing, with high activity levels attained in the pre-operative period and during surgery, followed by stepwise decrease of the activity levels during the post-operative period, e.g., within 1 to 3 days, 4 to 6 days, and as long as needed. The population PK model developed can be used as a tool to design such complicated activity profiles.
[0547] An evaluation of the population PK model, similar to external model validation, indicated that the population PK model is in good concordance with the activity observed during the surgical period. The correlation coefficient between the observed and individual predicted activity during surgery is high (R=0.742). The minimal discrepancies between observed and model-predicted activities during surgery are not more than 10% and point to a modest over-prediction associated with peak activity. This may be due to minimal loss of rFVIIIFc during surgery, associated with blood loss. For the surgeries performed in this study, the average blood loss was less than 200 mL.
[0548] Table 21 presents the dosing times, doses, and predicted FVIII activity for a hypothetical perioperative dosing regimen, to achieve levels recommended by WFH Guidelines. The doses, times, and administration as well as the predicted activities are listed for each subsequent dose. All doses after the second one are administered at 24-hour intervals. The resulting activity time profile is presented in FIG. 26.
TABLE-US-00021 TABLE 21 Dosing Times, Doses and Predicted FVIII Activity for a Hypothetical Perioperative Dosing Regimen for rFVIIIFc Dosing Dosing Time Dose Trough (IU/dL) Day (h) (IU/kg) Median (5.sup.th, 95.sup.th Prediction Interval) 0 0 60 0 12 50 67.3 (39.6, 105) 1 24 50 95.4 (50.7, 159) 2 48 50 67.0 (23.6, 140) 3 72 40 57.9 (19.0, 132) 4 96 40 48.1 (15.4, 119) 5 120 40 45.0 (14.8, 112) 6 144 40 44.0 (14.7, 109) 7 168 30 43.6 (14.7, 108) 8 192 30 36.9 (11.9, 95.6) 9 216 30 34.5 (11.3, 88.9) 10 240 30 33.6 (11.2, 85.6) 11 264 30 33.2 (11.2, 83.6) 12 288 30 33.0 (11.2, 82.4) 13 312 30 32.9 (11.1, 81.7)
[0549] Table 21 presents the dosing times, doses and predicted FVIII activity for a simpler hypothetical perioperative dosing regimen. All doses after the fourth dose are administered at 48 h intervals. FIG. 27 shows the predicted FVIII activity for the hypothetical perioperative dosing regimen in Table 22.
TABLE-US-00022 TABLE 22 Dosing times, Doses and Predicted FVIII Activity for a Sample Perioperative Dosing Regimen II Dosing Dosing Time Dose Trough (IU/dL) Day (hr) (IU/kg) Median [5.sup.th, 95.sup.th PI] 0 0 60 0 12 50 68.2 [39.8, 105] 1 24 50 97.7 [50.8, 160] 2 48 50 68.6 [23.7, 144] 4 96 50 22.0 [3.96, 75.1] 6 144 50 16.4 [3.32, 57.6] 8 192 50 15.6 [3.25, 52.7] 10 240 50 15.4 [3.23, 51.0] 12 288 50 15.3 [3.22, 50.4]
[0550] The model was used to predict FVIII activity in patients during the post-operative period based on subjects' presurgery baseline PK. In the Phase 3 study, there were 13 subjects who underwent major and minor surgeries and also had their rFVIIIFc activity measured during the perioperative period. These subjects had variable dosing regimens and time intervals in perioperative management. To check whether the observed FVIII activity during this period (coded as OCC=0 in the database) are in agreement with the population PK model, an evaluation, similar to external model validation, was performed.
[0551] Predicted FVIII activity was largely consistent with observed FVIII activity. FIG. 28 is a representative plot comparing the predicted and observed FVIII activities within the first 21 days after the first rFVIIIFc surgical dose (n=13; 9 major surgeries, 4 minor surgeries). There was good correlation between the observed FVIII activity data and that predicted by the PK model (relative prediction error 95% CI). The resulting Goodness of Fit (observed DV, versus individual predicted, IPRED) diagnostics, shown in FIG. 28, indicates that the population PK model is in concordance with the activity observed during the surgical period. The correlation coefficient between the observed and individual predicted activity is high (R=0.742).
[0552] The nonparametric fit of the data, represented by the lower line in FIG. 28, diverges only slightly from the identity line (upper line). This divergence is not more than 10% and points to a modest over-prediction in the region of high activity. This may be due to minimal loss of rFVIIIFc during surgery, associated with blood loss. For the surgeries performed in this study, the average blood loss was less than 200 mL. These results indicate that the surgical procedures that have been studied in the Phase 3 study had no significant impact on the PK properties of rFVIIIFc.
[0553] In conclusion, it is feasible to develop a general dosing guidance to achieve target FVIII levels recommended for perioperative management in patients with haemophilia A using a population PK model.
Example 10. Use of the Population Pharmacokinetic Model of rFVIIIFc to Simulate or Estimate Individualized and Median Patient Treatment
[0554] As is discussed in Example 9 or 11 or 16, the rFVIIIFc population model that has now been developed can be used to simulate (estimate) various dosing scenarios in support of dosing regimen selection and other decision making related to rFVIIIFc therapy.
[0555] For example, individualized patient treatment, e.g., pharmacokinetics (PK) and dosing regimens, can be selected using Bayesian estimation (or similar machine learning algorithm) based on the population pharmacokinetic (popPK) model described in Example 9 or 11 or 16, (e.g., Table 18, 24, 25, or 33). In this way, one can determine alternative prophylactic dosing regimens and optimized dosing regimens for pen-operative management that have not previously been studied in the A-LONG trials. Alternatively, the selected dosing regimen is based on population PK (median PK) rather than making an individualized selection.
[0556] In some embodiments, the rFVIIIFc popPK model of Example 9 or 11 or 16 (e.g., Table 18, 24, 25, or 33) is used without the Bayesian or similar machine learning algorithm.
[0557] In some embodiments of this aspect of the invention, the method is carried out on a computer-based system, e.g., a server, a desk top computer, a lap top computer, a tablet, a hand held device, or a smart phone. In some embodiments, the computer-based system is a computer application. The computer-based system includes a storage medium for the rFVIIIFc popPK model discussed in Example 9 or 11 or 16, e.g., the parameters of Table 18, 24, 25, or 33. In some embodiments, the storage medium can also contain a Bayesian estimating program, e.g., NONMEM or Phoenix NLME. E.g., Example 9 or 11 or 16; Kiang et al., Clin. Pharmacokinet 51:515-525 (2012).
[0558] In some embodiments, the system comprises two or more computer-based systems. In some embodiments, the user can input information into a first computer-based system that communicates with a second computer-based system, and the second computer-based system carries out calculations and communicates output information to the first computer-based system. This output information can include recommendations about individualized or non-individualized dosing regimens.
[0559] In some embodiments, the user inputs information into the system and the system calculates and outputs one or more PK or dosing regimens. In some embodiments, the system uses the received information to calculate and output individualized or median PK information. In some embodiments, the system calculates individualized dosing or interval information.
[0560] Information that can be input by a user and received by the system includes patient information and desired treatment outcome information. Based on the type and value of the received information, the computer-based system calculates output information based on the rFVIIIFc popPK model and optional machine learning algorithm on the storage medium.
[0561] Patient information includes, e.g., age, Von Willebrand Factor (VWF) level, hematocrit (HCT), body weight (BW), diagnostic (baseline) FVIII level, PK determinations, time of PK sampling, dosing history if PK samples were taken from multiple doses, actual dose, FVIII activity level, etc.
[0562] Desired treatment outcome information includes desired PK or desired regimen outcome, e.g., desired rise in plasma FVIII activity level following dose, desired dosing interval, and desired dose.
[0563] Based on the information that was input and received by the system, the system can output various information, e.g., PK curve, PK parameter such as incremental recovery (Cmax/dose), mean residence time, terminal t1/2, clearance, Vss, AUC/dose, doses and associated troughs, and intervals and associated troughs.
[0564] For example, for assessing individualized patient PK, the system can recommend that the user input 2-3 optimized PK sampling time points. In this case, system output can include PK curve and one or more selected PK parameters, e.g., incremental recovery (Cmax/Dose), mean residence time, terminal t1/2, clearance, Vss, AUC, and time to 1 or X %, etc. E.g., FIG. 13.
[0565] As additional examples, to select an individualized dosing regimen using the output individual PK parameters discussed in the preceding paragraph, (i) the dose selected for acute treatment can be based on user input of the desired rise in plasma FVIII activity level following the dose, (ii) the dose selected for prophylaxis can be based on user input of the desired dosing interval, or (iii) the selected interval for prophylaxis can be based on user input for the desired dose. In the first case, the system can output the dose (IU) based in the patient's incremental recovery. E.g., FIG. 14. In the second case, system output can be a table of doses and associated troughs, e.g., x IU/kg, 1% trough, y IU/kg, 2% trough, etc. E.g., FIG. 15, top. In the third case, system output can be a table of intervals and associated troughs, e.g., x days, 1% trough, y IU/kg, 2% trough, etc., E.g., FIG. 15, bottom.
[0566] The user may wish to use the system without inputting any individualized PK data. In this case, the dosing output would be based on the population median rather than being individualized for the particular patient. E.g., FIG. 29. In this way, the user inputs, e.g., body weight and age, and (i) the desired rise in plasma FVIII activity level following the dose, (ii) the desired dose interval for prophylaxis, or (iii) the desired dose for prophylaxis. In the first case, the system can output the dose. In the second case, the system can output the dose and associated trough. E.g., Table 20 In the third case, the system can output the interval and associated trough. E.g., Table 19.
[0567] Age can be input to determine if the system is suitable for the patient because the current version of the popPK model was built for patients 12 years and older.
[0568] In some embodiments, the system is compliant with patient privacy laws. In some embodiments, the system is encrypted, e.g., with SSL. In some embodiments, input patient information is made anonymous.
[0569] In some embodiments, the system includes a user help function.
[0570] The user can be, e.g., a physician, a nurse, or another healthcare practitioner.
[0571] In some embodiments, the method further includes selecting a dosing regimen based on the system's output information and administering rFVIIIFc to the patient according to the selected regimen.
Example 11. Population Pharmacokinetics of Recombinant Factor VIII:Fc
[0572] Abstract
[0573] Population pharmacokinetics (PK) of FVIII activity-time profiles following recombinant factor VIII Fc fusion protein (rFVIIIFc) and recombinant factor VIII (rFVIII) dosing were evaluated in treated patients with severe hemophilia A (from two clinical trials). Potential covariates were determined. A 2-compartment model adequately described the PK of both compounds. Von Willebrand Factor (vWF) concentration was the major covariate for rFVIIIFc clearance, reflecting its protective role in FVIII activity clearance. The effect of body weight and hematocrit on the central volume of distribution (V1) of rFVIIIFc was minor. The population PK for rFVIII demonstrated similar behavior to that in the published literature. The results of these analyses confirmed that rFVIIIFc clearance (1.65 dL/h) is much lower than that of rFVIII (2.53 dL/h), while V.sub.1 at steady state was similar. The strong positive correlations between the PK parameters of rFVIIIFc and rFVIII suggest that individuals who have high time-related PK characteristics with rFVIII are likely to have comparable characteristics with rFVIIIFc. Steady-state activity-time profiles for selected rFVIIIFc dosing regimens were simulated accounting for model prediction uncertainty. These population PK analyses and simulations provide a comprehensive characterization of the PK of rFVIIIFc and rFVIII and may be useful for designing dosing regimens.
Introduction
[0574] Hemophilia A is an X-chromosome-linked coagulation disorder that primarily affects males, and occurs in approximately 1-2 per 10,000 live births. It is caused by mutations and/or deletions in the F8 gene, resulting in a deficiency of factor VIII (FVIII) activity. Severe hemophilia A is defined as a coagulation activity of FVIII in plasma (FVIII:C) level <1% (<1 IU/dL), and individuals with this severe form of the disease experience recurrent spontaneous bleeding, primarily into the muscles and joints, leading to joint damage and severe disability. This is associated with a negative impact on psychosocial well-being and quality of life.
[0575] Modern FVIII replacement therapy for hemophilia A relies on the infusion of specific concentrates to substitute the deficient or inactive endogenous FVIII. Such infusions are performed either episodically (e.g., for on-demand treatment of bleeding or before/during and after surgery) or prophylactically. Target factor activity levels may vary depending on the dosing paradigm; for acute bleeding such as during major surgeries, this may be as high as 80 to 100 IU/dL, while the goal for prophylaxis is to maintain trough activity levels >1 IU/dL.
[0576] Recombinant factor VIII Fc fusion protein (rFVIIIFc) is a novel protein composed of a single B-domain-deleted human coagulation FVIII molecule attached to the Fc domain of human immunoglobulin G1 (IgG1), designed to offer a longer circulating half-life (t.sub.1/2) than currently available FVIII products. Clinical studies have confirmed this increase in t112 relative to recombinant FVIII (rFVIII) and demonstrated the safety and efficacy of rFVIIIFc for the prevention and treatment of bleeding episodes in patients with hemophilia A.
[0577] The quantitative characterization of FVIII activity-time profiles (referred to as pharmacokinetics [PK]) provides critical information for determining dose levels and dosing frequencies to achieve target therapeutic levels. Traditionally, the PK of most marketed agents have been characterized by non-compartmental or compartmental 2-stage methods. More recently, a number of population PK models and model implementations for several FVIII products have been published.
[0578] The objective of this example is to present the development of a population PK model based on rFVIIIFc activity data in individuals with severe hemophilia. The PK parameters of the model were estimated and significant determinants (covariates) of variability in rFVIIIFc PK in subjects with hemophilia A were identified. The population PK model was then used to simulate rFVIIIFc dosing regimens of interest. A population PK model for antihemophilic factor ([recombinant], plasma albumin-free method), a rFVIII product used as comparator in the clinical studies performed, was also developed.
[0579] Methods: Clinical Studies
[0580] The clinical data that served as a basis for the population PK model development originated from two studies--a phase 1/2a (n=16) and a phase 3 study (n=164). These protocols were approved by local institutional review boards/ethics committees, and the studies were conducted in accordance with the International Conference on Harmonization guidelines for Good Clinical Practice.
[0581] The Phase 1/2a study was an open-label, crossover, dose-escalation, multicenter study to determine the safety, tolerability, and PK of a single intravenous (IV) injection of rFVIIIFc in previously treated patients with severe hemophilia A. (Powell J S, Josephson N. c, Quon D, et al, Safety and prolonged activity of recombinant factor VIII Fc fusion protein in hemophilia A patients. Blood, 2012, 119 (13), 3031-7). The study included two cohorts dosed at the 25 IU/kg (Cohort A) and 65 IU/kg (Cohort B) level. After screening and a minimum of 4 days initial washout period, subjects from both cohorts received a single 25 IU/kg (Cohort A) or 65 IU/kg (Cohort B) dose of rFVIII followed by a 3-day (Cohort A) or 4-day (Cohort B) blood sampling regimen for PK assessment (see upper panel of Table 23 for the Phase 1/2a sampling schedule). These patients then received a 25 IU/kg (Cohort A) or 65 IU/kg (Cohort B) single dose of rFVIIIFc followed by a 7-day (Cohort A) or 10-day (Cohort B) blood sampling regimen for PK assessment.
TABLE-US-00023 TABLE 23 Intensive sampling schedules in the Phase 1/2a and Phase 3 studies Study Arm/Cohort Agent Dose Sampling Schedule Phase Cohort A rFVIII 25 IU/kg 0, 0.167, 0.5, 1, 3, 6, 9, 1/2a 24, 48, 72 h rFVIIIFc 25 IU/kg 0, 0.167, 0.5, 1, 3, 6, 9, 24, 48, 72, 96, 120, 168 h Cohort B rFVIII 65 IU/kg 0, 0.167, 0.5, 1, 3, 6, 9, 24, 48, 72, 96 h rFVIIIFc 65 IU/kg 0, 0.167, 0.5, 1, 3, 6, 9, 24, 48, 72, 96, 120, 168, 192, 216, 240 h Phase Arm 1 PK rFVIII 50 IU/kg 0, 0.5, 1, 6, 24, 48, 72 h 3 Arm 1 PK rFVIIIFc 50 IU/kg 0, 0.5, 1, 6, 24, 72, 96 and 120 h Arm 1 rFVIIIFc 50 IU/kg 0, 0.5, 3, 72, 96 h Non-PK Arm 2 rFVIIIFc 65 IU/kg 0, 0.5, 3, 72, 96 h Arm 3 rFVIIIFc 50 IU/kg 0, 0.5, 3, 72, 96 h
[0582] The Phase 3 study was an open-label, multinational, multicenter study to evaluate the safety, PK, and efficacy of rFVIIIFc administered as an IV injection to subjects with severe hemophilia A, at least 12 years of age (Mahlangu J. et al. Phase 3 study of recombinant factor VIII Fc fusion protein in haemophilia A, Lancet, submitted 2013). At study start, all subjects underwent a washout of FVIII products for 72-96 hours followed by an initial PK sampling. The study comprises 3 treatment arms:
[0583] In Arm 1 (n=118) patients received individualized prophylaxis regimen, consisting of two subgroups--a Sequential PK Subgroup and a Non-sequential PK Subgroup. Subjects assigned to the Arm 1 Sequential PK subgroup received a single dose of rFVIII 50 IU/kg on Day 0 followed by semi-sparse blood sampling for PK assessment over a 72-hour period (7 timepoints) according to the schedules shown in Table 23 (lower panel). Following a washout period, these subjects then received a single dose of rFVIIIFc 50 IU/kg followed by a semi-sparse PK sampling at 8 timepoints over a 120-hour period. PK profiling of rFVIIIFc 50 IU/kg was reassessed 12-24 weeks later. Subjects in Arm 1 non-sequential PK subgroup received a single rFVIIIFc dose of 50 IU/kg of rFVIIIFc, on Day 0 followed by a semi-sparse PK blood sampling performed at 5 timepoints. Upon completion of the rFVIIIFc PK assessment, an individualized prophylaxis regimen was established for each individual in Arm 1 (both subgroups) based on their PK, in which the dose (25-65 IU/kg) and dosing interval (3-5 days) were determined to maintain a trough level of 1% to 3% rFVIIIFc activity.
[0584] In Arm 2 (n=24) patients received a weekly prophylaxis regimen. Subjects received a single rFVIIIFc dose of 65 IU/kg of rFVIIIFc on Day 0 followed by a semi-sparse PK blood sampling performed at 5 timepoints. After the PK assessment, subjects in Arm 2 were administered a fixed weekly prophylaxis rFVIIIFc dose of 65 IU/kg.
[0585] In Arm 3 (N=23) patients received episodic dosing regimen with a single rFVIIIFc dose of 50 IU/kg of rFVIIIFc on Day 0 followed by a semi-sparse PK blood sampling performed at 5 timepoints. During the study, subjects in Arm 3 were treated episodically at rFVIIIFc doses of 10-50 IU/kg depending on the severity of the bleed.
[0586] In addition to the PK profiling, peak and trough measurements were carried out periodically, at nominal times spread over the whole course of study participation (e.g., peak/trough collections at week 7, 14, 28, 38, 52, etc.) for subjects in Arms 1 and 2.
[0587] Assay Methodology
[0588] For the Phase 1/2a study, the FVIII activity was measured by one-stage clotting (activated partial thromboplastin time [aPTT]) assay with a Siemens BCS-XP analyzer (Siemens AG, Erlangen, Germany) with the use of commercial reagents (Dade Actin FSL; Siemens Healthcare Diagnostics, Inc., Newark, Del., USA) and calibration against a normal reference plasma (CRYOCHECK.TM.; Precision Biologics, Dartmouth, Nova Scotia, Canada) traceable to the World Health Organization (WHO) Fifth International Standard for human plasma. In addition, FVIII activity was also measured by a chromogenic substrate assay with the use of a commercially available kit (Aniara BIOPHEN.TM. FVIII:C; Aniara, West Chester, Ohio, USA) that complies with European Pharmacopoeia recommendations. This assay was calibrated against normal human reference plasma (ORKE45; Instrumentation Laboratory, Bedford, Mass., USA), which also had a potency assigned against the human plasma standard from the WHO Fifth International Standard. The lower limits of quantification (LLOQ) for the aPTT and chromogenic assays were 0.5 IU/dL and 0.4 IU/dL, respectively. In the phase 3 study, FVIII activity was measured using the one-stage aPTT assay as outlined above.
[0589] Data Assembly and Manipulation
[0590] Datasets generated from both studies were merged together to form the population PK analysis dataset. An occasion (OCC) variable was added to the rFVIIIFc dataset to enable the inclusion of inter-occasional variability (IOV) in the models. Occasions are defined within each individual, as clusters of observations, separated from previous observations by at least 1 week of dosing. Occasions 1 and 2 are reserved for the Baseline (first) and Repeat (second) intensive PK sampling period. The rest of the occasions are allocated to trough and peak measurements, and as such, represent sparse observation periods.
[0591] Some missing covariate values were imputed by substituting with a typical (median) value. Where missing covariate values could not be imputed, these were replaced by negative values and ignored. Where only a fraction of the covariate values for a given individual were missing, they were imputed from the remaining values by a LOCF (Last Observation Carried Forward) technique--this was the case for von Willebrand Factor (VWF) antigen levels, IgG1 levels (IGG1), and hematocrit (HCT).
[0592] Baseline Correction and Residual Decay
[0593] Activity levels observed before administration of a rFVIII product represent a combination of endogenous activity (baseline) and residual activity from pre-study drug. To account for that, baseline and residual drug corrections were performed on the observed FVIII activity results for both rFVIIIFc and rFVIII. Similar corrections are typical for PK analyses of other FVIII and factor IX products (Bjorkman S, C. M., Berntop E, Pharmacokinetics of Factor IX in patients with hemophilia B. Eur J Clin Pharmacol, 1994. 46: p. 325-332; Carlsson M, B. S., Berntop E, Multidose pharmacokinetics of factor IX: Implications for dosing in prophylaxis. Hemophilia, 1998. 4: p. 83-88; Bjorkman S, S. A., Berntop E, Pharmacokinetics of recombinant factor IX in relation to age of the patients: Implications for dosing in prophylaxis. Hemophilia, 2001. 7: p. 133-139; Bjorkman S, O. M., Spotts G, et al., Population pharmacokinetics of recombinant factor VIII--the relationships of pharmacokinetics to age and body weight. Blood, 2012. 119: p. 612-618 ("Bjorkman 2012 A"); Bjorkman S, A. V., Population pharmacokinetics of plasma-derived factor IX in adult patients with hemophilia B: Implications for dosing in prophylaxis. Eur J Clin Pharmacol, 2012. 68(6): p. 969-77). These corrected activity-time profiles were included in the population PK datasets. It should be noted that only the first (baseline) rFVIII and rFVIIIFc activity-time profiles were corrected for residual decay.
[0594] Residual decay was performed using the terminal half-life (t.sub.1/2) obtained from noncompartmental analysis (NCA) of the raw, observed activity data. For the Arm 1 PK subgroup, rFVIII and Baseline rFVIIIFc PK profiles were decayed using the respective subject's rFVIII t.sub.1/2. For the Arm 1 non PK subgroup, Arm 2, and Arm 3, rFVIIIFc PK profiles were decayed using the average rFVIII t.sub.1/1 obtained from the Arm 1 PK subgroup.
[0595] The pre-dose FVIII activity levels are a combination of endogenous activity (baseline) and the residual activity from previous pre-study drug administration(s). Therefore, the baseline and residual drug corrections were performed on the observed FVIII activity results prior to data analysis.
[0596] The baseline- and residual-corrected activity (FVIII:Ccorr) is calculated from the actual observed activity (FVIII:Cobs) based on the formula given below:
FVIII:Ccorr=FVIII:Cobs-Baseline Activity-Residual decay (Eq. X)
[0597] where the Residual decay=(Pre-dose Activity-Baseline Activity)*e.sup.-.lamda.*time
[0598] Residual decay, to account for activity as a result of previous administration of a FVIII product, was performed using the terminal first-order decay rate (.lamda.) obtained from noncompartmental analysis (NCA) of the raw, observed activity data. The endogenous or baseline activity was set to zero for all subjects in the above equation.
[0599] For the Arm 1 sequential PK subgroup, the FVIII activities following Advate and Baseline rFVIIIFc PK administrations were decayed using the respective subject's Advate .lamda.. The FVIII activity-time profiles resulting from rFVIIIFc infusions for the subjects in Arm 1 non-sequential PK subgroup, Arm 2, and Arm 3 were decayed using the average Advate .lamda. obtained from the Arm 1 sequential PK subgroup.
[0600] Population Analysis Methodology
[0601] Two population PK models were developed independently of each other--one for rFVIIIFc, based on the rFVIIIFc data, and one for rFVIII, based on the rFVIII data alone.
[0602] Mixed-effects modeling with maximum likelihood parameter estimation methods were used to evaluate the population characteristics of rFVIIIFc and rFVIII in hemophilia A patients. For the description of random inter-individual variability (IIV), a log-normal distribution of the random effects, with a block covariance matrix was used. Various random residual error configurations were tested by combinations of additive and proportional variance terms. Inclusion of IOV to account for the change in the system properties with time was evaluated. First order conditional estimation with interaction (FOCEI) method was implemented for parameter estimation.
[0603] Diagnostic plots, minimum value of the objective function (OFV), and the evaluation of shrinkage were used to guide model building and assess goodness-of-fit. The Likelihood Ratio Test was used to compare hierarchical models.
[0604] The base pharmacokinetic model was developed by exploring typical structural models, including one- and two-compartment linear models. Models were compared by goodness-of-fit diagnostics including the Likelihood Ratio Test (significance level of 0.01, change in objective function value (OFV)=6.64 for 1 degree of freedom [df]), diagnostic plots, and estimates and standard errors of model parameters. The statistical model was built by testing and discriminating between various IIV and IOV structures and between different combinations of additive and proportional residual error terms. Candidate models were run from a number (usually 25-50) of different randomly generated initial estimates to assess the model stability and convergence.
[0605] Weight (WT) and Study (STUD), although technically assumed covariates, are sometimes considered as intrinsic to the basic model as their inclusion can be postulated a priori. For this reason the base models developed included these covariates.
[0606] The following factors were considered as potential covariates: height, age, race, blood type, hematocrit, von Willebrand factor antigen levels, IgG1 levels, albumin levels, non-neutralizing antibody (ADA) presence, HCV status, HIV status.
[0607] The continuous covariates were centered around a standard value--usually the median of the study population. For the forward covariate inclusion procedure, the Likelihood Ratio Test was used to compare hierarchical models with a significance level of 0.01. Decrease in the respective IIV term and other Goodness of Fit measures were also considered for inclusion. Once the full population covariate model was constructed a stepwise backwards deletion method with a significance level of 0.001 (change in objective function value=10.8 for 1 degree of freedom) was used to determine the final model. In all cases, physiological relevance of the covariates was considered before accepting a covariate.
[0608] A bootstrap procedure (nominally 1000 bootstraps), implemented by the bootstrap function of the Perl speaks NONMEN software package (PsN) was used to characterize the uncertainty in the model parameter estimates. Nonparametric 95% confidence intervals (CI) of all parameters were constructed based on the bootstrap results.
[0609] The predictive ability of the final model(s) was evaluated using simulation in a visual predictive check (vpc) using the vpc function of PsN. Outliers with |CWRES (Conditional Weighted RESiduals)|>5 were evaluated for impact on the qualified models by sensitivity analysis. Atypical drug activity data (such as very low or very high activity levels, or data not compliant with the trough-dose-peak sequence) were excluded from the analysis if no apparent explanation for these observations was provided. Activity data were excluded from the analysis if corresponding dosing or sampling times were missing or could not be reconstructed.
[0610] In order to evaluate the impact of values below the level of quantitation (BLQ), the analysis was performed using various approaches, either (i) excluding the BLQ values or (ii) using method(s) outlined in the literature to handle BLQ values (Beal, S., Ways to fit a PK model with some data below the quantification limit. J Pharmacokin Pharmacodyn, 2001. 28: p. 481-504; Jae Eun Ahn, M. O. K., Adrian Dunne and Thomas M. Ludden, Likelihood based approaches to handling data below the quantification limit using NONMEM VI J Pharmacokin Pharmacodyn, 2008. 35(4): p. 401-21).
[0611] Simulations
[0612] A number of rFVIIIFc dosing regimens were simulated. During the simulations, the activity-time profiles at Steady State (SS) for 2000 individuals were generated. Weight characteristics of the population simulated were derived from the Phase 3 study data. Where IOV was part of the model, the SS dosing interval or period simulated was set up as a single occasion. All dosing regimens were simulated using the same value of the random seed(s) to ensure comparability of the results. Simulation results are represented as the median as well as the 5th, 25th, 75th, and 95th percentiles activity-time curves.
[0613] Two types of simulation exercises were performed. In the first type, simulations were performed with models without including uncertainty in the model parameters. These simulations were used to illustrate the dosing regimen of interest and to derive parameters of therapeutic relevance (such as the percentage of individuals with FVIII activity levels >1 IU/dL). In the second type of simulation, univariate uncertainty distributions were reconstructed from the bootstrap results and used to explore the impact of modeling uncertainties on model predictions. The uncertainty distributions were sampled 1,000 times and 2,000 individuals were simulated with each set of parameter values. The 90% CIs of the activity percentile profiles were calculated from the simulated curves.
[0614] Software and Hardware
[0615] NONMEM (ICON plc, Dublin, Ireland, versions 7.1.2, and 7.2) was used for population PK analysis with Intel Fortran compiler (Intel Corporation, Santa Clara, Calif., version 11.1.048 and version 12.1).
[0616] Most of the model development was done on a workstation with a Quad Xeon Intel Processor and 8 GB of RAM. The computer intensive procedures such as bootstraps, visual predictive checks, etc. were run with up to 24 parallel cores on an HP 20-node cluster, each node with 2 quad-core Intel Xeon E5630 (160 cores in total) at 2.53 GHz and 24 to 60 GB of RAM.
[0617] Results: Base Model for rFVIIIFc
[0618] The base model for rFVIIIFc is a two compartment model with covariate WT on the central volume of distribution (V.sub.1); IOV, and BLOCK(2) IIV on clearance (CL) and V.sub.1; common proportional error, and separate additive residual error for the Phase 1/2a and Phase 3 data (TVV.sub.1: typical apparent value for central volume of distribution):
V 1 = TVV 1 [ WT 73 ] .THETA. 8 ( P ) add = STUD .THETA. 5 + ( 1 - STUD ) .THETA. 6 , where STUD = { 1 for Phase 1 0 for Phase 3 . ( Q ) ##EQU00009## [0619] The population parameters and the bootstrap-derived nonparametric 95% CIs are given in Table 24:
TABLE-US-00024 [0619] TABLE 24 Population parameters of the base model for rFVIIIFc Method BLQ values commented out M3 Method Population Nonparametric Population Parameter Symbol Estimate 95% CI Estimate Clearance, CL, [dL/h] .THETA..sub.1 1.63 1.54-1.73 1.72 Central Volume, V.sub.1, [dL] .THETA..sub.2 37.9 36.9-38.8 36.4 Allometric exponent on V.sub.1 .THETA..sub.8 0.448 0.341-0.552 0.498 Intercompartmental Clearance, Q, [dL/h] .THETA..sub.3 0.0742 0.0581-0.187 1.15 Peripheral Volume, V.sub.2, [dL] .THETA..sub.4 6.77 3.83-12.7 5.79 IIV on CL, [%] .eta..sub.1 29.3 24.9-33.5 31.1 IIV on V1, [%] .eta..sub.2 13.5 11.3-15.5 13.8 Correlation between IIV on CL and V.sub.1 .eta..sub.12 0.464 N.C. .sup.a 0.461 IOV on CL, [%] .eta..sub.3 20.7 16.5-25.1 21.9 IOV on V.sub.1, [%] .eta..sub.4 12.2 7.81-16.2 10.5 Correlation between IOV on CL and V.sub.1 .eta..sub.34 0.643 N.C. .sup.b 0.558 Additive error, Phase 1/2a study, [IU/dL] .THETA..sub.5 0.419 0.150-0.634 0.469 Additive error, Phase 3 study, [IU/dL] .THETA..sub.6 0.207 0.112-0.270 0.264 Proportional error, [%] .THETA..sub.7 13.7 12.1-15.5 14.6 .sup.a Nonparametric 95% CI of 0.00972-0.0281 for a population mean of the covariance .omega. 12 of 0.0184 .sup.b Nonparametric 95% CI of 0.00637-0.0310 for a population mean of the covariance .omega.34 of 0.0163
[0620] The observation records containing BLQ activity values were excluded while developing the base model. In order to assess the influence of the BLQ values on the population estimates, these data records were re-introduced and the estimation was re-run using the M3 and M4 methods. Those runs experienced some instability in both the estimation and covariance steps; M4 was more unstable than M3. When an Importance Sampling estimation step (METHOD=IMP) was implemented following the FOCEI estimation, both the minimization and covariance step converged with the M3 method. Despite the inherent estimation instability with the inclusion of the BLQ values, whenever the estimation converged, the parameter estimates were very close to the estimates obtained in the same model that excluded BLQ values (see Table 24, last column).
[0621] Covariate Model Building and Final Model for rFVIIIFc
[0622] As a result of the forward covariate inclusion, the full covariate model was identified, with VWF, AGE, and Hepatitis C virus (HCV, binary) as covariates on CL, and hematocrit (HCT), in addition to the base model WT and STUD as covariates on the central volume of distribution (V.sub.1).
[0623] According to the accepted mechanistic hypothesis about the influence of antibodies on protein kinetics, the presence of antibodies usually increases the clearance of the target proteins by speeding up their rate of elimination. The incidence of antibodies in the dataset was low--5 individuals had antibodies at baseline, while 6 individuals acquired antibodies during the course of the clinical trial. It should be noted also that the antibody detection was transient within the same individual.
[0624] Testing the antibody presence (ADA) as a binary covariate on V.sub.1 unexpectedly led to a statistically significant drop in the OFV, while the influence on ADA on clearance was negligible. A closer inspection of the model revealed that although the drop in the OFV was statistically significant, the IIV term on V.sub.1 decreased only marginally (from 0.018 in to 0.0173) following the covariate inclusion. The V.sub.1 in the presence of antibodies increased by 18%, which is unlikely to be clinically meaningful. A possible explanation for the assignment of the ADA covariate to the V.sub.1, rather than to the clearance, is the dominant influence of those individuals who are antibody-positive at baseline over the individuals who acquire antibodies during therapy.
[0625] Due to the small number of those individuals as well as the transient character of the antibody response, the antibody covariate (ADA) on V.sub.1 was rejected. Thus, no definitive effect of the presence of non-neutralizing antibodies on the PK of rFVIIIFc activity could be detected by this analysis.
[0626] As a result of the backward elimination procedure, STUD covariate on V.sub.1 as well as HCV and AGE covariates on clearance were removed from the full covariate model without a significant impact on the OFV. The removal of the HCT on V.sub.1, however, led to a significant increase in the OFV, therefore HCT was retained.
[0627] The final population PK model for rFVIIIFc was a two compartment model with covariates VWF on CL, WT and HCT on V.sub.1, IOV (7 occasions), BLOCK(2) variance-covariance matrix on CL and V.sub.1, and separate additive residual error for the Phase 1/2a and Phase 3 with a common proportional error term, as follows (TVCL: typical apparent value for clearance):
CL = TVCL [ VWF 118 ] .THETA. 10 ( R ) V 1 = TVV 1 [ WT 73 ] .THETA. 8 [ HCT 45 ] .THETA. 9 ( S ) add = STUD .THETA. 5 + ( 1 - STUD ) .THETA. 6 , where STUD = { 1 for Phase 1 0 for Phase 3 ( T ) ##EQU00010##
[0628] The population parameters of the final model and the bootstrap-derived nonparametric 95% CIs are given in Table 25:
TABLE-US-00025 TABLE 25 Population parameters of the final model for rFVIIIFc Method BLQ values commented out M3 Method Population Nonparametric Population Parameter Symbol Estimate 95% CI Estimate Clearance, CL, [dL/h] .THETA..sub.1 1.65 1.57 to 1.74 1.73 Exponent on VWF .THETA..sub.10 -0.343 -0.439 to -0.247 -0.391 Central Volume, V.sub.1, [dL] .THETA..sub.2 37.5 36.5 to 38.4 36.8 Allometric exponent on V.sub.1 .THETA..sub.8 0.382 0.271 to 0.499 0.423 Exponent on HCT .THETA..sub.9 -0.419 -0.656 to -0.208 -0.412 Intercompartmental Clearance, Q, [dL/h] .THETA..sub.3 0.0746 0.0594 to 0.184 0.279 Peripheral Volume, V.sub.2, [dL] .THETA..sub.4 6.92 3.80 to 13.8 4.09 IIV on CL, [%] .eta..sub.1 24.3 20.5 to 27.7 25.1 IIV on V.sub.1, [%] .eta..sub.2 13.4 11.0 to 15.5 13.6 Correlation between IIV on CL and V.sub.1 .eta..sub.12 0.548 N.C. .sup.a 0.563 IOV on CL, [%] .eta..sub.3 20.6 16.7 to 25.1 22.0 IOV on V.sub.1, [%] .eta..sub.4 12.0 7.46 to 16.3 9.27 Correlation between IOV on CL and V.sub.1 .eta..sub.34 0.639 N.C. .sup.b 0.526 Additive error, Phase 1/2a study, [IU/dL] .THETA..sub.5 0.421 0.172 to 0.612 0.416 Additive error, Phase 3 study, [IU/dL] .THETA..sub.6 0.208 0.126 to 0.275 0.240 Proportional error, [%] .THETA..sub.7 13.6 12.0 to 15.3 15.4 .sup.b Nonparametric 95% CI of 0.00956-0.0264 for a population mean of the covariance .omega.12 of 0.0179 .sup.c Nonparametric 95% CI of 0.00579-0.0312 for a population mean of the covariance .omega. 34 of 0.0158
[0629] As with the base model case, the influence of the BLQ values on the population estimates was assessed by running the M3 method on the final model with the BLQ values re-included in the dataset. The run completed with a successful minimization, but the covariance step was aborted, confirming the inherent instability introduced by the inclusion of BLQ values. There are minimal differences between the two sets of parameter estimates (Table 25); all M3 method parameters, except the intercompartmental clearance and the proportional error terms, lie within the nonparametric 95% CI identified for the final model.
[0630] The Goodness of Fit (GoF) diagnostics of the final model are shown in FIG. 30A-D; the results of a Visual Predictive Check are presented in FIG. 31A-F.
[0631] The IIV of the activity was low to moderate. Typically, as with other FVIII products (Bjorkman S, Blanchette V S, Fischer K, et al., J Thromb Haemost., 8(4):730-736 (2010); Bjorkman S, Oh M, Spotts G, et al., Blood, 119(2):612-618 (2010)) the CL had higher IIV while the IIV of the volume of distribution, characterized by a coefficient of variation (CV) of 13.4%, was very low. Similarly, the IOV was low, which was in line with observations from other FVIII products (Bjorkman S, Blanchette V S, Fischer K, et al., J Thromb Haemost., 8(4):730-736 (2010); Bjorkman S, Oh M, Spotts G, et al., Blood, 119(2):612-618 (2010)). As with the IIV, the IOV of the clearance was higher than the IOV of the volume of distribution.
[0632] The GoF plots indicate that the model fitted the experimental data very well, specifically at the lower end of the activities (which is the range of interest with respect to therapeutic effects). There were no systematic deviations or shapes detectable in the residual plots and no notable deviations from the symmetry distribution assumption for most of the exponential inter-individual variability (ETA) terms.
[0633] The residual error values for both the base and the final models were very low. The additive error was less than the LLOQ. The proportional error was of the same magnitude as the precision of the assay (CV <10%). This showed that the final model had almost completely extracted the information contained in the data; the unexplained variance was almost exclusively due to the inherent activity assay variability.
[0634] The ETA shrinkage of the IIV terms was moderate, whereas the ETA shrinkage on the IOV terms was higher (>25%) and was especially high for occasions containing sparse data.
[0635] The results from both the base and the final models indicate that the activity of rFVIIIFc does not display strong dependence on weight. CL did not accept a WT covariate, while the retained WT covariate on the V.sub.1 had a low value exponent (0.382 with 95% CI of 0.271-0.499). This opens the opportunity of exploring fixed (weight-independent) dosing regimens for rFVIIIFc if such are of benefit to the patients.
[0636] AGE was included in the full covariate model as a very weak covariate, which was cancelled during the backward elimination of covariates. The dataset did not include individuals <12 years of age. Therefore, the activity of rFVIIIFc is not impacted by age for individuals aged >12 years.
[0637] External Validation of the rFVIIIFc Model
[0638] In order to further qualify the predictive performance of the PK model, an external validation procedure was performed. A model development (training) dataset was constructed, containing the intensive sampled profiles from the two studies (a total of 1162 observation records in the training set). In addition, a model validation set included all of the remaining observed data (predominantly peak and trough observations, a total of 888 observation records in the validation set). As the first step of the external validation, a model development procedure, similar to the base model development, was carried out with the training dataset. The parameters estimated from the whole dataset and from the training dataset only were very similar (results not shown).
[0639] At the validation step, the validation data (peak and trough data for occasions 3 through 7) were re-introduced. The model was run with parameter estimates set to the population means from the training set model with the NONMEM option MAXEVAL=0. The GoF diagnostics for the validation set only (troughs and peaks) are shown in FIG. 32. There was a very good agreement between the observed data in the validation dataset and the predicted data by the model developed on the training set.
[0640] Base Model for rFVIII
[0641] The base model for rFVIII (model Adv0D) is a two compartment model with covariates WT on V.sub.1 and study (STUD) on the peripheral volume (V2), BLOCK(2) IIV on CL, V.sub.1, common additive error and separated proportional residual error by study:
V 1 = TVV 1 [ WT 73 ] .THETA. 8 ( U ) V 2 = TVV 2 [ .THETA. 9 ] STUD ( V ) prop = STUD .THETA. 6 + ( 1 - STUD ) .THETA. 7 , where STUD = { 1 for Phase 1 0 for Phase 3 ( W ) ##EQU00011##
[0642] The population parameters of model Adv0D and the bootstrap-derived nonparametric 95% CIs are given in Table 26. No IOV was included in Adv0D as only single dose data were available for this agent. No covariate model was built in this case as developing a full rFVIII model was outside the scope of this modeling exercise.
[0643] The GoF diagnostics of model Adv0D are shown in FIG. 33.
TABLE-US-00026 TABLE 26 Population parameters and bootstrap-derived nonparametric 95% CI's for the base ADVATE .RTM. model Population Nonparametric Parameter Symbol Estimate 95% CI.sup.a Clearance, CL, [dL/h] .THETA..sub.1 2.53 2.32-2.78 Central Volume, V.sub.1, [dL] .THETA..sub.2 34.6 32.5-36.2 Allometric exponent on V.sub.1 .THETA..sub.8 0.508 0.277-0.762 Intercompartmental .THETA..sub.3 0.548 0.401-0.929 Clearance, Q, [dL/h] Peripheral Volume for Phase 3, .THETA..sub.4 4.94 3.82-6.51 V.sub.2, [dL] V.sub.2 Correcting Coefficient for .THETA..sub.9 2.17 1.64-3.00 Phase 1/2a IIV on CL, [%] .eta..sub.1 30.4 24.4-35.8 IIV on V.sub.1, [%] .eta..sub.2 16.2 11.4-19.3 Correlation between IIV on CL .eta..sub.12 0.532 N.C. .sup.b and V.sub.1 IIV on V.sub.2, [%] .eta..sub.4 30.6 0.31-42.4 Additive error, [IU/dL] .THETA..sub.5 0.110 0.00110-0.256 Proportional error, Phase 1/2a .THETA..sub.6 10.9 8.42-12.6 study, [%] Proportional error, Phase 3 study .THETA..sub.7 16.8 10.0-22.4 [%] .sup.aOut of 1000 bootstraps, 23 runs with minimization terminated were skipped when calculating the bootstrap results. .sup.b Nonparametric 95% CI of 0.00773-0.0442 for a population mean of the covariance .quadrature..sub.12 of 0.0263
[0644] The narrow CIs of the rFVIII model parameter estimates indicate that they were estimated with very good precision. V.sub.1 approximates the plasma volume, and the IIV of the activity was low to moderate. The residual errors of Adv0D were very low, and the additive error was less than one-quarter of the LLOQ. The proportional errors for both studies were of the same magnitude as the precision of the aPTT assay (CV <10%). This shows that Adv0D almost completely captured the information contained in the data; the unexplained variance was almost exclusively due to the measurement errors. The model diagnostics suggest that the model described the data adequately. There were no systematic deviations or shapes detectable in the residual plots. The lower end of the activities (which is the range of interest with respect to therapeutic effects) was approximated very well.
[0645] Model Implementation: Simulations of Prospective Dosing Regimens
[0646] The population PK models adequately describe the time course of both rFVIII and rFVIIIFc activity. Therefore, they can be used to simulate various dosing scenarios in the target population with the aim to explore and compare the resulting activity profiles. Such model based simulations have been widely used, especially in recent years, and have become a valuable tool in support of operational, regulatory, and therapeutic decision making.
[0647] In patients with hemophilia, it is widely accepted that 1 IU/dL (or 1% activity) is a threshold value under which the risk of bleeding increases (Collins P W, B. V., Fischer K, et al., Break-through bleeding in relation to predicted factor VIII levels in patients receiving prophylactic treatment for severe hemophilia A. J Thromb Haemost., 2009. 7(3): p. 413-20; MASAC, Recommendation #190 Concerning Products Licensed for the Treatment of Hemophilia and Other Bleeding Disorders. March 2009 (Replaced by Recommendation #215, November 2012). New York, N.Y.: National Hemophilia Foundation). It should be noted, however, that the threshold cannot be considered an "absolute criterion" by itself; other factors, such as duration of time with low activity levels, patient characteristics, etc. are likely also involved.
[0648] For the simulation of rFVIIIFc activity, the base model (Eq. Q) was used. This was preferred to the final model as: (i) the base model and the final model provided the same approximation of the data; the final model only assigned part of the IIV to the covariates selected, and (ii) no covariate model was developed for rFVIII, so it is meaningful to compare simulations from base models when FVIIIFc is referenced to rFVIII. In addition to that, at this moment, the course of the time-variant covariates, VWF and HCT, has not qualitatively characterized. In any case, the parameter values of the base and final models from Tables 24 and 25 indicate that the base model is adequate and can be used for simulations.
[0649] The simulations without uncertainty were performed with both the base model without BLQ data (considered to be mildly optimistic, see the Discussion section) and with the base model with BLQ data included (considered to be conservative, see the Discussion section). The simulations with uncertainty were based upon the base model without BLQ values.
[0650] Several rFVIIIFc prophylaxis dosing regimens that are of therapeutic interest have been simulated. Table 28 presents the predicted SS peaks and troughs of the rFVIIIFc activity-time profiles (5.sup.th, 25.sup.th, 50.sup.th [median], 75.sup.th, and 95.sup.th percentiles) at various dose levels administered every 3, 4, or 5 days (E3D, E4D, and E5D administration, respectively). The top section of Table 28 displays the simulation results with the base model with no BLQ data included and no uncertainty. The bottom section of Table 28 displays the simulation results with the base model with BLQ included and no uncertainty. The middle section of Table 28 displays the simulation results with uncertainty in the model parameters. The simulated SS activity profiles of selected rFVIIIFc prophylaxis dosing regimens are given in FIG. 35 for illustrative purposes. Panels A, C, E, and G display the simulations without uncertainty; panels B, D, F, and H display the 90% confidence regions around the 5%, 50%, and 95% percentile curves calculated from the uncertainty simulations.
[0651] These simulation results can be considered when determining long-term prophylaxis dosing regimens. It should be noted also that a dosing regimen of 65 IU/kg administered weekly (QW) is predicted to yield troughs >1 IU/dL in 26.6% of the individuals treated (also shown in FIG. 35, using the base model with no BLQ data), or 16.8% of the individuals treated (using the base model with BLQ data). The 90% confidence region of these predictions is 14.6% to 35.8%. The dosing regimens simulated include dose levels and dosing intervals that have been tested in the phase 1/2a and phase 3 studies. Therefore, the simulations can be considered to interpolate within the existing clinical experience, increasing the credibility of the predictions.
TABLE-US-00027 TABLE 27 Comparison of ADVATE .RTM. population PK parameters from the current analysis and the analysis published in Bjorkman 2012 A This Analysis Estimates from Parameter Estimates [Bjorkman 2012a] Clearance, CL, [dL/h] 2.53 2.30* Allometric exponent on CL Not estimated 0.8 Central Volume, V.sub.1, [dL] 34.6 28.6* Allometric exponent on V.sub.1 0.508 0.905 Intercompartmental Clearance, 0.548 1.47 Q, [dL/h] Peripheral Volume, V.sub.2, [dL] 4.94 8.92* Allometric exponent on V.sub.2 Not estimated 0.76 V.sub.2 Correcting Coefficient for 2.17 Not estimated Phase 1/2a IIV on CL, [%] 30.4 30.0 IIV on V.sub.1, [%] 16.2 21.0 Correlation between IIV on 0.532 0.45 CL and V.sub.1 IIV on V.sub.2, [%] 30.6 Not estimated Additive error, [IU/dL] 0.110 8.90 Proportional error, Phase 10.9 Not estimated 1/2a study, [%] Proportional error, Phase 16.8 Not estimated 3 study [%] *CL, V1 and V2 calculated for an average 73 kg, 30 yr old subject from equations 4-7 (Bjorkman 2012 A)
[0652] The dosing regimens simulated include dose levels (20-65 IU/kg) and dosing intervals that have been tested in the Phase 1/2a and Phase 3 studies. Therefore, the simulations can be considered to interpolate within the existing clinical experience, increasing the credibility of the predictions.
TABLE-US-00028 TABLE 28 Predicted SS peaks and troughs of the rFVIIIFc activity-time profiles with various dose regimens Unit Percentile Dosing Frequency Dose of Every 3 Days Every 4 Days Level Subjects Peak Trough Peak Trough 25 IU/kg 5% 35.2 <0.5.sup.a 34.9 <0.5.sup.a 50% 51.2 2.64 50.0 1.16 95% 74.5 10.2 70.7 5.69 40 IU/kg 5% 56.3 0.619 55.9 <0.5.sup.a 50% 82.0 4.22 80.0 1.85 95% 119 16.3 113 9.11 50 IU/kg 5% 70.4 0.774 69.9 <0.5.sup.a 50% 102 5.27 100 2.32 95% 149 20.4 141 11.4 25 IU/kg 5% 35.2 (33.8, 36.7) <0.5.sup.a (<0.5.sup.a, 0.545) 34.9 (33.7, 36.3) <0.5.sup.a (<0.5.sup.a, <0.5.sup.a) 50% 51.5 (50.5, 52.5) 2.63 (2.23, 3.05) 50.0 (49.0, 51.0) 1.16 (0.895, 1.45) 95% 74.5 (72.0, 77.0) 10.3 (8.60, 12.2) 71.0 (68.5, 73.5) 5.80 (4.60, 7.05) 40 IU/kg 5% 56.3 (54.1, 58.6) 0.591 (<0.5.sup.a, 0.872) 55.8 (53.8, 58.0) <0.5.sup.a (<0.5.sup.a, <0.5.sup.a) 50% 82.4 (80.8, 84.0) 4.21 (3.57, 4.88) 80.0 (78.4, 81.6) 1.85 (1.43, 2.31) 95% 119 (115, 123) 16.5 (13.8, 19.4) 114 (110, 118) 9.28 (7.35, 11.3) 50 IU/kg 5% 70.4 (67.6, 73.3) 0.739 (<0.5.sup.a, 1.09) 69.8 (67.3, 72.5) <0.5.sup.a (<0.5.sup.a, 0.521) 50% 103 (101, 105) 5.26 (4.46, 6.10) 100 (98.0, 102) 2.31 (1.79, 2.89) 95% 149 (144, 154) 20.6 (17.2, 24.3) 142 (137, 147) 11.6 (9.19, 14.1) 25 IU/kg 5% 37.2 <0.5.sup.a 37.0 <0.5.sup.a 50% 52.9 2.54 51.6 1.01 95% 75.6 10.8 71.8 5.92 40 IU/kg 5% 59.5 <0.5.sup.a 59.2 <0.5.sup.a 50% 84.7 4.06 82.5 1.61 95% 121 17.2 115 9.47 50 IU/kg 5% 74.3 0.509 74.1 <0.5.sup.a 50% 106 5.07 103 2.01 95% 151 21.5 144 11.8 Unit Percentile Dosing Frequency Dose of Every 5 Days Level Subjects Peak Trough Model 25 IU/kg 5% 34.6 <0.5.sup.a Base model 50% 49.2 0.549 with 95% 69.6 3.08 BLQ values 40 IU/kg 5% 55.3 <0.5.sup.a commented 50% 78.8 0.878 out 95% 111 4.94 50 IU/kg 5% 69.1 <0.5.sup.a 50% 98.5 1.10 95% 139 6.17 25 IU/kg 5% 34.3 (33.0, 35.9) <0.5.sup.a (<0.5.sup.a, <0.5.sup.a) Base model 50% 49.3 (48.2, 50.5) 0.535 (0.5.sup.a, 0.69) with 95% 69.5 (66.5, 72.5) 3.1 (2.27, 3.96) BLQ values 40 IU/kg 5% 54.8 (52.7, 57.4) <0.5.sup.a (<0.5.sup.a, <0.5.sup.a) commented 50% 78.8 (77.1, 80.8) 0.856 (0.560, 1.10) out 95% 111 (106, 116) 4.96 (3.63, 6.34) (with 50 IU/kg 5% 68.5 (65.9, 71.7) <0.5.sup.a (<0.5.sup.a, <0.5.sup.a) uncertainty)* 50% 98.5 (96.4, 101) 1.07 (0.700, 1.38) 95% 139 (133, 145) 6.20 (4.54, 7.92) 25 IU/kg 5% 35.8 <0.5.sup.a Base model 50% 51.0 <0.5.sup.a with 95% 70.9 3.27 BLQ (M3 40 IU/kg 5% 57.2 <0.5.sup.a method) 50% 81.5 0.619 95% 113 5.23 50 IU/kg 5% 71.5 <0.5.sup.a 50% 102 0.774 95% 142 6.54 .sup.aBelow the level of quantification. *Simulation results shown as median and 90% CI
[0653] Other Implementations
[0654] Although the rFVIIIFc and rFVIII population PK models were developed separately, a comparative evaluation of the individual Bayesian PK parameter estimates of the subjects (from the Phase 1 study and the Arm 1 PK Subgroup of the Phase 3 study) who received both rFVIII and rFVIIIFc indicates that they are highly correlated. FIG. 36A-C presents the individual Bayesian CL, V.sub.1, and Time to 1 IU/dL (Time 1%) estimates for rFVIII and rFVIIIFc, where each point represents one individual. The correlation coefficients are uniformly high: R=0.839 (R2=0.7043) for CL, R=0.862 (R2=0.7437) for V.sub.1, and R=0.865 (R2=0.7481) for Time 1%.
Discussion
[0655] The generally narrow CIs of the parameter value estimates of both the base and final rFVIIIFc models indicate that the population PK parameters were estimated with good precision. The PK behavior of the activity profiles as assessed by population analysis is typical for a FVIII product (Bjorkman S, Oh M, Spotts G, et al., Blood., 119(2):612-618 (2012)) with a peripheral compartment much smaller than the central volume (V.sub.2 is >5 times lower than V.sub.1). The V.sub.1 approximates the plasma volume.
[0656] By far the strongest covariate for rFVIIIFc identified in this analysis was vWF on CL. As a result of the inclusion of the vWF covariate on CL, the CV of the IIV on this parameter decreased by approximately 20%. These results are expected, as the vast majority of circulating FVIII (>95%) is in complex with vWF and is protected from proteolytic degradation, premature binding to its receptors, and rapid CL from the blood. The negative exponent on vWF indicates that the higher the measured level of vWF, the lower the rFVIII CL, which is in line with the above mechanistic hypothesis.
[0657] The (across and within) individual range of vWF in the model development dataset was in the range of 10-495%. The 10% value was repeated and found to be erroneous (after database lock). This would result in a variation of the rFVIIIFc CL from 3.85-1.10 dL/hr, the population mean being 1.65 dL/hr. It should be noted that VWF is a time-varying parameter within the same individual. The exact mechanisms and relationships governing this within-individual variation are not well elucidated or quantitatively characterized. A quantitative framework for the vWF level IIVs needs to be combined with the current population PK model to permit further investigation of the possible dosing implications of the VWF covariate. Another time-varying covariate that was identified was HCT on V.sub.1; however, the influence of HCT was rather weak. Such a relationship has not been reported for FVIII products previously and a mechanistic hypothesis linking HCT with FVIII activity has not been proposed.
[0658] Although no definitive effect of non-neutralizing antibodies on the observed activity was detected as a result of the population PK analysis, due to the small number of subjects with antibodies and the transient character of the antibody response, such an effect cannot be totally excluded.
[0659] The results from the VPC and the simulations indicate that both the full and the base model without the BLQ values (not shown) in the dataset mildly overestimate the trough activity. For example, with 65 IU QW dosing, the base model predicts that more than one-quarter of the individuals will have trough values above the 1 IU/dL threshold. This prediction can be compared with the results from Arm 2 (weekly dosing with 65 IU/kg) of the phase 3 study, where 9 of 21 (42.9%) had troughs above 1 IU/dL at Week 7; 6 of 19 (31.6%) had troughs above 1 IU/dL at Week 14, and 1 of 6 (16.7%) had troughs above 1 IU/dL at Week 18. On the other hand, both the full and base model with the BLQ values included seem to underestimate the trough activity--using the base version of this model predicts that 16.8% of the Arm 2 individuals will have troughs >1 IU/dL. This apparent discrepancy is reconciled in the simulations with uncertainty, where the predicted 90% CI include any of the respective predicted troughs and peaks using either the base model with or without BLQ values in the dataset (compare the middle section with the top and bottom sections of Table 28). These simulation results confirm the power of population PK model-based simulations with uncertainty, which can be seen as a generalization of the two alternative base models.
[0660] Evidence from the published literature (Bjorkman S, Folkesson A, Jonsson S., A. Eur J Clin Pharmacol; 65(10):989-998 2009), Bjorkman S, Oh M, Spotts G, et al., Blood., 119(2):612-618 (2012)), as well as from the current research, indicates that FVIII displays a 2-compartment disposition; however, the peripheral compartment has a small V.sub.1 and its impact on the activity profiles is very subtle. The weak influence of the second compartment on the observed activity profiles has led to the inability to fit a 2-compartment model to clinical data in at least one instance (Karafoulidou A, Suarez E, Anastasopoulou I, et al., Eur J Clin Pharmacol.; 65(11):1121-1130 (2009)).
[0661] The mechanisms determining the observed shapes are not well elucidated--as stated in Bjorkman S, Folkesson A, Jonsson S. A., Eur J Clin Pharmacol.; 65(10):989-998 (2009): " . . . It is still not clear whether the 2-compartment characteristic reflects distribution of FVIII from the circulation or rapid initial elimination of some of the injected protein." In the absence of well-defined mechanistic understanding, the information contained in the clinical data available remains critical for model selection.
[0662] The observed variation in the intercompartmental clearance (Tables 24 and 25) leads to the effect that for the models (either base or final) developed without BLQ data, the estimator captures a curvature in the profiles due to the second compartment close to the limit of detection. This behavior of the estimator is the source of the apparent terminal t.sub.1/2 value. It should be pointed out that: (i) such an overestimation occurs at very low activities, close to the LLOQ; (ii) such an overestimation is not likely to affect meaningfully the predictive performance of the model within the time window of interest (up to 5-7 days); and (iii) such an overestimation affects only a very small portion (less than 2-3%) of the overall area under the curve associated with the activities close to the LLOQ, where the divergence between the models begins.
[0663] When the BLQ values were reintroduced into the dataset and the M3 method was applied in NONMEM, the estimator seemed to move the curvature due to the second compartment toward the initial portion of the profile. It should be kept in mind that the M3 method treats the BLQ values as categorical variables and what happens under the LLOQ is quantitatively unknown.
[0664] A similar effect was observed for the 2 variants of the rFVIII base model (Table 26), where the model derived from phase 1/2a data overestimated terminal t.sub.1/2, whereas the model from the phase 3 data provided a terminal t112 value in line with the conventional analyses results. Similar to the rFVIIIFc models, the mean residence time (MRT) and the Time to 1% were largely unaffected. Based on this discussion, the rFVIIIFc models developed from data without the BLQ values as well as the rFVIII model reflective of the phase 1/2a data have the potential to over-predict the activity during simulation. Such an over-prediction within the time window of interest (up to 5-7 days) is expected to be low. On the other hand, the models developed from data with the BLQ values as well as the rFVIII model reflective of the phase 3 data have the potential to under-predict the activity during simulation. The impact of the model variation on the model predictions were quantified by the simulations performed.
[0665] The results from the uncertainty simulations demonstrate that any of the developed pivotal models (with and without BLQ values, base and final, etc.) can be used for simulations without an impact on the overall PK conclusions, provided that the random nature of the predictions is acknowledged. The selection of the simulation model should be determined by the objectives and/or the context (eg, risk tolerance) of the simulation exercise. When risk tolerance is low, the more conservative models (with the BLQ data included) may be the best simulation option. For population-oriented simulations (such as those shown in Table 28) the base model simulation is adequate, whereas for individual-oriented simulations, when the individual covariate values are of interest, the final covariate model may be more appropriate. It is suggested that simulations with uncertainty should be the preferred option, accounting for the inherent randomness of the simulations. It is also important to note that when referencing between rFVIII and rFVIIIFc dosing regimens, it is meaningful to use either the optimistic models for both agents, or the conservative models for both agents to avoid the potential of bias.
[0666] Although the external validation exercise was not conducted in a random manner, the results emphasize the strong predictive potential of the current population PK model and indicate that the peak and troughs in the long term can be predicted by a model developed on a semi-sparse sampling schedule. This represents one possible treatment scenario, when the physician adjusts the dosing regimen (initially or during the course of therapy) based on PK information derived from more or less intensive sampling scheme. Due to the low IOV, this adjustment is likely to be valid for extended periods in the absence of abrupt changes in the system state (such as illness, trauma, etc.).
[0667] There is a subtle difference between the rFVIII models derived from the phase 3 data and the one identified from the phase 1/2a data--the peripheral volume of distribution V.sub.2 is 4.94 dL from phase 3 and 2.17 times higher, when identified from phase 1/2a data. This difference may originate from the difference in the sampling schemes between the two studies (10-11 sampling points in phase 1/2a and fewer sampling points in phase 3) and makes the rFVIII phase 3 model more conservative with respect to predicting trough values (predicts lower trough values) than the rFVIII phase 1/2a model. This subtle difference is built into the STUD covariate (Table 26) and may account for any differences in design, assays, execution, and other conditions across the 2 studies. No BLQ model has been developed for rFVIII due to the very low number of BLQ values in the rFVIII dataset as a result of the shorter sampling window for this agent (see Table 23).
[0668] Table 27 shows that the FVIII population PK parameters from the current analysis and the analysis published by Bjorkman S, Oh M, Spotts G, et al., Blood, 119(2):612-618 (2010) are comparable, although there are differences in the analysis methodology. Bjorkman's model identified a weight dependence of CL and V.sub.2, which was not substantiated by our data. Additionally, age was not identified by our modeling as a covariate of rFVIIIFc clearance. It is worth mentioning that the data used by Bjorkman S, Oh M, Spotts G, et al., Blood, 119(2):612-618 (2010) include PK profiles from subjects as young as 1 year; hence the, age and weight range in this dataset may be considerably wider. The latter would facilitate the identification of WT/AGE covariates from such data.
[0669] The high positive correlations between the PK parameters of rFVIII and rFVIIIFc, illustrated in FIG. 36 A-C, suggest that individuals who had high CL values for rFVIII are very likely to have had high CL values for rFVIIIFc as well, and vice-versa. The population PK models predicted that the average population CL for rFVIIIFc (1.65 dL/hr) is about 35% lower than that of rFVIII (2.53 dL/hr). This is consistent with the geometric mean (95% CI) for the intraindividual CL ratio of rFVIIIFc to rFVIII (0.64 [0.60-0.69]) derived from the conventional 2-stage compartmental analysis. At the same time, the V.sub.1 panel of FIG. 36 A-C indicates that individuals had similar V.sub.1 values for rFVIII and for rFVIIIFc. These two relationships rise the hypothesis that individuals who had high time-related characteristics (such as t.sub.1/2, MRT, Time to 1%, and Time to 3%) for rFVIII are very likely to have had high characteristics for rFVIIIFc, and vice-versa. This hypothesis was confirmed in the Time 1% panel of FIG. 36 A-C, where the individual Times to 1%, calculated based on the Bayesian estimates from the rFVIII and rFVIIIFc model, are plotted.
[0670] Time to 1% activity is a PK outcome parameter that is directly related to frequency of dosing under the paradigm of maintaining target activity above this threshold. Therefore, based on the relationship identified, a conclusion can be made, that individuals who were on less frequent rFVIII dosing would require less frequent rFVIIIFc dosing, and vice-versa. Such a relationship could be useful when transition between the two products is considered.
[0671] Conclusions
[0672] The population PK analysis and simulations presented provide a comprehensive quantitative characterization of the activity-time profiles for rFVIIIFc and rFVIII. These confirm that the CL of rFVIIIFc is much lower than the CL of rFVIII, while the volumes of distribution at steady state are similar. This was first observed following noncompartmental analysis and conventional 2-stage analysis of the same data and explain the extended duration of activity achieved by rFVIIIFc relative to rFVIII.
[0673] The population PK model for rFVIIIFc was used for simulation of various dosing scenarios to aid dosing regimen selection and adjustment. Based on this, it was concluded that individuals on a less frequent rFVIII dosing regimen would require less frequent rFVIIIFc dosing, and vice-versa. Such a relationship could be useful when transitioning from one agent to the other.
[0674] The population PK models are useful tools for predicting peak, trough, and average activity of various dosing scenarios, and can be further extended to develop aids and methods for individualizing treatment. Many efforts have been made to correlate activity levels with bleeding risk, although a definitive quantitative relationship to calculate bleeding probability based on activity has not yet been identified. These population PK models may serve as a basis for the development of a population PK/pharmacodynamics model to better understand the relationship between FVIII activity and bleeding.
Example 12. Association of Bleeding Tendency with Time Under Target FIX Activity Levels in Severe Hemophilia B Patients Treated with Recombinant Factor IX-Fc Fusion Protein (rFIXFc)
[0675] The objective of this post hoc analysis was to evaluate the relationship between the annualized time spent under target 1, 3, and 5 IU/dL FIX activity levels and clinical outcomes (overall, spontaneous, traumatic, and joint bleeds), as well as the probability of experiencing bleeding episodes given time spent under the target trough.
[0676] Subjects
[0677] Subjects enrolled in the B-LONG study with available efficacy data were used for this analysis. This study included male subjects (.gtoreq.12 years of age) with hemophilia B (FIX levels .ltoreq.2 IU/dL), no history of FIX inhibitors, and .gtoreq.100 exposure days to FIX.
[0678] Design
[0679] B-LONG was a phase 3 interventional, nonrandomized, open-label, multicenter study of rFIXFc in subjects with hemophilia B.
[0680] Subjects were assigned by the investigator based on the clinical site's standard of care to 1 of 4 treatment arms: Arm 1, weekly prophylaxis (50 IU/kg every 7 days; dose adjusted to maintain factor levels); Arm 2, individualized interval prophylaxis (100 IU/kg dose, every 10 days; interval adjusted to maintain factor levels); Arm 3, episodic (on-demand) treatment as needed for bleeding episodes (20-100 IU/kg, depending on bleeding severity); Arm 4, perioperative management.
[0681] The dose (in Arm 1) and the interval (in Arm 2) were adjusted during the study to maintain a trough level of 1 to 3 IU/dL above baseline, or higher if clinically necessary. The end of the study was defined as the point in time when pre-specified criteria were reached (e.g., 53 subjects completed .gtoreq.50 rFIXFc exposure days, in conjunction with additional criteria).
[0682] Statistical Analysis
[0683] Data from the B-LONG study were used to evaluate the relationship between bleeding tendency and FIX activity in individuals with severe hemophilia B. A 3-compartment population pharmacokinetics model of rFIXFc was developed based on the activity-time profiles of 12 subjects from a phase 1/2a study 7 of rFIXFc and 123 subjects from the B-LONG study.
[0684] Individual post hoc pharmacokinetic parameters were used to construct continuous FIX activity-time profiles for each dose of rFIXFc administered over the course of the study for all individual subjects in the B-LONG study.
[0685] The cumulative time spent under the target trough FIX levels of 1, 3, and 5 IU/dL for each individual on-study was calculated and normalized to obtain an annualized time under the respective target trough level, expressed in days. The time spent under the target trough level (1, 3, or 5 IU/dL) is summarized by treatment arm (individualized weekly prophylaxis, individualized interval prophylaxis, and episodic treatment).
[0686] Negative binomial regression models, unadjusted and adjusted for the number of pre-study bleeding episodes and pre-treatment switch (i.e., switching from on-demand to prophylaxis), were used to evaluate the association between the annualized time spent under the target trough FIX activity levels of 1, 3, or 5 IU/dL and the number of bleeding episodes experienced on-study Subjects.
Results
[0687] Of the 123 subjects in the study, 117 subjects in the prophylactic and episodic arms had available information for calculating time spent under target trough levels; 106 subjects had available efficacy data for inclusion in multivariable models. Of the 117 subjects evaluated for time under the target trough, 2 declined to switch to study drug, 1 did not participate in the efficacy period, 7 were missing information regarding pre-study bleeding episodes, and 1 was missing information regarding pre-study treatment. Demographic and baseline characteristics for these 106 subjects were consistent with that expected in the severe hemophilia B population.
[0688] The median time under the target trough level is summarized by treatment arm in Table 29. The annualized median time spent under the 1 IU/dL target trough level in both prophylaxis arms was 0 days, while the annualized median time spent under the 1 IU/dL target trough level in the episodic arm was 146.28 days.
TABLE-US-00029 TABLE 29 Annualized Time (Days) Under Target FIX Trough Levels by Treatment Arm in the B-LONG Study.sup.a Weekly Individualized Episodic Target prophylaxis interval prophylaxis treatment trough level (N = 62) (n = 28) (n = 27) 1 IU/dL Mean (SD) 0.1 (0.81) 0.00 (0.00) 140.12 (95.79) Median 0.00 0.00 146.28 IQR 0.00, 0.00 0.00, 0.00 65.5, 214.2 3 IU/dL Mean (SD) 37.67 (43.47) 35.01 (32.39) 248.70 (76.33) Median 19.86 34.12 270.47 IQR 3.61, 64.92 8.87, 50.75 207.9, 298.6 5 IU/dL Mean (SD) 121.22 (73.28) 118.46 (52.84) 293.19 (43.06) Median 140.48 129.32 308.54 IQR 51.49, 178.5 78.74, 162.4 257.1, 302.6 FIX, factor IX; SD, standard deviation, IQR, interquartile range. .sup.aThe median (IQR) on-study weekly dose among subjects with time under target trough information in Arm 1 was 45.2 IU/kg (38.1, 53.7 IU/kg; n = 61) and in Arm 2 was 57.1 IU/kg (53.5, 68.9 IU/kg; n = 26).
[0689] The predicted ABRs by annualized time (in days) under the targeting trough FIX levels of 1, 3, and 5 IU/dL based on the adjusted negative binomial regression model are shown in FIG. 37.
[0690] Based on the unadjusted negative binomial regression model, for every additional day spent under the target troughs of 1, 3, and 5 IU/dL, there was an estimated increase in the overall ABR of 0.8%, 0.5%, and 0.5%, respectively (P <0.0001 for all comparisons). Based on the adjusted negative binomial regression model, for every additional day spent under the target troughs of 1, 3, and 5 IU/dL, there was an estimated increase in the overall ABR of 0.5%, 0.3%, and 0.2%, respectively (P <0.05 for all comparisons).
[0691] This is the first report to demonstrate a relationship between bleeding tendency and time spent under 1, 3, and 5 IU/dL FIX activity in hemophilia B subjects. The majority of subjects in the prophylaxis arms (60%) did not spend any time under 1 IU/dL FIX activity during the trial. Results of this study demonstrated a significant association between increased duration of time spent under a target therapeutic FIX activity level (1, 3, or 5 IU/dL) and an increased bleeding tendency, after adjusting for baseline bleeding tendency in the past 12 months and switching from an on-demand therapy at baseline to a prophylaxis regimen on-study. Although all trough levels were associated with changes in ABR, a steeper slope was seen with a target trough of 1 IU/dL; hence, that trough is more sensitive to change and potentially more meaningful to subjects compared with troughs of 3 and 5 IU/dL. The statistical power to determine a change in bleeding probability under a target trough of 1 IU/dL was limited due to the relatively small number of subjects spending time under this activity level. These results confirm the importance of a minimum therapeutic threshold of 1 IU/dL for prophylactic FIX replacement therapy and provide additional support for the use of 1% as the minimal trough level in the population pharmacokinetic simulations for establishing effective rFIXFc prophylaxis regimens.
Example 13. Dosing Long-Lasting Recombinant Factor VIII-Fc Fusion Protein (rFVIIIFc)Clotting Factors
[0692] A-LONG Study Design
[0693] A-LONG is a phase 3, open-label, multicenter, partially randomized study of the PK, efficacy, and safety of rFVIIIFc in patients with severe hemophilia A.
[0694] METHODS: The study enrolled 165 subjects into 1 of 3 treatment arms (FIG. 38). In Arm 1, dosing recommendations were based on individual subject PK evaluations to target a steady-state FVIII activity trough of 1% to 3% (1-3 IU/dL) or higher, with additional regimen adjustments made if the subject experienced .gtoreq.2 spontaneous bleeding episodes over a rolling 8-week period.
[0695] Study Population: Previously treated males aged .gtoreq.12 years with severe hemophilia A (<1 IU/dL [1%] endogenous FVIII activity or severe genotype) and treated prophylactically, or treated episodically and with a history of .gtoreq.12 bleeding events in the 12 months prior to the study. Exclusion criteria: history of inhibitors (neutralizing antibodies), history of hypersensitivity associated with any FVIII concentrate or intravenous immunoglobulin, or other coagulation disorders.
[0696] Prophylactic Dosing Subgroup Analysis: The subgroup of subjects with .gtoreq.6 months on-study who were (1) previously on prophylactic therapy (.gtoreq.2 injections/week) and assigned to the individualized prophylaxis arm (Arm 1), or (2) previously treated episodically and assigned to the weekly prophylaxis arm (Arm 2; FIG. 38) was analyzed. Self-reported information collected at the time of study enrollment from patient logs and/or hospital records included prestudy prophylactic dose and dosing frequency (infusions per week), and the number of bleeding episodes in the prior 12 months. On-study parameters recorded included rFVIIIFc dose and dosing interval (number of days), and the median ABR for the last 3 months on-study, once subjects' treatment regimens had stabilized. Subjects were stratified according to their final on-study rFVIIIFc dose and dosing interval, and the corresponding self-reported prestudy FVIII dose and infusion frequency were analyzed. Subjects were also stratified according to their prestudy FVIII infusion frequency, and their final on-study dosing interval was examined. Population PK models for rFVIIIFc and ADVATE.RTM. were developed based on A-LONG PK data (collected in 164 subjects over .ltoreq.52 weeks of treatment, and in 30 subjects participating in the sequential PK analysis, respectively), and factors that may be determinants of variability in FVIII activity were identified. Subjects were monitored for the development of inhibitors and adverse events. The presence of inhibitors was assessed by the Nijmegen-modified Bethesda assay. Descriptive statistics included the median and interquartile range (IQR) values for demographic characteristics, estimated number of prestudy bleeding events, and on-study ABR for the prophylactic dosing subgroups of Arms 1 and 2.
[0697] RESULTS: Study Participants--Baseline characteristics of the subjects in the prophylactic dosing subgroups were consistent with the overall A-LONG study population and were representative of a population with severe hemophilia A (FIG. 38). Among Arm 1 subjects previously treated prophylactically, >80% were on their prestudy regimen for 12 months; the most common products used for prophylaxis prior to study entry were Kogenate/Helixate (25/80 subjects; 31.3%) and rFVIII (22/80 subjects; 27.5%).
[0698] Dosing Interval Analysis: Nearly all subjects (79/80; 98.8%) had a decrease in the number of prophylactic infusions administered per week on-study compared with their self-reported prestudy infusion frequency, as shown in FIG. 39. Prior to entering the study, most subjects (65/80; 81.3%) reported a FVIII prophylactic regimen of 3 times per week. On-study, the most common rFVIIIFc prophylactic dosing intervals were every 3 days (29/80 subjects; 36.3%), twice weekly (23/80 subjects; 28.8%), and every 5 days (24/80 subjects; 30.0%).
[0699] On-study rFVIIIFc Dosing: The median on-study rFVIIIFc dose was 50 IU/kg, most commonly administered every 5 days (19/37 subjects; 51.4%), or every 3 days (16/37 subjects; 43.2% [Table 30, solid box]). At study end, 22/80 subjects (27.5%) were taking the twice-weekly starting regimen of 25 IU/kg on Day 1 and 50 IU/kg on Day 4 (Table 30, dashed box). Comparison of individual subject half-lives for rFVIII and rFVIIIFc in subjects from the A-LONG sequential PK subgroup indicates a longer half-life for rFVIIIFc compared with rFVIII (1.53-fold longer; P <0.0001), 5 which supports the increased dosing intervals for rFVIIIFc observed in the trial.
TABLE-US-00030 TABLE 30 Prescribed Prophylactic Dose and Dosing Interval (End of Study) in Arm 1 Subjects Last on-study dosing frequency Every Twice Every Every Dose per injection (IU/kg).sup.a 3 days weekly 4 days 5 days Total, n 25-35 4 -- -- -- 4 25/50.sup.b -- ##STR00001## -- -- 22 40-45 2 1 -- -- 3 50 ##STR00002## -- 2 ##STR00003## 37 60-65 7 -- 2 5 14 Total 29 23 4 24 80 .sup.aBlack boxes indicate most common dose at study end (50 IU/kg); dashed box indicates second most common regimen at study end (25 IU/kg (Day 1); 50 IU/kg (Day 4)). .sup.bInitial dosing regimen of 25 IU/kg on Day 1, followed by 50 IU/kg on Day 4.
[0700] Factor Consumption: Overall, weekly factor consumption for prophylaxis remained consistent for the majority of patients; the median difference in weekly dose (last on-study minus prestudy) was 4.4 (data not shown) Prestudy median (IQR) weekly dose: 78.0 IU/kg (60.0, 102.5). On-study (last 3 months) median (IQR) weekly dose: 79.2 IU/kg (72.1, 111.5).
[0701] Prior Episodic/Weekly Prophylaxis Subgroup (Arm 2): Per protocol, dose and dosing interval were unchanged in Arm 2 during the course of the study. The median (min, max) dose of rFVIIIFc was 65.9 (51.2, 76.5) IU/kg per week.
[0702] Efficacy Outcome: ABR: Median ABR in the last 3 months on-study was lower than the self-reported prestudy median number of bleeding episodes across all rFVIIIFc dosing interval subgroups, as shown in FIG. 40. Overall, subjects in the prior prophylaxis/individualized prophylaxis subgroup (Arm 1) reported a median of 6.0 bleeding episodes in the 12 months prior to study; in the last 3 months on-study they had a median ABR of 0.0. Subjects in the prior episodic/weekly prophylaxis subgroup (Arm 2) reported a median of 29.0 bleeding episodes in the 12 months prior to study; in the last 3 months on-study they had a median ABR of 4.0.
[0703] Simulation of FVIII Activity (Population PK Modeling): Dosing regimen simulations using population PK models of ADVATE.RTM. and rFVIIIFc predicted the proportion of subjects who would maintain a trough FVIII activity level at steady-state above 1 IU/dL (1%; FIG. 41). The values reported are the lowest and highest predicted proportions of subjects, respectively, who would remain protected (e.g., >1%) during the shortest and longest portions of the dosing period, respectively.
Example 14. The Bleeding Tendency in Relation to Predicted FVIII Activity Levels in Severe Hemophilia a Patients Treated with Recombinant Factor VIII Fc Fusion Protein (rFVIIIFc)
[0704] The objective of this post hoc analysis was to evaluate the relationship between the annualized time spent under target 1 IU/dL, 3 IU/dL, and 5 IU/dL FVIII activity levels and clinical outcomes (e.g., overall, spontaneous, traumatic, and joint bleeds), as well as the probability of experiencing .gtoreq.1 bleed given time spent under the target trough level.
[0705] METHODS: Subjects enrolled in the A-LONG study who had available efficacy data were used in this analysis. The study included previously-treated male subjects (.gtoreq.12 years of age) with severe hemophilia A and no history of FVIII inhibitors. Subjects on prophylaxis prior to study entry were assigned to treatment in Arm 1, individualized prophylaxis (twice-weekly dosing; 25 IU/kg on Day 1 and 50 IU/kg on Day 4 during the first week, followed by 25-65 IU/kg every 3-5 days; dose and interval adjusted to maintain factor trough levels of 1 to 3 IU/dL above baseline, or higher if clinically necessary). Subjects on prior episodic treatment were randomized to Arm 2, weekly prophylaxis (65 IU/kg), or Arm 3, episodic (on-demand) treatment as needed for bleeding episodes (10-50 IU/kg, depending on bleeding severity). The end of the study was defined as the point in time when prespecified criteria were reached (e.g., 104 subjects completed .gtoreq.50 rFVIIIFc exposure days, in conjunction with additional criteria).
[0706] Data from the A-LONG study were used to evaluate the relationship between bleeding tendency and FVIII activity in individuals with severe hemophilia A. A two-compartment population pharmacokinetics (PK) model of rFVIIIFc was developed based on FVIII activity data collected from a total of 180 subjects (16 subjects from a phase 1 study and 164 subjects from the phase 3 A-LONG study). Individual post hoc PK parameters were used to construct continuous FVIII activity-over-time profiles for each dose of rFVIIIFc administered over the course of the study for all individual subjects in the A-LONG study.
[0707] The cumulative annualized time spent under the target trough FVIII levels of 1 IU/dL, 3 IU/dL, and 5 IU/dL, for each individual on-study, was calculated and normalized to obtain an annualized time under the respective target trough level, expressed in days. The time spent under the target trough level (1 IU/dL, 3 IU/dL, and 5 IU/dL) is summarized by treatment arm (i.e., individualized prophylaxis, weekly prophylaxis, and episodic treatment). Negative binomial regression models, unadjusted and adjusted for the annualized number of pre-study bleeding episodes and pre-treatment switch (i.e., switching from on-demand to prophylaxis), were used to evaluate the association between the annualized time under the target trough FVIII levels of 1 IU/dL, 3 IU/dL, and 5 IU/dL and the numbers of spontaneous, traumatic, and joint bleeds, and bleeds overall. Logistic regression models, unadjusted and adjusted for the number of pre-study bleeding episodes and pre-treatment switch, were used to evaluate the association between the time spent under the target trough level of 1 IU/kg, 3 IU/kg, and 5 IU/kg and the probability of experiencing bleeding. Data were also stratified by the type of bleed (e.g., spontaneous, traumatic, or joint bleeds).
[0708] RESULTS: Of the 165 subjects who enrolled in the A-LONG study, the time spent under the target troughs was calculated for 163 subjects; 162 subjects had available data for inclusion in multivariable models. Demographic and baseline characteristics of subjects enrolled in A-LONG were consistent with that expected in a severe hemophilia A population (Table 31).
TABLE-US-00031 TALE 31 Baseline Demographic and Clinical Characteristics Total A-LONG population Characteristic (n = 165) Median (min, max) age, y 30.0 (12, 65) Median (min, max) weight, kg 71.60 (42.0, 127.4) Median (min, max) BMI, kg/m.sup.2 23.90 (15.3, 37.4) Race, n (%) White 107 (64.8) Asian 43 (26.1) Black 10 (6.1) Other 5 (3.0) Geographic location, n (%) North America 56 (33.9) Europe 41 (24.8) Other 68 (41.2) Received pre-study episodic treatment, 78/165 (47.3) n/N (%) Estimated median (min, max) number of 16 (0, 120) bleeding episodes during the 12 months prior to the start of the study BMI, body mass index.
[0709] The annualized median time under the target trough level is summarized by treatment group in Table 32 and FIG. 42. The annualized median time spent under the 1 IU/dL target trough level was 2.17 days in the individualized prophylaxis arm, 51.55 days in the weekly prophylaxis arm, and 224.8 days in the episodic treatment arm.
TABLE-US-00032 TABLE 32 Annualized Time (Days) Under Target FVIII Trough Levels by Treatment Arm in the A-LONG Study.sup.a Individualized Weekly Episodic Target prophylaxis prophylaxis treatment trough level (n = 117) (n = 23) (n = 23) 1 IU/dL Mean (SD) 9.5 (20.2) 54.81 (55.9) 200.7 (77.0) Median 2.17 51.55 244.8 IQR 0.00, 8.49 0.84, 98.81 140.3, 260.6 3 IU/dL Mean (SD) 50.19 (40.8) 126.2 (61.5) 246.3 (60.5) Median 43.72 130.3 266.6 IQR 21.75, 66.57 74.58, 176.7 195.2, 292.5 5 IU/dL Mean (SD) 91.36 (46.9) 159.6 (59.5) 267.1 (51.4) Median 92.39 167.3 284.0 IQR 66.44, 117.0 123.0, 205.8 225.8, 305.2 FVIII, factor VIII; SD, standard deviation, IQR, interquartile range. .sup.aThe median (IQR) on-study weekly dose among subjects with time under target trough information in Arm 1 was 77.9 IU/kg (72.3, 91.2 IU/kg; n = 117) and in Arm 2 was 65.6 IU/kg (64.2, 68.2 IU/kg; n = 23).
[0710] The predicted ABRs by annualized time (in days) under the target trough FVIII levels of 1 IU/dL, 3 IU/dL, and 5 IU/dL based on the unadjusted and adjusted negative binomial regression models are shown in FIGS. 43A and B, respectively. Based on both the unadjusted and adjusted negative binomial regression models, a significant increase was observed in the predicted overall ABR for each additional annualized day under the target troughs of 1 IU/dL, 3 IU/dL, and 5 IU/dL (FIG. 43). Based on the unadjusted negative binomial regression model, for every additional day spent under the target troughs of 1 IU/dL, 3 IU/dL, and 5 IU/dL, there was an estimated increase in the overall ABR of 1%, 0.9%, and 0.9%, respectively (P <0.0001 for all comparisons). Based on the adjusted negative binomial regression model, for every additional day spent under the target troughs of 1 IU/dL, 3 IU/dL, and 5 IU/dL, there was an estimated increase in the overall ABR of 0.9%, 0.8%, and 0.8%, respectively (P <0.0001 for all comparisons). For spontaneous bleeds, traumatic bleeds, and joint bleeds, a significant increase was also observed in the predicted ABR for each additional day under the target trough (1 IU/dL, 3 IU/dL, and 5 IU/dL), based on both the unadjusted and adjusted negative binomial regression models (P.ltoreq.0.0003).
[0711] The adjusted probability of experiencing any bleed according to the time (in days) under target trough FVIII levels of 1 IU/dL, 3 IU/dL, and 5 IU/dL is shown in FIG. 44. Results for the adjusted probability of experiencing spontaneous, traumatic, or joint bleeds according to time (in days) under target trough FVIII levels of 1 IU/dL, 3 IU/dL, and 5 IU/dL are also shown in FIG. 44. As the time spent under the target trough FVIII levels of 1 IU/dL, 3 IU/dL, and 5 IU/dL increased, the adjusted probability of experiencing all types of bleeding episodes increased.
Example 15. Pharmacokinetics of Recombinant Factor VIII Fc Fusion Protein (rFVIIIFc) in Previously-Treated Children with Severe Hemophilia A (Kids-ALONG)
[0712] Kids A-LONG was a phase 3 open-label study evaluating the safety, efficacy, and pharmacokinetics of recombinant factor VIII Fc fusion protein (rFVIIIFc), in previously treated children with severe hemophilia A (endogenous FVIII level <1 IU/dL [<1%]).
[0713] Methods: The study enrolled 71 subjects. The starting rFVIIIFc regimen was twice-weekly prophylaxis (Day 1, 25 IU/kg; Day 4, 50 IU/kg); dose (.ltoreq.80 IU/kg) and dosing interval (.gtoreq.2 days) were adjusted as needed. A subset of subjects had sequential pharmacokinetic evaluations of FVIII and rFVIIIFc. The primary endpoint was development of inhibitors (neutralizing antibodies). Secondary endpoints included pharmacokinetics, annualized bleeding rate (ABR) and number of infusions required to control a bleed.
[0714] Results: No subject developed an inhibitor to rFVIIIFc. Adverse events were typical of a pediatric hemophilia population. rFVIIIFc half-life was prolonged relative to FVIII, consistent with observations in adults and adolescents. The median ABR was 1.96 overall, and 0.00 for spontaneous bleeds; 46.4% of subjects reported no bleeding episodes on study. 93.0% of bleeding episodes were controlled with 1-2 infusions. The median average weekly rFVIIIFc prophylactic dose was 88.1 IU/kg. At study end, 62/69 of subjects (90%) were infusing twice-weekly. Among subjects previously on FVIII prophylaxis, 74% reduced their dosing frequency with rFVIIIFc.
[0715] Pharmacokinetics: Of the 60 subjects dosed with rFVIIIFc in the pharmacokinetics subgroup, 54 (<6 years of age, n=23; 6 to <12 years of age, n=31) had evaluable pharmacokinetic data by the one-stage clotting assay. The activity-time profiles in both age cohorts, adjusted for baseline and residual prestudy FVIII activity, were adequately characterized by noncompartmental analysis with moderate inter-subject variability. All numbers are given in arithmetic mean (95% confidence interval). The terminal half-life of rFVIIIFc in subjects aged <6 years of age and 6 to <12 years of age was 12.67 (11.23, 14.11) hours and 14.88 (11.98, 17.77) hours, respectively. An age-dependent effect on clearance was observed, with mean clearance higher in the younger cohort of 3.60 (3.13, 4.07) mL/h/kg than in the older cohort of 2.78 (2.44, 3.13) mL/h/kg. Incremental recovery of rFVIIIFc was consistent between the age cohorts (mean of approximately 2 IU/dL per IU/kg) (with the younger cohort having 1.92 (1.80, 2.04) IU/dL per IU/kg and the older cohort having 2.44 (2.07, 2.80) IU/dL per IU/kg. The mean recovery time was 17.24 (15.40, 19.07) hours in the younger cohort and 20.90 (17.06, 24.74) in the older cohort. The volume of distribution at steady state was 58.58 (54.90, 62.27) mL/kg for the younger cohort and 52.13 (45.25, 59.01) mL/kg for the older cohort. The dose normalized area under the concentration-time curve was 30.04 (26.45, 33.63) IU*h/dL per IU/kg for the younger cohort and 41.87 (34.00, 49.75) IU*h/dL per IU/kg for the older cohort.
Example 16. Population Pharmacokinetic Analysis of Long-Acting Recombinant Factor VIII-Fc Fusion Protein (rFVIIIFc) in Adult, Adolescent, and Pediatric Patients with Severe Haemophilia A
[0716] The population pharmacokinetic (popPK) data for the adult/adolescent (.gtoreq.12 years) and pediatric studies discussed above were combined to develop a new rFVIIIFc popPK model. As before (see Examples 9 and 11; Tables 18, 24, and 25), a final model (Table 33) was developed from base and covariate models.
TABLE-US-00033 TABLE 33 Final Model Population Parameter Estimates and Bootstrap-derived Nonparametric 95% CI's Population % Nonparametric Parameter Estimate RSE 95% CI.sup.a Clearance, CL, [dL/h] 1.56 2.01 1.49, 1.64 Central Volume, V1, [dL] 32.8 1.22 31.5, 33.6 Intercompartmental Clearance, Q, [dL/h] 0.157 77.1 0.0468, 1.18 Peripheral Volume, V2, [dL] 2.93 19.9 2.41, 5.43 Allometric exponent on CL/Q 0.704 4.47 0.640, 0.760 Allometric exponent on V1/V2 0.945 2.17 0.908, 0.987 Exponent on VWF~CL -0.413 10.1 -0.497, -0.330 .omega..sup.2.sub.CL (IIV; inter-individual variability) 0.0585 12.4 0.0432, 0.0741 .omega..sup.2.sub.V1 (IIV) 0.0265 13.8 0.0198, 0.0337 Covariance.sub.CL:V1 (IIV) 0.0185 23.5 0.0109, 0.0266 .omega.2CL (IOV; inter-occasion variability) 0.0470 13.9 0.0342, 0.0604 .omega..sup.2.sub.V1 (IOV) 0.00987 41.9 0.00323, 0.0197 Covariance.sub.CL:V1 (IOV) 0.0110 40.2 0.00444, 0.0228 Additive error, Phase 1/2a study, [IU/dL] 0.402 20.3 0.172, 0.600 Additive error, Phase 3 and Pediatric study, [IU/dL] 0.217 14.6 0.161, 0.285 Proportional error, Phase 1/2a and Phase 3 study [%] 15.4 8.44 12.7, 17.7 Proportional error, Pediatric study [%] 21.2 6.70 18.1, 24.3
[0717] The model-predicted steady state (SS) peaks and troughs of the rFVIIIFc activity-time profiles for various rFVIIIFc dosing regimens are presented in Table 34 (for adult/adolescents (.gtoreq.12 years)), Table 35 (6 to <1 2 year) and Table 36 (<6 year age cohorts). These results can be considered when determining the chronic dosing regimens for prophylaxis.
TABLE-US-00034 TABLE 34 Predicted steady state (SS) peaks and troughs of the rFVIIIFc activity-time profiles with 50 IU/kg dose administered every 3, 4, or 5 days for .gtoreq.12 years. Unit Percentile Dosing Frequency Dose Of Every 3 Days Every 4 Days Every 5 Days Every 7 Days Level Subjects Peak Trough Peak Trough Peak Trough Peak Trough 25 IU/kg 5% 37.8 <0.5.sup.a 37.0 <0.5.sup.a 36.7 <0.5.sup.a -- -- 25% 46.4 1.07 45.0 <0.5.sup.a 44.1 <0.5.sup.a -- -- 50% 53.1 2.39 51.1 0.922 50.1 <0.5.sup.a -- -- 75% 60.2 4.71 58.2 2.10 56.7 0.932 -- -- 95% 73.3 10.6 69.9 5.49 68.5 2.79 -- -- 40 IU/kg 5% 60.5 0.522 59.2 <0.5.sup.a 58.7 <0.5.sup.a -- -- 25% 74.3 1.71 71.9 0.589 70.6 <0.5.sup.a -- -- 50% 85.0 3.83 81.7 1.48 80.2 0.613 -- -- 75% 96.3 7.53 93.1 3.35 90.8 1.49 -- -- 95% 117 16.9 112 8.78 110 4.47 -- -- 50 IU/kg 5% 75.7 0.654 73.9 <0.5.sup.a 73.4 <0.5.sup.a -- -- 25% 92.9 2.14 89.9 0.737 88.3 <0.5.sup.a -- -- 50% 106 4.78 102 1.84 100 0.766 -- -- 75% 120 9.41 116 4.19 113 1.86 -- -- 95% 147 21.1 140 11.0 137 5.59 -- -- 65 IU/kg 5% 98.3 0.850 96.1 <0.5.sup.a 95.4 <0.5.sup.a 94.2 <0.5.sup.a 25% 121 2.78 117 0.958 115 <0.5.sup.a 114 <0.5.sup.a 50% 138 6.22 133 2.40 130 0.995 130 <0.5.sup.a 75% 157 12.2 151 5.45 148 2.42 146 0.586 95% 191 27.5 182 14.3 178 7.27 177 2.63 .sup.aBelow the level of quantitation of 0.5 IU/dL.
TABLE-US-00035 TABLE 35 Predicted steady state (SS) peaks and troughs of the rFVIIIFc activity-time profiles with various dose levels administered every 3, 4, or 5 days for 6 to <12 years. Unit Percentile Dosing Frequency Dose Of Every 2 Days Every 3 Days Every 4 Days Every 5 Days Level Subjects Peak Trough Peak Trough Peak Trough Peak Trough 25 IU/kg 5% 37.7 0.868 35.3 <0.5.sup.a 35.2 <0.5.sup.a 34.2 <0.5.sup.a 25% 45.6 2.29 43.1 0.586 42.3 <0.5.sup.a 41.6 <0.5.sup.a 50% 52.1 3.97 49.3 1.25 48.4 <0.5.sup.a 47.5 <0.5.sup.a 75% 59.7 6.40 56.3 2.35 54.7 0.921 54.0 <0.5.sup.a 95% 72.5 12.9 67.7 5.07 66.1 2.43 65.7 1.15 40 IU/kg 5% 60.3 1.39 56.5 <0.5.sup.a 56.3 <0.5.sup.a 54.7 <0.5.sup.a 25% 73.0 3.67 69.0 0.937 67.6 <0.5.sup.a 66.5 <0.5.sup.a 50% 83.3 6.34 78.9 2.00 77.5 0.638 76.0 <0.5.sup.a 75% 95.5 10.2 90.1 3.76 87.6 1.47 86.4 0.585 95% 116 20.6 108 8.12 106 3.88 105 1.85 50 IU/kg 5% 75.4 1.74 70.6 <0.5.sup.a 70.3 <0.5.sup.a 68.4 <0.5.sup.a 25% 91.3 4.58 86.2 1.17 84.5 <0.5.sup.a 83.1 <0.5.sup.a 50% 104 7.93 98.6 2.49 96.8 0.797 95.0 <0.5.sup.a 75% 119 12.8 113 4.70 109 1.84 108 0.731 95% 145 25.7 135 10.1 132 4.86 131 2.31 65 IU/kg 5% 98.0 2.26 91.8 <0.5.sup.a 91.4 <0.5.sup.a 88.9 <0.5.sup.a 25% 119 5.96 112 1.52 110 <0.5.sup.a 108 <0.5.sup.a 50% 135 10.3 128 3.24 126 1.04 123 <0.5.sup.a 75% 155 16.6 146 6.10 142 2.39 140 0.950 95% 189 33.4 176 13.2 172 6.31 171 3.00 80 IU/kg 5% 121 2.78 113 0.599 113 <0.5.sup.a 109 <0.5.sup.a 25% 146 7.33 138 1.87 135 0.552 133 <0.5.sup.a 50% 167 12.7 158 3.99 155 1.28 152 <0.5.sup.a 75% 191 20.5 180 7.51 175 2.95 173 1.17 95% 232 41.1 217 16.2 212 7.77 210 3.69 .sup.aBelow the level of quantitation of 0.5 IU/dL.
TABLE-US-00036 TABLE 36 Predicted steady state (SS) peaks and troughs of the rFVIIIFc activity-time profiles with various dose levels administered every 3, 4, or 5 days for <6 years. Unit Percentile Dosing Frequency Dose Of Every 2 Days Every 3 Days Every 4 Days Every 5 Days Level Subjects Peak Trough Peak Trough Peak Trough Peak Trough 25 IU/kg 5% 35.6 0.512 33.7 <0.5.sup.a 33.8 <0.5.sup.a 32.9 <0.5.sup.a 25% 42.9 1.43 41.1 <0.5.sup.a 40.6 <0.5.sup.a 40.1 <0.5.sup.a 50% 48.8 2.54 47.0 0.700 46.5 <0.5.sup.a 45.8 <0.5.sup.a 75% 55.9 4.22 53.5 1.39 52.4 <0.5.sup.a 51.8 <0.5.sup.a 95% 67.3 8.75 64.2 3.13 63.3 1.42 63.2 0.586 40 IU/kg 5% 57.0 0.820 54.0 <0.5.sup.a 54.0 <0.5.sup.a 52.6 <0.5.sup.a 25% 68.7 2.28 65.8 <0.5.sup.a 65.0 <0.5.sup.a 64.2 <0.5.sup.a 50% 78.1 4.06 75.3 1.12 74.3 <0.5.sup.a 73.2 <0.5.sup.a 75% 89.5 6.75 85.5 2.22 83.8 0.738 82.8 <0.5.sup.a 95% 108 14.0 103 5.01 101 2.27 101 0.938 50 IU/kg 5% 71.2 1.03 67.4 <0.5.sup.a 67.5 <0.5.sup.a 65.8 <0.5.sup.a 25% 85.8 2.85 82.2 0.613 81.2 <0.5.sup.a 80.2 <0.5.sup.a 50% 97.7 5.07 94.1 1.40 92.9 <0.5.sup.a 91.5 <0.5.sup.a 75% 112 8.44 107 2.78 105 0.922 104 <0.5.sup.a 95% 135 17.5 128 6.26 127 2.84 126 1.17 65 IU/kg 5% 92.6 1.33 87.7 <0.5.sup.a 87.8 <0.5.sup.a 85.5 <0.5.sup.a 25% 112 3.71 107 0.797 106 <0.5.sup.a 104 <0.5.sup.a 50% 127 6.59 122 1.81 121 0.505 119 <0.5.sup.a 75% 145 11.0 139 3.61 136 1.20 135 <0.5.sup.a 95% 175 22.7 167 8.14 165 3.69 164 1.52 80 IU/kg 5% 114 1.64 108 <0.5.sup.a 108 <0.5.sup.a 105 <0.5.sup.a 25% 137 4.56 132 0.981 130 <0.5.sup.a 128 <0.5.sup.a 50% 156 8.12 151 2.32 149 0.621 146 <0.5.sup.a 75% 179 13.5 171 4.44 168 1.48 166 0.542 95% 215 28.0 206 10.0 203 4.54 202 1.88 .sup.aBelow the level of quantitation of 0.5 IU/dL.
[0718] The foregoing description of the specific embodiments will so fully reveal the general nature of the invention that others can, by applying knowledge within the skill of the art, readily modify and/or adapt for various applications such specific embodiments, without undue experimentation, without departing from the general concept of the present invention. Therefore, such adaptations and modifications are intended to be within the meaning and range of equivalents of the disclosed embodiments, based on the teaching and guidance presented herein. It is to be understood that the phraseology or terminology herein is for the purpose of description and not of limitation, such that the terminology or phraseology of the present specification is to be interpreted by the skilled artisan in light of the teachings and guidance.
TABLE-US-00037 TABLE 37 Polynucleotide Sequences: FIX-Fc A. FIX-Fc Chain DNA Sequence (SEQ ID NO: 1, which encodes SEQ ID NO: 2) pSYN-FIX-030 Nucleotide sequence (nt 1 to 7583): FIX exon 1 (signal peptide, 1st amino acid propeptide): nt 690-777 FIX mini intron: nt 778-1076 FIX propeptide sequence: nt 1077-1126 Mature FIX sequence: nt 1127-2371 Fc: nt 2372-3052 gcgcgcgttgacattgattattgactagttattaatagtaatcaattacggggtcattagttcatagcccatat- atgg agttccgcgttacataacttacggtaaatggcccgcctggctgaccgcccaacgacccccgcccattgacgtca- ataa tgacgtatgttcccatagtaacgccaatagggactttccattgacgtcaatgggtggagtatttacggtaaact- gccc acttggcagtacatcaagtgtatcatatgccaagtacgccccctattgacgtcaatgacggtaaatggcccgcc- tggc attatgcccagtacatgaccttatgggactttcctacttggcagtacatctacgtattagtcatcgctattacc- atgg tgatgcggttttggcagtacatcaatgggcgtggatagcggtttgactcacggggatttccaagtctccacccc- attg acgtcaatgggagtttgttttggcaccaaaatcaacgggactttccaaaatgtcgtaacaactccgccccattg- acgc aaatgggcggtaggcgtgtacggtgggaggtctatataagcagagctctctggctaactagagaacccactgct- tact ggcttatcgaaattaatacgactcactatagggagacccaagcttcgcgacgtacggccgccaccatgcagcgc- gtga acatgatcatggcagaatcaccaggcctcatcaccatctgccttttaggatatctactcagtgctgaatgtaca- ggtt tgtttccttttttaaaatacattgagtatgcttgccttttagatatagaaatatctgatgctgtcttcttcact- aaat tttgattacatgatttgacagcaatattgaagagtctaacagccagcacgcaggttggtaagtactgtgggaac- atca cagattttggctccatgccctaaagagaaattggctttcagattatttggattaaaaacaaagactttcttaag- agat gtaaaattttcatgatgttttcttttttgctaaaactaaagaattattcttttacatttcagtttttcttgatc- atga aaacgccaacaaaattctgaatcggccaaagaggtataattcaggtaaattggaagagtttgttcaagggaatc- taga gagagaatgtatggaagaaaagtgtagttttgaagaagcacgagaagtttttgaaaacactgaaagaacaactg- aatt ttggaagcagtatgttgatggagatcagtgtgagtccaatccatgtttaaatggcggcagttgcaaggatgaca- ttaa ttcctatgaatgttggtgtccctttggatttgaaggaaagaactgtgaattagatgtaacatgtaacattaaga- atgg cagatgcgagcagttttgtaaaaatagtgctgataacaaggtggtttgctcctgtactgagggatatcgacttg- caga aaaccagaagtcctgtgaaccagcagtgccatttccatgtggaagagtttctgtttcacaaacttctaagctca- cccg tgctgagactgtttttcctgatgtggactatgtaaattctactgaagctgaaaccattttggataacatcactc- aaag cacccaatcatttaatgacttcactcgggttgttggtggagaagatgccaaaccaggtcaattcccttggcagg- ttgt tttgaatggtaaagttgatgcattctgtggaggctctatcgttaatgaaaaatggattgtaactgctgcccact- gtgt tgaaactggtgttaaaattacagttgtcgcaggtgaacataatattgaggagacagaacatacagagcaaaagc- gaaa tgtgattcgaattattcctcaccacaactacaatgcagctattaataagtacaaccatgacattgcccttctgg- aact ggacgaacccttagtgctaaacagctacgttacacctatttgcattgctgacaaggaatacacgaacatcttcc- tcaa atttggatctggctatgtaagtggctggggaagagtcttccacaaagggagatcagctttagttcttcagtacc- ttag agttccacttgttgaccgagccacatgtcttcgatctacaaagttcaccatctataacaacatgttctgtgctg- gctt ccatgaaggaggtagagattcatgtcaaggagatagtgggggaccccatgttactgaagtggaagggaccagtt- tctt aactggaattattagctggggtgaagagtgtgcaatgaaaggcaaatatggaatatataccaaggtgtcccggt- atgt caactggattaaggaaaaaacaaagctcactgacaaaactcacacatgcccaccgtgcccagctccggaactcc- tggg cggaccgtcagtcttcctcttccccccaaaacccaaggacaccctcatgatctcccggacccctgaggtcacat- gcgt ggtggtggacgtgagccacgaagaccctgaggtcaagttcaactggtacgtggacggcgtggaggtgcataatg- ccaa gacaaagccgcgggaggagcagtacaacagcacgtaccgtgtggtcagcgtcctcaccgtcctgcaccaggact- ggct gaatggcaaggagtacaagtgcaaggtctccaacaaagccctcccagcccccatcgagaaaaccatctccaaag- ccaa agggcagccccgagaaccacaggtgtacaccctgcccccatcccgggatgagctgaccaagaaccaggtcagcc- tgac ctgcctggtcaaaggcttctatcccagcgacatcgccgtggagtgggagagcaatgggcagccggagaacaact- acaa gaccacgcctcccgtgttggactccgacggctccttcttcctctacagcaagctcaccgtggacaagagcaggt- ggca gcaggggaacgtcttctcatgctccgtgatgcatgaggctctgcacaaccactacacgcagaagagcctctccc- tgtc tccgggtaaatgagaattcagacatgataagatacattgatgagtttggacaaaccacaactagaatgcagtga- aaaa aatgctttatttgtgaaatttgtgatgctattgctttatttgtaaccattataagctgcaataaacaagttggg- gtgg gcgaagaactccagcatgagatccccgcgctggaggatcatccagccggcgtcccggaaaacgattccgaagcc- caac ctttcatagaaggcggcggtggaatcgaaatctcgtagcacgtgtcagtcctgctcctcggccacgaagtgcac- gcag ttgccggccgggtcgcgcagggcgaactcccgcccccacggctgctcgccgatctcggtcatggccggcccgga- ggcg tcccggaagttcgtggacacgacctccgaccactcggcgtacagctcgtccaggccgcgcacccacacccaggc- cagg gtgttgtccggcaccacctggtcctggaccgcgctgatgaacagggtcacgtcgtcccggaccacaccggcgaa- gtcg tcctccacgaagtcccgggagaacccgagccggtcggtccagaactcgaccgctccggcgacgtcgcgcgcggt- gagc accggaacggcactggtcaacttggccatggtttagttcctcaccttgtcgtattatactatgccgatatacta- tgcc gatgattaattgtcaacacgtgctgatcagatccgaaaatggatatacaagctcccgggagctttttgcaaaag- ccta ggcctccaaaaaagcctcctcactacttctggaatagctcagaggcagaggcggcctcggcctctgcataaata- aaaa aaattagtcagccatggggcggagaatgggcggaactgggcggagttaggggcgggatgggcggagttaggggc- ggga ctatggttgctgactaattgagatgcatgctttgcatacttctgcctgctggggagcctggggactttccacac- ctgg ttgctgactaattgagatgcatgctttgcatacttctgcctgctggggagcctggggactttccacaccctcgt- cgag ctagcttcgtgaggctccggtgcccgtcagtgggcagagcgcacatcgcccacagtccccgagaagttgggggg- aggg gtcggcaattgaaccggtgcctagagaaggtggcgcggggtaaactgggaaagtgatgtcgtgtactggctccg- cctt tttcccgagggtgggggagaaccgtatataagtgcagtagtcgccgtgaacgttctttttcgcaacgggtttgc- cgcc agaacacaggtaagtgccgtgtgtggttcccgcgggcctggcctctttacgggttatggcccttgcgtgccttg- aatt acttccacctggctccagtacgtgattcttgatcccgagctggagccaggggcgggccttgcgctttaggagcc- cctt cgcctcgtgcttgagttgaggcctggcctgggcgctggggccgccgcgtgcgaatctggtggcaccttcgcgcc- tgtc tcgctgctttcgataagtctctagccatttaaaatttttgatgacctgctgcgacgctttttttctggcaagat- agtc ttgtaaatgcgggccaggatctgcacactggtatttcggtttttggggccgcgggcggcgacggggcccgtgcg- tccc agcgcacatgttcggcgaggcggggcctgcgagcgcggccaccgagaatcggacgggggtagtctcaagctggc- cggc ctgctctggtgcctggcctcgcgccgccgtgtatcgccccgccctgggcggcaaggctggcccggtcggcacca- gttg cgtgagcggaaagatggccgcttcccggccctgctccagggggctcaaaatggaggacgcggcgctcgggagag- cggg cgggtgagtcacccacacaaaggaaaggggcctttccgtcctcagccgtcgcttcatgtgactccacggagtac- cggg cgccgtccaggcacctcgattagttctggagcttttggagtacgtcgtctttaggttggggggaggggttttat- gcga tggagtttccccacactgagtgggtggagactgaagttaggccagcttggcacttgatgtaattctccttggaa- tttg ccctttttgagtttggatcttggttcattctcaagcctcagacagtggttcaaagtttttttcttccatttcag- gtgt cgtgaacacgtggtcgcggccgcgccgccaccatggagacagacacactcctgctatgggtactgctgctctgg- gttc caggttccactggtgacaaaactcacacatgcccaccgtgcccagcacctgaactcctgggaggaccgtcagtc- ttcc tcttccccccaaaacccaaggacaccctcatgatctcccggacccctgaggtcacatgcgtggtggtggacgtg- agcc acgaagaccctgaggtcaagttcaactggtacgtggacggcgtggaggtgcataatgccaagacaaagccgcgg- gagg agcagtacaacagcacgtaccgtgtggtcagcgtcctcaccgtcctgcaccaggactggctgaatggcaaggag- taca agtgcaaggtctccaacaaagccctcccagcccccatcgagaaaaccatctccaaagccaaagggcagccccga- gaac cacaggtgtacaccctgcccccatcccgcgatgagctgaccaagaaccaggtcagcctgacctgcctggtcaaa- ggct tctatcccagcgacatcgccgtggagtgggagagcaatgggcagccggagaacaactacaagaccacgcctccc- gtgt tggactccgacggctccttcttcctctacagcaagctcaccgtggacaagagcaggtggcagcaggggaacgtc- ttct catgctccgtgatgcatgaggctctgcacaaccactacacgcagaagagcctctccctgtctccgggtaaatga- ctcg agagatctggccggctgggcccgtttcgaaggtaagcctatccctaaccctctcctcggtctcgattctacgcg- tacc ggtcatcatcaccatcaccattgagtttaaacccgctgatcagcctcgactgtgccttctagttgccagccatc- tgtt gtttgcccctcccccgtgccttccttgaccctggaaggtgccactcccactgtcctttcctaataaaatgagga- aatt gcatcgcattgtctgagtaggtgtcattctattctggggggtggggtggggcaggacagcaagggggaggattg- ggaa gacaatagcaggcatgctggggatgcggtgggctctatggcttctgaggcggaaagaaccagtggcggtaatac- ggtt atccacagaatcaggggataacgcaggaaagaacatgtgagcaaaaggccagcaaaaggccaggaaccgtaaaa- aggc cgcgttgctggcgtttttccataggctccgcccccctgacgagcatcacaaaaatcgacgctcaagtcagaggt- ggcg aaacccgacaggactataaagataccaggcgtttccccctagaagctccctcgtgcgctctcctgttccgaccc- tgcc gcttaccggatacctgtccgcctttctcccttcgggaagcgtggcgctttctcatagctcacgctgtaggtatc- tcag ttcggtgtaggtcgttcgctccaagctgggctgtgtgcacgaaccccccgttcagcccgaccgctgcgccttat- ccgg taactatcgtcttgagtccaacccggtaagacacgacttatcgccactggcagcagccactggtaacaggatta- gcag agcgaggtatgtaggcggtgctacagagttcttgaagtggtggcctaactacggctacactagaagaacagtat- ttgg tatctgcgctctgctgaagccagttaccttcggaaaaagagttggtagctcttgatccggcaaacaaaccaccg- ctgg tagcggtggtttttttgtttgcaagcagcagattacgcgcagaaaaaaaggatctcaagaagatcctttgatct- tttc tacggggtctgacgctcagtggaacgaaaactcacgttaagggattttggtcatgacattaacctataaaaata- ggcg tatcacgaggccctttcgtctcgcgcgtttcggtgatgacggtgaaaacctctgacacatgcagctcccggaga- cggt cacagcttgtctgtaagcggatgccgggagcagacaagcccgtcagggcgcgtcagcgggtgttggcgggtgtc- gggg ctggcttaactatgcggcatcagagcagattgtactgagagtgcaccatatatgcggtgtgaaataccgcacag- atgc gtaaggagaaaataccgcatcaggcgccattcgccattcaggctgcgcaactgttgggaagggcgatcggtgcg- ggcc tcttcgctattacgcca B. Fc DNA sequence (mouse ID( signal peptide underlined) (SEQ ID NO: 3, which encodes SEQ ID NO: 4) This is the Fc cassette from pSYN-FIX-030. In addition, there is a separate Fc expression cassette that was transfected into the cell line in plasmid pSYN-Fc-015 that encodes the same amino acid sequence, but contains a few noncoding changes. The second copy of Fc encoding sequence enables a better monomer: dimer ratio. Atggagacagacacactcctgctatgggtactgctgctctgggttccaggttccactggtgacaaaactcacac- atgcc caccgtgcccagcacctgaactcctgggaggaccgtcagtcttcctcttccccccaaaacccaaggacaccctc- atgat ctcccggacccctgaggtcacatgcgtggtggtggacgtgagccacgaagaccctgaggtcaagttcaactggt- acg tggacggcgtggaggtgcataatgccaagacaaagccgcgggaggagcagtacaacagcacgtaccgtgtggtc- a gcgtcctcaccgtcctgcaccaggactggctgaatggcaaggagtacaagtgcaaggtctccaacaaagccctc- cca gcccccatcgagaaaaccatctccaaagccaaagggcagccccgagaaccacaggtgtacaccctgcccccatc- cc gcgatgagctgaccaagaaccaggtcagcctgacctgcctggtcaaaggcttctatcccagcgacatcgccgtg- gagt gggagagcaatgggcagccggagaacaactacaagaccacgcctcccgtgttggactccgacggctccttcttc- ctct acagcaagctcaccgtggacaagagcaggtggcagcaggggaacgtcttctcatgctccgtgatgcatgaggct- ctg cacaaccactacacgcagaagagcctctccctgtctccgggtaaa
TABLE-US-00038 TABLE 38 Polypeptide Sequences FIX-Fc Monomer Hybrid: created by coexpressing FIX-Fc and Fc chains. A. FIX-Fc chain (SEQ ID NO: 2): (28 amino acid signal sequence underlined, 18 amino acid propeptide double underlined, Fc portion in italics.) The C-terminal lysine is not present in either subunit; this Processing is often observed in recombinant proteins produced in mammalian cell culture, as well as with plasma derived proteins. FIXFC-SC SUBUNIT: FIX Signal Peptide: -46 MQRVNMIMAE SPGLITICLL GYLLSAEC FIX Propeptide: -18 TVFLDHENAN KILNRPKR 1 YNSGKLEEFV QGNLERECME EKCSFEEARE VFENTERTTE FWKQYVDGDQ 51 CESNPCLNGG SCKDDINSYE CWCPFGFEGK NCELDVTCNI KNGRCEQFCK 101 NSADNKVVCS CTEGYRLAEN QKSCEPAVPF PCGRVSVSQT SKLTRAETVF 151 PDVDYVNSTE AETILDNITQ STQSFNDFTR VVGGEDAKPG QFPWQVVLNG 201 KVDAFCGGSI VNEKWIVTAA HCVETGVKIT VVAGEHNIEE TEHTEQKRNV 251 IRIIPHHNYN AAINKYNHDI ALLELDEPLV LNSYVTPICI ADKEYTNIFL 301 KFGSGYVSGW GRVFHKGRSA LVLQYLRVPL VDRATCLRST KFTIYNNMFC 351 AGFHEGGRDS CQGDSGGPHV TEVEGTSFLT GIISWGEECA MKGKYGIYTK 401 VSRYVNWIKE KTKLTDKTHT CPPCPAPELL GGPSVFLFPP KPKDTLMISR 451 TPEVTCVVVD VSHEDPEVKF NWYVDGVEVH NAKTKPREEQ YNSTYRVVSV 501 LTVLHQDWLN GKEYKCKVSN KALPAPIEKT ISKAKGQPRE PQVYTLPPSR 551 DELTKNQVSL TCLVKGFYPS DIAVEWESNG QPENNYKTTP PVLDSDGSFF 601 LYSKLTVDKS RWQQGNVFSC SVMHEALHNH YTQKSLSLSP GK B. Fc chain (SEQ ID NO: 4) 20 amino acid heterologous mouse ID( light chain signal peptide (underlined): -20 METDTLLLWV LLLWVPGSTG Mature Fc sequence (corresponding to human IgG1 amino acids 221 to 447, EU numbering) 1 DKTHTCPPCP APELLGGPSV FLFPPKPKDT LMISRTPEVT CVVVDVSHED 51 PEVKFNWYVD GVEVHNAKTK PREEQYNSTY RVVSVLTVLH QDWLNGKEYK 101 CKVSNKALPA PIEKTISKAK GQPREPQVYT LPPSRDELTK NQVSLTCLVK 151 GFYPSDIAVE WESNGQPENN YKTTPPVLDS DGSFFLYSKL TVDKSRWQQG 201 NVFSCSVMHE ALHNHYTQKS LSLSPGK
TABLE-US-00039 TABLE 39 FVIIIFc Polynucleotide Sequences A. B-Domain Deleted FVIIIFc (i) B-Domain Deleted FVIIIFc Chain DNA Sequence (FVIII signal peptide underlined. Fc region in bold) (SEQ ID NO: 5, which encodes SEQ ID NO: 6) A TGCAAATAGA GCTCTCCACC TGCTTCTTTC TGTGCCTTTT GCGATTCTGC TTTAGTGCCA CCAGAAGATA CTACCTGGGT GCAGTGGAAC TGTCATGGGA CTATATGCAA AGTGATCTCG GTGAGCTGCC TGTGGACGCA AGATTTCCTC CTAGAGTGCC AAAATCTTTT CCATTCAACA CCTCAGTCGT GTACAAAAAG ACTCTGTTTG TAGAATTCAC GGATCACCTT TTCAACATCG CTAAGCCAAG GCCACCCTGG ATGGGTCTGC TAGGTCCTAC CATCCAGGCT GAGGTTTATG ATACAGTGGT CATTACACTT AAGAACATGG CTTCCCATCC TGTCAGTCTT CATGCTGTTG GTGTATCCTA CTGGAAAGCT TCTGAGGGAG CTGAATATGA TGATCAGACC AGTCAAAGGG AGAAAGAAGA TGATAAAGTC TTCCCTGGTG GAAGCCATAC ATATGTCTGG CAGGTCCTGA AAGAGAATGG TCCAATGGCC TCTGACCCAC TGTGCCTTAC CTACTCATAT CTTTCTCATG TGGACCTGGT AAAAGACTTG AATTCAGGCC TCATTGGAGC CCTACTAGTA TGTAGAGAAG GGAGTCTGGC CAAGGAAAAG ACACAGACCT TGCACAAATT TATACTACTT TTTGCTGTAT TTGATGAAGG GAAAAGTTGG CACTCAGAAA CAAAGAACTC CTTGATGCAG GATAGGGATG CTGCATCTGC TCGGGCCTGG CCTAAAATGC ACACAGTCAA TGGTTATGTA AACAGGTCTC TGCCAGGTCT GATTGGATGC CACAGGAAAT CAGTCTATTG GCATGTGATT GGAATGGGCA CCACTCCTGA AGTGCACTCA ATATTCCTCG AAGGTCACAC ATTTCTTGTG AGGAACCATC GCCAGGCGTC CTTGGAAATC TCGCCAATAA CTTTCCTTAC TGCTCAAACA CTCTTGATGG ACCTTGGACA GTTTCTACTG TTTTGTCATA TCTCTTCCCA CCAACATGAT GGCATGGAAG CTTATGTCAA AGTAGACAGC TGTCCAGAGG AACCCCAACT ACGAATGAAA AATAATGAAG AAGCGGAAGA CTATGATGAT GATCTTACTG ATTCTGAAAT GGATGTGGTC AGGTTTGATG ATGACAACTC TCCTTCCTTT ATCCAAATTC GCTCAGTTGC CAAGAAGCAT CCTAAAACTT GGGTACATTA CATTGCTGCT GAAGAGGAGG ACTGGGACTA TGCTCCCTTA GTCCTCGCCC CCGATGACAG AAGTTATAAA AGTCAATATT TGAACAATGG CCCTCAGCGG ATTGGTAGGA AGTACAAAAA AGTCCGATTT ATGGCATACA CAGATGAAAC CTTTAAGACT CGTGAAGCTA TTCAGCATGA ATCAGGAATC TTGGGACCTT TACTTTATGG GGAAGTTGGA GACACACTGT TGATTATATT TAAGAATCAA GCAAGCAGAC CATATAACAT CTACCCTCAC GGAATCACTG ATGTCCGTCC TTTGTATTCA AGGAGATTAC CAAAAGGTGT AAAACATTTG AAGGATTTTC CAATTCTGCC AGGAGAAATA TTCAAATATA AATGGACAGT GACTGTAGAA GATGGGCCAA CTAAATCAGA TCCTCGGTGC CTGACCCGCT ATTACTCTAG TTTCGTTAAT ATGGAGAGAG ATCTAGCTTC AGGACTCATT GGCCCTCTCC TCATCTGCTA CAAAGAATCT GTAGATCAAA GAGGAAACCA GATAATGTCA GACAAGAGGA ATGTCATCCT GTTTTCTGTA TTTGATGAGA ACCGAAGCTG GTACCTCACA GAGAATATAC AACGCTTTCT CCCCAATCCA GCTGGAGTGC AGCTTGAGGA TCCAGAGTTC CAAGCCTCCA ACATCATGCA CAGCATCAAT GGCTATGTTT TTGATAGTTT GCAGTTGTCA GTTTGTTTGC ATGAGGTGGC ATACTGGTAC ATTCTAAGCA TTGGAGCACA GACTGACTTC CTTTCTGTCT TCTTCTCTGG ATATACCTTC AAACACAAAA TGGTCTATGA AGACACACTC ACCCTATTCC CATTCTCAGG AGAAACTGTC TTCATGTCGA TGGAAAACCC AGGTCTATGG ATTCTGGGGT GCCACAACTC AGACTTTCGG AACAGAGGCA TGACCGCCTT ACTGAAGGTT TCTAGTTGTG ACAAGAACAC TGGTGATTAT TACGAGGACA GTTATGAAGA TATTTCAGCA TACTTGCTGA GTAAAAACAA TGCCATTGAA CCAAGAAGCT TCTCTCAAAA CCCACCAGTC TTGAAACGCC ATCAACGGGA AATAACTCGT ACTACTCTTC AGTCAGATCA AGAGGAAATT GACTATGATG ATACCATATC AGTTGAAATG AAGAAGGAAG ATTTTGACAT TTATGATGAG GATGAAAATC AGAGCCCCCG CAGCTTTCAA AAGAAAACAC GACACTATTT TATTGCTGCA GTGGAGAGGC TCTGGGATTA TGGGATGAGT AGCTCCCCAC ATGTTCTAAG AAACAGGGCT CAGAGTGGCA GTGTCCCTCA GTTCAAGAAA GTTGTTTTCC AGGAATTTAC TGATGGCTCC TTTACTCAGC CCTTATACCG TGGAGAACTA AATGAACATT TGGGACTCCT GGGGCCATAT ATAAGAGCAG AAGTTGAAGA TAATATCATG GTAACTTTCA GAAATCAGGC CTCTCGTCCC TATTCCTTCT ATTCTAGCCT TATTTCTTAT GAGGAAGATC AGAGGCAAGG AGCAGAACCT AGAAAAAACT TTGTCAAGCC TAATGAAACC AAAACTTACT TTTGGAAAGT GCAACATCAT ATGGCACCCA CTAAAGATGA GTTTGACTGC AAAGCCTGGG CTTATTTCTC TGATGTTGAC CTGGAAAAAG ATGTGCACTC AGGCCTGATT GGACCCCTTC TGGTCTGCCA CACTAACACA CTGAACCCTG CTCATGGGAG ACAAGTGACA GTACAGGAAT TTGCTCTGTT TTTCACCATC TTTGATGAGA CCAAAAGCTG GTACTTCACT GAAAATATGG AAAGAAACTG CAGGGCTCCC TGCAATATCC AGATGGAAGA TCCCACTTTT AAAGAGAATT ATCGCTTCCA TGCAATCAAT GGCTACATAA TGGATACACT ACCTGGCTTA GTAATGGCTC AGGATCAAAG GATTCGATGG TATCTGCTCA GCATGGGCAG CAATGAAAAC ATCCATTCTA TTCATTTCAG TGGACATGTG TTCACTGTAC GAAAAAAAGA GGAGTATAAA ATGGCACTGT ACAATCTCTA TCCAGGTGTT TTTGAGACAG TGGAAATGTT ACCATCCAAA GCTGGAATTT GGCGGGTGGA ATGCCTTATT GGCGAGCATC TACATGCTGG GATGAGCACA CTTTTTCTGG TGTACAGCAA TAAGTGTCAG ACTCCCCTGG GAATGGCTTC TGGACACATT AGAGATTTTC AGATTACAGC TTCAGGACAA TATGGACAGT GGGCCCCAAA GCTGGCCAGA CTTCATTATT CCGGATCAAT CAATGCCTGG AGCACCAAGG AGCCCTTTTC TTGGATCAAG GTGGATCTGT TGGCACCAAT GATTATTCAC GGCATCAAGA CCCAGGGTGC CCGTCAGAAG TTCTCCAGCC TCTACATCTC TCAGTTTATC ATCATGTATA GTCTTGATGG GAAGAAGTGG CAGACTTATC GAGGAAATTC CACTGGAACC TTAATGGTCT TCTTTGGCAA TGTGGATTCA TCTGGGATAA AACACAATAT TTTTAACCCT CCAATTATTG CTCGATACAT CCGTTTGCAC CCAACTCATT ATAGCATTCG CAGCACTCTT CGCATGGAGT TGATGGGCTG TGATTTAAAT AGTTGCAGCA TGCCATTGGG AATGGAGAGT AAAGCAATAT CAGATGCACA GATTACTGCT TCATCCTACT TTACCAATAT GTTTGCCACC TGGTCTCCTT CAAAAGCTCG ACTTCACCTC CAAGGGAGGA GTAATGCCTG GAGACCTCAG GTGAATAATC CAAAAGAGTG GCTGCAAGTG GACTTCCAGA AGACAATGAA AGTCACAGGA GTAACTACTC AGGGAGTAAA ATCTCTGCTT ACCAGCATGT ATGTGAAGGA GTTCCTCATC TCCAGCAGTC AAGATGGCCA TCAGTGGACT CTCTTTTTTC AGAATGGCAA AGTAAAGGTT TTTCAGGGAA ATCAAGACTC CTTCACACCT GTGGTGAACT CTCTAGACCC ACCGTTACTG ACTCGCTACC TTCGAATTCA CCCCCAGAGT TGGGTGCACC AGATTGCCCT GAGGATGGAG GTTCTGGGCT GCGAGGCACA GGACCTCTAC GACAAAACTC ACACATGCCC ACCGTGCCCA GCTCCAGAAC TCCTGGGCGG ACCGTCAGTC TTCCTCTTCC CCCCAAAACC CAAGGACACC CTCATGATCT CCCGGACCCC TGAGGTCACA TGCGTGGTGG TGGACGTGAG CCACGAAGAC CCTGAGGTCA AGTTCAACTG GTACGTGGAC GGCGTGGAGG TGCATAATGC CAAGACAAAG CCGCGGGAGG AGCAGTACAA CAGCACGTAC CGTGTGGTCA GCGTCCTCAC CGTCCTGCAC CAGGACTGGC TGAATGGCAA GGAGTACAAG TGCAAGGTCT CCAACAAAGC CCTCCCAGCC CCCATCGAGA AAACCATCTC CAAAGCCAAA GGGCAGCCCC GAGAACCACA GGTGTACACC CTGCCCCCAT CCCGGGATGA GCTGACCAAG AACCAGGTCA GCCTGACCTG CCTGGTCAAA GGCTTCTATC CCAGCGACAT CGCCGTGGAG TGGGAGAGCA ATGGGCAGCC GGAGAACAAC TACAAGACCA CGCCTCCCGT GTTGGACTCC GACGGCTCCT TCTTCCTCTA CAGCAAGCTC ACCGTGGACA AGAGCAGGTG GCAGCAGGGG AACGTCTTCT CATGCTCCGT GATGCATGAG GCTCTGCACA ACCACTACAC GCAGAAGAGC CTCTCCCTGT CTCCGGGTAA A (ii) Fc DNA sequence (mouse IgK signal peptide underlined) (SEQ ID NO: 7, which encodes SEQ ID NO: 8) ATGGA GACAGACACA CTCCTGCTAT GGGTACTGCT GCTCTGGGTT CCAGGTTCCA CTGGTGACAA AACTCACACA TGCCCACCGT GCCCAGCACC TGAACTCCTG GGAGGACCGT CAGTCTTCCT CTTCCCCCCA AAACCCAAGG ACACCCTCAT GATCTCCCGG ACCCCTGAGG TCACATGCGT GGTGGTGGAC GTGAGCCACG AAGACCCTGA GGTCAAGTTC AACTGGTACG TGGACGGCGT GGAGGTGCAT AATGCCAAGA CAAAGCCGCG GGAGGAGCAG TACAACAGCA CGTACCGTGT GGTCAGCGTC CTCACCGTCC TGCACCAGGA CTGGCTGAAT GGCAAGGAGT ACAAGTGCAA GGTCTCCAAC AAAGCCCTCC CAGCCCCCAT CGAGAAAACC ATCTCCAAAG CCAAAGGGCA GCCCCGAGAA CCACAGGTGT ACACCCTGCC CCCATCCCGC GATGAGCTGA CCAAGAACCA GGTCAGCCTG ACCTGCCTGG TCAAAGGCTT CTATCCCAGC GACATCGCCG TGGAGTGGGA GAGCAATGGG CAGCCGGAGA ACAACTACAA GACCACGCCT CCCGTGTTGG ACTCCGACGG CTCCTTCTTC CTCTACAGCA AGCTCACCGT GGACAAGAGC AGGTGGCAGC AGGGGAACGT CTTCTCATGC TCCGTGATGC ATGAGGCTCT GCACAACCAC TACACGCAGA AGAGCCTCTC CCTGTCTCCG GGTAAA B. Full Length FVIIIFc (i) Full Length FVIIIFc DNA Sequence (FVIII signal peptide underlined, Fc region in bold) (SEQ ID NO: 9, which encodes SEQ ID NO: 10) ATG CAAATAGAGC TCTCCACCTG CTTCTTTCTG TGCCTTTTGC GATTCTGCTT TAGTGCCACC AGAAGATACT ACCTGGGTGC AGTGGAACTG TCATGGGACT ATATGCAAAG TGATCTCGGT GAGCTGCCTG TGGACGCAAG ATTTCCTCCT AGAGTGCCAA AATCTTTTCC ATTCAACACC TCAGTCGTGT ACAAAAAGAC TCTGTTTGTA GAATTCACGG ATCACCTTTT CAACATCGCT AAGCCAAGGC CACCCTGGAT GGGTCTGCTA GGTCCTACCA TCCAGGCTGA GGTTTATGAT ACAGTGGTCA TTACACTTAA GAACATGGCT TCCCATCCTG TCAGTCTTCA TGCTGTTGGT GTATCCTACT GGAAAGCTTC TGAGGGAGCT GAATATGATG ATCAGACCAG TCAAAGGGAG AAAGAAGATG ATAAAGTCTT CCCTGGTGGA AGCCATACAT ATGTCTGGCA GGTCCTGAAA GAGAATGGTC CAATGGCCTC TGACCCACTG TGCCTTACCT ACTCATATCT TTCTCATGTG GACCTGGTAA AAGACTTGAA TTCAGGCCTC ATTGGAGCCC TACTAGTATG TAGAGAAGGG AGTCTGGCCA AGGAAAAGAC ACAGACCTTG CACAAATTTA TACTACTTTT TGCTGTATTT GATGAAGGGA AAAGTTGGCA CTCAGAAACA AAGAACTCCT TGATGCAGGA TAGGGATGCT GCATCTGCTC GGGCCTGGCC TAAAATGCAC ACAGTCAATG GTTATGTAAA CAGGTCTCTG CCAGGTCTGA TTGGATGCCA CAGGAAATCA GTCTATTGGC ATGTGATTGG AATGGGCACC ACTCCTGAAG TGCACTCAAT ATTCCTCGAA GGTCACACAT TTCTTGTGAG GAACCATCGC CAGGCGTCCT TGGAAATCTC GCCAATAACT TTCCTTACTG CTCAAACACT CTTGATGGAC CTTGGACAGT TTCTACTGTT TTGTCATATC TCTTCCCACC AACATGATGG CATGGAAGCT TATGTCAAAG TAGACAGCTG TCCAGAGGAA CCCCAACTAC GAATGAAAAA TAATGAAGAA GCGGAAGACT ATGATGATGA TCTTACTGAT TCTGAAATGG ATGTGGTCAG GTTTGATGAT GACAACTCTC CTTCCTTTAT CCAAATTCGC TCAGTTGCCA AGAAGCATCC TAAAACTTGG GTACATTACA TTGCTGCTGA AGAGGAGGAC TGGGACTATG CTCCCTTAGT CCTCGCCCCC GATGACAGAA GTTATAAAAG TCAATATTTG AACAATGGCC CTCAGCGGAT TGGTAGGAAG TACAAAAAAG TCCGATTTAT GGCATACACA GATGAAACCT TTAAGACTCG TGAAGCTATT CAGCATGAAT CAGGAATCTT GGGACCTTTA CTTTATGGGG AAGTTGGAGA CACACTGTTG ATTATATTTA AGAATCAAGC AAGCAGACCA TATAACATCT ACCCTCACGG AATCACTGAT GTCCGTCCTT TGTATTCAAG GAGATTACCA AAAGGTGTAA AACATTTGAA GGATTTTCCA ATTCTGCCAG GAGAAATATT CAAATATAAA TGGACAGTGA CTGTAGAAGA TGGGCCAACT AAATCAGATC CTCGGTGCCT GACCCGCTAT TACTCTAGTT TCGTTAATAT GGAGAGAGAT CTAGCTTCAG GACTCATTGG CCCTCTCCTC ATCTGCTACA AAGAATCTGT AGATCAAAGA GGAAACCAGA TAATGTCAGA CAAGAGGAAT GTCATCCTGT TTTCTGTATT TGATGAGAAC CGAAGCTGGT ACCTCACAGA GAATATACAA CGCTTTCTCC CCAATCCAGC TGGAGTGCAG CTTGAGGATC CAGAGTTCCA AGCCTCCAAC ATCATGCACA GCATCAATGG CTATGTTTTT GATAGTTTGC AGTTGTCAGT TTGTTTGCAT GAGGTGGCAT ACTGGTACAT TCTAAGCATT GGAGCACAGA CTGACTTCCT TTCTGTCTTC TTCTCTGGAT ATACCTTCAA ACACAAAATG GTCTATGAAG ACACACTCAC CCTATTCCCA TTCTCAGGAG AAACTGTCTT CATGTCGATG GAAAACCCAG GTCTATGGAT TCTGGGGTGC CACAACTCAG ACTTTCGGAA CAGAGGCATG ACCGCCTTAC TGAAGGTTTC TAGTTGTGAC AAGAACACTG GTGATTATTA CGAGGACAGT TATGAAGATA TTTCAGCATA CTTGCTGAGT AAAAACAATG CCATTGAACC AAGAAGCTTC TCCCAGAATT CAAGACACCC TAGCACTAGG CAAAAGCAAT TTAATGCCAC CACAATTCCA GAAAATGACA TAGAGAAGAC TGACCCTTGG TTTGCACACA GAACACCTAT GCCTAAAATA CAAAATGTCT CCTCTAGTGA TTTGTTGATG CTCTTGCGAC AGAGTCCTAC TCCACATGGG CTATCCTTAT CTGATCTCCA AGAAGCCAAA TATGAGACTT TTTCTGATGA TCCATCACCT GGAGCAATAG ACAGTAATAA CAGCCTGTCT GAAATGACAC ACTTCAGGCC ACAGCTCCAT CACAGTGGGG ACATGGTATT TACCCCTGAG TCAGGCCTCC AATTAAGATT AAATGAGAAA CTGGGGACAA CTGCAGCAAC AGAGTTGAAG AAACTTGATT TCAAAGTTTC TAGTACATCA AATAATCTGA TTTCAACAAT TCCATCAGAC AATTTGGCAG CAGGTACTGA TAATACAAGT TCCTTAGGAC CCCCAAGTAT GCCAGTTCAT TATGATAGTC AATTAGATAC CACTCTATTT GGCAAAAAGT CATCTCCCCT TACTGAGTCT GGTGGACCTC TGAGCTTGAG TGAAGAAAAT AATGATTCAA AGTTGTTAGA ATCAGGTTTA ATGAATAGCC AAGAAAGTTC ATGGGGAAAA AATGTATCGT CAACAGAGAG TGGTAGGTTA TTTAAAGGGA AAAGAGCTCA TGGACCTGCT TTGTTGACTA AAGATAATGC CTTATTCAAA GTTAGCATCT CTTTGTTAAA GACAAACAAA ACTTCCAATA ATTCAGCAAC TAATAGAAAG ACTCACATTG ATGGCCCATC ATTATTAATT GAGAATAGTC CATCAGTCTG GCAAAATATA TTAGAAAGTG ACACTGAGTT TAAAAAAGTG ACACCTTTGA TTCATGACAG AATGCTTATG GACAAAAATG CTACAGCTTT GAGGCTAAAT CATATGTCAA ATAAAACTAC TTCATCAAAA AACATGGAAA TGGTCCAACA GAAAAAAGAG GGCCCCATTC CACCAGATGC ACAAAATCCA GATATGTCGT TCTTTAAGAT GCTATTCTTG CCAGAATCAG CAAGGTGGAT ACAAAGGACT CATGGAAAGA ACTCTCTGAA CTCTGGGCAA GGCCCCAGTC CAAAGCAATT AGTATCCTTA GGACCAGAAA AATCTGTGGA AGGTCAGAAT TTCTTGTCTG AGAAAAACAA AGTGGTAGTA GGAAAGGGTG AATTTACAAA GGACGTAGGA CTCAAAGAGA TGGTTTTTCC AAGCAGCAGA AACCTATTTC TTACTAACTT GGATAATTTA CATGAAAATA ATACACACAA TCAAGAAAAA AAAATTCAGG AAGAAATAGA AAAGAAGGAA ACATTAATCC AAGAGAATGT AGTTTTGCCT CAGATACATA CAGTGACTGG CACTAAGAAT TTCATGAAGA ACCTTTTCTT ACTGAGCACT AGGCAAAATG TAGAAGGTTC ATATGACGGG GCATATGCTC CAGTACTTCA AGATTTTAGG TCATTAAATG ATTCAACAAA TAGAACAAAG AAACACACAG CTCATTTCTC AAAAAAAGGG GAGGAAGAAA ACTTGGAAGG CTTGGGAAAT CAAACCAAGC AAATTGTAGA GAAATATGCA TGCACCACAA GGATATCTCC TAATACAAGC CAGCAGAATT TTGTCACGCA ACGTAGTAAG AGAGCTTTGA AACAATTCAG ACTCCCACTA GAAGAAACAG AACTTGAAAA AAGGATAATT GTGGATGACA CCTCAACCCA GTGGTCCAAA AACATGAAAC ATTTGACCCC GAGCACCCTC ACACAGATAG ACTACAATGA GAAGGAGAAA GGGGCCATTA CTCAGTCTCC CTTATCAGAT TGCCTTACGA GGAGTCATAG CATCCCTCAA GCAAATAGAT CTCCATTACC CATTGCAAAG GTATCATCAT TTCCATCTAT TAGACCTATA TATCTGACCA GGGTCCTATT CCAAGACAAC TCTTCTCATC TTCCAGCAGC ATCTTATAGA AAGAAAGATT CTGGGGTCCA AGAAAGCAGT CATTTCTTAC AAGGAGCCAA AAAAAATAAC CTTTCTTTAG CCATTCTAAC CTTGGAGATG ACTGGTGATC AAAGAGAGGT TGGCTCCCTG GGGACAAGTG CCACAAATTC AGTCACATAC AAGAAAGTTG AGAACACTGT TCTCCCGAAA CCAGACTTGC CCAAAACATC TGGCAAAGTT GAATTGCTTC CAAAAGTTCA CATTTATCAG AAGGACCTAT TCCCTACGGA AACTAGCAAT GGGTCTCCTG GCCATCTGGA TCTCGTGGAA GGGAGCCTTC TTCAGGGAAC AGAGGGAGCG ATTAAGTGGA ATGAAGCAAA CAGACCTGGA AAAGTTCCCT TTCTGAGAGT AGCAACAGAA AGCTCTGCAA AGACTCCCTC CAAGCTATTG GATCCTCTTG CTTGGGATAA CCACTATGGT ACTCAGATAC CAAAAGAAGA GTGGAAATCC CAAGAGAAGT CACCAGAAAA AACAGCTTTT AAGAAAAAGG ATACCATTTT GTCCCTGAAC GCTTGTGAAA GCAATCATGC AATAGCAGCA ATAAATGAGG GACAAAATAA GCCCGAAATA GAAGTCACCT GGGCAAAGCA AGGTAGGACT GAAAGGCTGT GCTCTCAAAA CCCACCAGTC TTGAAACGCC ATCAACGGGA AATAACTCGT ACTACTCTTC AGTCAGATCA AGAGGAAATT GACTATGATG ATACCATATC AGTTGAAATG AAGAAGGAAG ATTTTGACAT TTATGATGAG GATGAAAATC AGAGCCCCCG CAGCTTTCAA AAGAAAACAC GACACTATTT TATTGCTGCA GTGGAGAGGC TCTGGGATTA TGGGATGAGT AGCTCCCCAC ATGTTCTAAG AAACAGGGCT CAGAGTGGCA GTGTCCCTCA GTTCAAGAAA GTTGTTTTCC AGGAATTTAC TGATGGCTCC TTTACTCAGC CCTTATACCG TGGAGAACTA AATGAACATT TGGGACTCCT GGGGCCATAT ATAAGAGCAG AAGTTGAAGA TAATATCATG GTAACTTTCA GAAATCAGGC CTCTCGTCCC TATTCCTTCT ATTCTAGCCT TATTTCTTAT GAGGAAGATC AGAGGCAAGG AGCAGAACCT AGAAAAAACT TTGTCAAGCC TAATGAAACC AAAACTTACT TTTGGAAAGT GCAACATCAT ATGGCACCCA CTAAAGATGA GTTTGACTGC AAAGCCTGGG CTTATTTCTC TGATGTTGAC CTGGAAAAAG ATGTGCACTC AGGCCTGATT GGACCCCTTC TGGTCTGCCA CACTAACACA CTGAACCCTG CTCATGGGAG ACAAGTGACA GTACAGGAAT TTGCTCTGTT TTTCACCATC TTTGATGAGA CCAAAAGCTG GTACTTCACT GAAAATATGG AAAGAAACTG CAGGGCTCCC TGCAATATCC AGATGGAAGA TCCCACTTTT AAAGAGAATT ATCGCTTCCA TGCAATCAAT GGCTACATAA TGGATACACT ACCTGGCTTA GTAATGGCTC AGGATCAAAG GATTCGATGG TATCTGCTCA GCATGGGCAG CAATGAAAAC ATCCATTCTA TTCATTTCAG TGGACATGTG TTCACTGTAC GAAAAAAAGA GGAGTATAAA ATGGCACTGT ACAATCTCTA TCCAGGTGTT TTTGAGACAG TGGAAATGTT ACCATCCAAA GCTGGAATTT GGCGGGTGGA ATGCCTTATT GGCGAGCATC TACATGCTGG GATGAGCACA CTTTTTCTGG TGTACAGCAA TAAGTGTCAG ACTCCCCTGG GAATGGCTTC TGGACACATT AGAGATTTTC AGATTACAGC TTCAGGACAA TATGGACAGT GGGCCCCAAA GCTGGCCAGA CTTCATTATT CCGGATCAAT CAATGCCTGG AGCACCAAGG AGCCCTTTTC TTGGATCAAG GTGGATCTGT TGGCACCAAT GATTATTCAC GGCATCAAGA CCCAGGGTGC CCGTCAGAAG TTCTCCAGCC TCTACATCTC TCAGTTTATC ATCATGTATA GTCTTGATGG GAAGAAGTGG CAGACTTATC GAGGAAATTC CACTGGAACC TTAATGGTCT TCTTTGGCAA TGTGGATTCA TCTGGGATAA AACACAATAT TTTTAACCCT CCAATTATTG CTCGATACAT CCGTTTGCAC CCAACTCATT ATAGCATTCG CAGCACTCTT CGCATGGAGT TGATGGGCTG TGATTTAAAT AGTTGCAGCA TGCCATTGGG AATGGAGAGT AAAGCAATAT CAGATGCACA GATTACTGCT TCATCCTACT TTACCAATAT GTTTGCCACC TGGTCTCCTT CAAAAGCTCG ACTTCACCTC CAAGGGAGGA GTAATGCCTG GAGACCTCAG GTGAATAATC CAAAAGAGTG GCTGCAAGTG GACTTCCAGA AGACAATGAA AGTCACAGGA GTAACTACTC AGGGAGTAAA ATCTCTGCTT ACCAGCATGT ATGTGAAGGA GTTCCTCATC TCCAGCAGTC AAGATGGCCA TCAGTGGACT CTCTTTTTTC AGAATGGCAA AGTAAAGGTT TTTCAGGGAA ATCAAGACTC CTTCACACCT GTGGTGAACT CTCTAGACCC ACCGTTACTG ACTCGCTACC TTCGAATTCA CCCCCAGAGT TGGGTGCACC AGATTGCCCT GAGGATGGAG GTTCTGGGCT GCGAGGCACA GGACCTCTAC GACAAAACTC ACACATGCCC ACCGTGCCCA GCTCCAGAAC TCCTGGGCGG ACCGTCAGTC TTCCTCTTCC CCCCAAAACC CAAGGACACC CTCATGATCT CCCGGACCCC TGAGGTCACA TGCGTGGTGG TGGACGTGAG CCACGAAGAC CCTGAGGTCA AGTTCAACTG GTACGTGGAC GGCGTGGAGG TGCATAATGC CAAGACAAAG CCGCGGGAGG AGCAGTACAA CAGCACGTAC CGTGTGGTCA GCGTCCTCAC CGTCCTGCAC CAGGACTGGC TGAATGGCAA GGAGTACAAG TGCAAGGTCT CCAACAAAGC CCTCCCAGCC CCCATCGAGA AAACCATCTC CAAAGCCAAA GGGCAGCCCC GAGAACCACA GGTGTACACC CTGCCCCCAT CCCGGGATGA GCTGACCAAG AACCAGGTCA GCCTGACCTG CCTGGTCAAA GGCTTCTATC CCAGCGACAT CGCCGTGGAG TGGGAGAGCA ATGGGCAGCC GGAGAACAAC TACAAGACCA CGCCTCCCGT GTTGGACTCC GACGGCTCCT TCTTCCTCTA CAGCAAGCTC ACCGTGGACA AGAGCAGGTG GCAGCAGGGG AACGTCTTCT CATGCTCCGT GATGCATGAG GCTCTGCACA ACCACTACAC GCAGAAGAGC CTCTCCCTGT CTCCGGGTAA A (ii) Fc (same sequence as A (ii) (SEQ ID NO: 7))]
TABLE-US-00040 TABLE 40 FVIII Polypeptide Sequences A. B-Domain Deleted FVIII-Fc Monomer Hybrid (BDD FVIIIFc monomer dimer): created by coexpressing BDD FVIIIFc and Fc chains. Construct = HC-LC-Fc fusion. An Fc expression cassette is cotransfected with BDDFVIII-Fc to generate the BDD FVIIIFc monomer-. For the BDD FVIIIFc chain, the Fc sequence is shown in bold; HC sequence is shown in double underline; remaining B domain sequence is shown in italics. Signal peptides are underlined. i) B domain deleted FVIII-Fc chain (19 amino acid signal sequence underlined) (SEQ ID NO: 6) MQIELSTCFFLCLLRFCFS ATRRYYLGAVELSWDYMQSDLGELPVDARFPPRVPKSFPFNTSVVYKKTLFVEFTDHLF NIAKPRPPWMGLLGPTIQAEVYDTVVITLKNMASHPVSLHAVGVSYWKASEGAEYDDQ TSQREKEDDKVFPGGSHTYVWQVLKENGPMASDPLCLTYSYLSHVDLVKDLNSGLIGA LLVCREGSLAKEKTQTLHKFILLFAVFDEGKSWHSETKNSLMQDRDAASARAWPKMHT VNGYVNRSLPGLIGCHRKSVYWHVIGMGTTPEVHSIFLEGHTFLVRNHRQASLEISPITFL TAQTLLMDLGQFLLFCHISSHQHDGMEAYVKVDSCPEEPQLRMKNNEEAEDYDDDLTD SEMDVVRFDDDNSPSFIQIRSVAKKHPKTWVHYIAAEEEDWDYAPLVLAPDDRSYKSQY LNNGPQRIGRKYKKVRFMAYTDETFKTREAIQHESGILGPLLYGEVGDTLLIIFKNQASRP YNIYPHGITDVRPLYSRRLPKGVKHLKDFPILPGEIFKYKWTVTVEDGPTKSDPRCLTRY YSSFVNMERDLASGLIGPLLICYKESVDQRGNQIMSDKRNVILFSVFDENRSWYLTENIQ RFLPNPAGVQLEDPEFQASNIMHSINGYVFDSLQLSVCLHEVAYWYILSIGAQTDFLSVFF SGYTFKHKMVYEDTLTLFPFSGETVFMSMENPGLWILGCHNSDFRNRGMTALLKVSSC DKNTGDYYEDSYEDISAYLLSKNNAIEPRSFSQNPPVLKRHQREITRTTLQSDQEEIDYDD TISVEMKKEDFDIYDEDENQSPRSFQKKTRHYFIAAVERLWDYGMSSSPHVLRNRAQSG SVPQFKKVVFQEFTDGSFTQPLYRGELNEHLGLLGPYIRAEVEDNIMVTFRNQASRPYSF YSSLISYEEDQRQGAEPRKNFVKPNETKTYFWKVQHHMAPTKDEFDCKAWAYFSDVDL EKDVHSGLIGPLLVCHTNTLNPAHGRQVTVQEFALFFTIFDETKSWYFTENMERNCRAP CNIQMEDPTFKENYRFHAINGYIMDTLPGLVMAQDQRIRWYLLSMGSNENIHSIHFSGH VFTVRKKEEYKMALYNLYPGVFETVEMLPSKAGIWRVECLIGEHLHAGMSTLFLVYSN KCQTPLGMASGHIRDFQITASGQYGQWAPKLARLHYSGSINAWSTKEPFSWIKVDLLAP MIIHGIKTQGARQKFSSLYISQFIIMYSLDGKKWQTYRGNSTGTLMVFFGNVDSSGIKHNI FNPPIIARYIRLHPTHYSIRSTLRMELMGCDLNSCSMPLGMESKAISDAQITASSYFTNMF ATWSPSKARLHLQGRSNAWRPQVNNPKEWLQVDFQKTMKVTGVTTQGVKSLLTSMY VKEFLISSSQDGHQWTLFFQNGKVKVFQGNQDSFTPVVNSLDPPLLTRYLRIHPQSWVH QIALRMEVLGCEAQDLYDKTHTCPPCPAPELLGGPSVFLFPPKPKDTLMISRTPEVTC VVVDVSHEDPEVKFNWYVDGVEVHNAKTKPREEQYNSTYRYVSVLTVLHQDWLN GKEYKCKVSNKALPAPIEKTISKAKGQPREPQVYTLPPSRDELTKNQVSLTCLVKG FYPSDIAVEWESNGQPENNYKTTPPVLDSDGSFFLYSKLTVDKSRWQQGNVFSCSV MHEALHNHYTQKSLSLSPGK ii) Fc chain (20 amino acid heterologous signal peptide from mouse IgK.kappa. chain underlined) (SEQ ID NO: 8) METDTLLLWVLLLWVPGSTG DKTHTCPPCPAPELLGGPSVFLFPPKPKDTLMISRTPEVTCVVVDVSHEDPEVKFNWYVD GVEVHNAKTKPREEQYNSTYRVVSVLTVLHQDWLNGKEYKCKVSNKALPAPIEKTISK AKGQPREPQVYTLPPSRDELTKNQVSLTCLVKGFYPSDIAVEWESNGQPENNYKTTPPV LDSDGSFFLYSKLTVDKSRWQQGNVFSCSVMHEALHNHYTQKSLSLSPGK B. Full length FVIIIFc monomer hybrid (Full length FVIIIFc monomer dimer): created by coexpressing FVIIIFc and Fc chains. Construct = HC-B-LC-Fc fusion. An Fc expression cassette is cotransfected with full length FVIII-Fc to generate the full length FVIIIFc monomer. For the FVIIIFc chain, the Fc sequence is shown in bold; HC sequence is shown in double underline; B domain sequence is shown in italics. Signal peptides are underlined. i) Full length FVIIIFc chain (FVIII signal peptide underlined (SEQ ID NO: 10) MQIELSTCFFLCLLRFCFS ATRRYYLGAVELSWDYMQSDLGELPVDARFPPRVPKSFPFNTSVVYKKTLFVEFTDHLF NIAKPRPPWMGLLGPTIQAEVYDTVVITLKNMASHPVSLHAVGVSYWKASEGAEYDDQ TSQREKEDDKVFPGGSHTYVWQVLKENGPMASDPLCLTYSYLSHVDLVKDLNSGLIGA LLVCREGSLAKEKTQTLHKFILLFAVFDEGKSWHSETKNSLMQDRDAASARAWPKMHT VNGYVNRSLPGLIGCHRKSVYWHVIGMGTTPEVHSIFLEGHTFLVRNHRQASLEISPITFL TAQTLLMDLGQFLLFCHISSHQHDGMEAYVKVDSCPEEPQLRMKNNEEAEDYDDDLTD SEMDVVRFDDDNSPSFIQIRSVAKKHPKTWVHYIAAEEEDWDYAPLVLAPDDRSYKSQY LNNGPQRIGRKYKKVRFMAYTDETFKTREAIQHESGILGPLLYGEVGDTLLIIFKNQASRP YNIYPHGITDVRPLYSRRLPKGVKHLKDFPILPGEIFKYKWTVTVEDGPTKSDPRCLTRY YSSFVNMERDLASGLIGPLLICYKESVDQRGNQIMSDKRNVILFSVFDENRSWYLTENIQ RFLPNPAGVQLEDPEFQASNIMHSINGYVFDSLQLSVCLHEVAYWYILSIGAQTDFLSVFF SGYTFKHKMVYEDTLTLFPFSGETVFMSMENPGLWILGCHNSDFRNRGMTALLKVSSC DKNTGDYYEDSYEDISAYLLSKNNAIEPRSFSQNSRHPSTRQKQFNATTIPENDIEKTDPWF AHRTPMPKIQNVSSSDLLMLLRQSPTPHGLSLSDLQEAKYETESDDPSPGAIDSNNSLSEMTHE RPQLHHSGDMVETPESGLQLRLNEKLGTTAATELKKLDEKVSSTSNNLISTIPSDNLAAGTDNT SSLGPPSMPVHYDSQLDTTLFGKKSSPLTESGGPLSLSEENNDSKLLESGLMNSQESSWGKNV SSTESGRLFKGKRAHGPALLTKDNALFKVSISLLKTNKTSNNSATNRKTHIDGPSLLIENSPSVW QNILESDTEFKKVTPLIHDRAILMDKNATALRLNHMSNKTTSSKNMEMYQQKKEGPIPPDAQN PDMSFFICMLFLPESARWIQRTHGKNSLNSGQGPSPKQLVSLGPEKSVEGQNFLSEKNKVVVG KGEFTKDVGLKEIVIVEPSSRNLFLTNLDNLHENNTHNQEKKIQEETEKKETLIQENVVLPQIHT VTGTKNFMKNLELLSTRQNVEGSYDGAYAPVLQDFRSLNDSTNRTKKHTAHFSKKGEEENLE GLGNQTKQIVEKYACTTRISPNTSQQNFVTQRSKRALKQERLPLEETELEKRIIVDDTSTQWSK NMKHLTPSTLTQIDYNEKEKGAITQSPLSDCLTRSHSIPQANRSPLPIAKVSSEPSIRPTYLTRVLF QDNSSHLPAASYRKKDSGVQESSHFLQGAKKNNLSLAILTLEMTGDQREVGSLGISATNSVTY KKVENTVLPKPDLPKTSGKVELLPKVHIYQKDLEPTETSNGSPGHLDLVEGSLLQGTEGAIKW NEANRPGKVPFLRVATESSAKTPSKLLDPLAWDNHYGTQIPKEEWKSQEKSPEKTAFKKKDTI LSLNACESNHAMAINEGQNKPEIEVTWAKQGRTERLCSQNPPVLKRHQREITRTTLQSDQEEI DYDDTISVEMKKEDFDIYDEDENQSPRSFQKKTRHYFIAAVERLWDYGMSSSPHVLRNR AQSGSVPQFKKVVFQEFTDGSFTQPLYRGELNEHLGLLGPYIRAEVEDNIMVTFRNQASR PYSFYSSLISYEEDQRQGAEPRKNFVKPNETKTYFWKVQHHMAPTKDEFDCKAWAYFS DVDLEKDVHSGLIGPLLVCHTNTLNPAHGRQVTVQEFALFFTIFDETKSWYFTENMERN CRAPCNIQMEDPTFKENYRFHAINGYIMDTLPGLVMAQDQRIRWYLLSMGSNENIHSIHF SGHVFTVRKKEEYKMALYNLYPGVFETVEMLPSKAGIWRVECLIGEHLHAGMSTLFLV YSNKCQTPLGMASGHIRDFQITASGQYGQWAPKLARLHYSGSINAWSTKEPFSWIKVDL LAPMIIHGIKTQGARQKFSSLYISQFIIMYSLDGKKWQTYRGNSTGTLMVFFGNVDSSGIK HNIFNPPIIARYIRLHPTHYSIRSTLRMELMGCDLNSCSMPLGMESKAISDAQITASSYFTN MFATWSPSKARLHLQGRSNAWRPQVNNPKEWLQVDFQKTMKVTGVTTQGVKSLLTS MYVKEFLISSSQDGHQWTLFFQNGKVKVFQGNQDSFTPVVNSLDPPLLTRYLRIHPQSW VHQIALRMEVLGCEAQDLYDKTHTCPPCPAPELLGGPSVFLFPPKPKDTLMISRTPEV TCVVVDVSHEDPEVKFNWYVDGVEVHNAKTKPREEQYNSTYRVVSVLTVLHQDW LNGKEYKCKVSNKALPAPIEKTISKAKGQPREPQVYTLPPSRDELTKNQVSLTCLV KGFYPSDIAVEWESNGQPENNYKTTPPVLDSDGSFFLYSKLTVDKSRWQQGNVFSC SVMHEALHNHYTQKSLSLSPGK ii) Fc chain (20 amino acid heterologous signal peptide from mouse ID (chain underlined) (SEQ ID NO: 8) METDTLLLWVLLLWVPGSTG DKTHTCPPCPAPELLGGPSVFLFPPKPKDTLMISRTPEVTCVVVDVSHEDPEVKFNWYVD GVEVHNAKTKPREEQYNSTYRVVSVLTVLHQDWLNGKEYKCKVSNKALPAPIEKTISK AKGQPREPQVYTLPPSRDELTKNQVSLTCLVKGFYPSDIAVEWESNGQPENNYKTTPPV LDSDGSFFLYSKLTVDKSRWQQGNVFSCSVMHEALHNHYTQKSLSLSPGK
Sequence CWU 1 SEQUENCE LISTING <160> NUMBER OF SEQ ID
NOS: 21 <210> SEQ ID NO 1 <211> LENGTH: 7583
<212> TYPE: DNA <213> ORGANISM: Artificial Sequence
<220> FEATURE: <223> OTHER INFORMATION: pSYN-FIX-030
<400> SEQUENCE: 1 gcgcgcgttg acattgatta ttgactagtt attaatagta
atcaattacg gggtcattag 60 ttcatagccc atatatggag ttccgcgtta
cataacttac ggtaaatggc ccgcctggct 120 gaccgcccaa cgacccccgc
ccattgacgt caataatgac gtatgttccc atagtaacgc 180 caatagggac
tttccattga cgtcaatggg tggagtattt acggtaaact gcccacttgg 240
cagtacatca agtgtatcat atgccaagta cgccccctat tgacgtcaat gacggtaaat
300 ggcccgcctg gcattatgcc cagtacatga ccttatggga ctttcctact
tggcagtaca 360 tctacgtatt agtcatcgct attaccatgg tgatgcggtt
ttggcagtac atcaatgggc 420 gtggatagcg gtttgactca cggggatttc
caagtctcca ccccattgac gtcaatggga 480 gtttgttttg gcaccaaaat
caacgggact ttccaaaatg tcgtaacaac tccgccccat 540 tgacgcaaat
gggcggtagg cgtgtacggt gggaggtcta tataagcaga gctctctggc 600
taactagaga acccactgct tactggctta tcgaaattaa tacgactcac tatagggaga
660 cccaagcttc gcgacgtacg gccgccacca tgcagcgcgt gaacatgatc
atggcagaat 720 caccaggcct catcaccatc tgccttttag gatatctact
cagtgctgaa tgtacaggtt 780 tgtttccttt tttaaaatac attgagtatg
cttgcctttt agatatagaa atatctgatg 840 ctgtcttctt cactaaattt
tgattacatg atttgacagc aatattgaag agtctaacag 900 ccagcacgca
ggttggtaag tactgtggga acatcacaga ttttggctcc atgccctaaa 960
gagaaattgg ctttcagatt atttggatta aaaacaaaga ctttcttaag agatgtaaaa
1020 ttttcatgat gttttctttt ttgctaaaac taaagaatta ttcttttaca
tttcagtttt 1080 tcttgatcat gaaaacgcca acaaaattct gaatcggcca
aagaggtata attcaggtaa 1140 attggaagag tttgttcaag ggaatctaga
gagagaatgt atggaagaaa agtgtagttt 1200 tgaagaagca cgagaagttt
ttgaaaacac tgaaagaaca actgaatttt ggaagcagta 1260 tgttgatgga
gatcagtgtg agtccaatcc atgtttaaat ggcggcagtt gcaaggatga 1320
cattaattcc tatgaatgtt ggtgtccctt tggatttgaa ggaaagaact gtgaattaga
1380 tgtaacatgt aacattaaga atggcagatg cgagcagttt tgtaaaaata
gtgctgataa 1440 caaggtggtt tgctcctgta ctgagggata tcgacttgca
gaaaaccaga agtcctgtga 1500 accagcagtg ccatttccat gtggaagagt
ttctgtttca caaacttcta agctcacccg 1560 tgctgagact gtttttcctg
atgtggacta tgtaaattct actgaagctg aaaccatttt 1620 ggataacatc
actcaaagca cccaatcatt taatgacttc actcgggttg ttggtggaga 1680
agatgccaaa ccaggtcaat tcccttggca ggttgttttg aatggtaaag ttgatgcatt
1740 ctgtggaggc tctatcgtta atgaaaaatg gattgtaact gctgcccact
gtgttgaaac 1800 tggtgttaaa attacagttg tcgcaggtga acataatatt
gaggagacag aacatacaga 1860 gcaaaagcga aatgtgattc gaattattcc
tcaccacaac tacaatgcag ctattaataa 1920 gtacaaccat gacattgccc
ttctggaact ggacgaaccc ttagtgctaa acagctacgt 1980 tacacctatt
tgcattgctg acaaggaata cacgaacatc ttcctcaaat ttggatctgg 2040
ctatgtaagt ggctggggaa gagtcttcca caaagggaga tcagctttag ttcttcagta
2100 ccttagagtt ccacttgttg accgagccac atgtcttcga tctacaaagt
tcaccatcta 2160 taacaacatg ttctgtgctg gcttccatga aggaggtaga
gattcatgtc aaggagatag 2220 tgggggaccc catgttactg aagtggaagg
gaccagtttc ttaactggaa ttattagctg 2280 gggtgaagag tgtgcaatga
aaggcaaata tggaatatat accaaggtgt cccggtatgt 2340 caactggatt
aaggaaaaaa caaagctcac tgacaaaact cacacatgcc caccgtgccc 2400
agctccggaa ctcctgggcg gaccgtcagt cttcctcttc cccccaaaac ccaaggacac
2460 cctcatgatc tcccggaccc ctgaggtcac atgcgtggtg gtggacgtga
gccacgaaga 2520 ccctgaggtc aagttcaact ggtacgtgga cggcgtggag
gtgcataatg ccaagacaaa 2580 gccgcgggag gagcagtaca acagcacgta
ccgtgtggtc agcgtcctca ccgtcctgca 2640 ccaggactgg ctgaatggca
aggagtacaa gtgcaaggtc tccaacaaag ccctcccagc 2700 ccccatcgag
aaaaccatct ccaaagccaa agggcagccc cgagaaccac aggtgtacac 2760
cctgccccca tcccgggatg agctgaccaa gaaccaggtc agcctgacct gcctggtcaa
2820 aggcttctat cccagcgaca tcgccgtgga gtgggagagc aatgggcagc
cggagaacaa 2880 ctacaagacc acgcctcccg tgttggactc cgacggctcc
ttcttcctct acagcaagct 2940 caccgtggac aagagcaggt ggcagcaggg
gaacgtcttc tcatgctccg tgatgcatga 3000 ggctctgcac aaccactaca
cgcagaagag cctctccctg tctccgggta aatgagaatt 3060 cagacatgat
aagatacatt gatgagtttg gacaaaccac aactagaatg cagtgaaaaa 3120
aatgctttat ttgtgaaatt tgtgatgcta ttgctttatt tgtaaccatt ataagctgca
3180 ataaacaagt tggggtgggc gaagaactcc agcatgagat ccccgcgctg
gaggatcatc 3240 cagccggcgt cccggaaaac gattccgaag cccaaccttt
catagaaggc ggcggtggaa 3300 tcgaaatctc gtagcacgtg tcagtcctgc
tcctcggcca cgaagtgcac gcagttgccg 3360 gccgggtcgc gcagggcgaa
ctcccgcccc cacggctgct cgccgatctc ggtcatggcc 3420 ggcccggagg
cgtcccggaa gttcgtggac acgacctccg accactcggc gtacagctcg 3480
tccaggccgc gcacccacac ccaggccagg gtgttgtccg gcaccacctg gtcctggacc
3540 gcgctgatga acagggtcac gtcgtcccgg accacaccgg cgaagtcgtc
ctccacgaag 3600 tcccgggaga acccgagccg gtcggtccag aactcgaccg
ctccggcgac gtcgcgcgcg 3660 gtgagcaccg gaacggcact ggtcaacttg
gccatggttt agttcctcac cttgtcgtat 3720 tatactatgc cgatatacta
tgccgatgat taattgtcaa cacgtgctga tcagatccga 3780 aaatggatat
acaagctccc gggagctttt tgcaaaagcc taggcctcca aaaaagcctc 3840
ctcactactt ctggaatagc tcagaggcag aggcggcctc ggcctctgca taaataaaaa
3900 aaattagtca gccatggggc ggagaatggg cggaactggg cggagttagg
ggcgggatgg 3960 gcggagttag gggcgggact atggttgctg actaattgag
atgcatgctt tgcatacttc 4020 tgcctgctgg ggagcctggg gactttccac
acctggttgc tgactaattg agatgcatgc 4080 tttgcatact tctgcctgct
ggggagcctg gggactttcc acaccctcgt cgagctagct 4140 tcgtgaggct
ccggtgcccg tcagtgggca gagcgcacat cgcccacagt ccccgagaag 4200
ttggggggag gggtcggcaa ttgaaccggt gcctagagaa ggtggcgcgg ggtaaactgg
4260 gaaagtgatg tcgtgtactg gctccgcctt tttcccgagg gtgggggaga
accgtatata 4320 agtgcagtag tcgccgtgaa cgttcttttt cgcaacgggt
ttgccgccag aacacaggta 4380 agtgccgtgt gtggttcccg cgggcctggc
ctctttacgg gttatggccc ttgcgtgcct 4440 tgaattactt ccacctggct
ccagtacgtg attcttgatc ccgagctgga gccaggggcg 4500 ggccttgcgc
tttaggagcc ccttcgcctc gtgcttgagt tgaggcctgg cctgggcgct 4560
ggggccgccg cgtgcgaatc tggtggcacc ttcgcgcctg tctcgctgct ttcgataagt
4620 ctctagccat ttaaaatttt tgatgacctg ctgcgacgct ttttttctgg
caagatagtc 4680 ttgtaaatgc gggccaggat ctgcacactg gtatttcggt
ttttggggcc gcgggcggcg 4740 acggggcccg tgcgtcccag cgcacatgtt
cggcgaggcg gggcctgcga gcgcggccac 4800 cgagaatcgg acgggggtag
tctcaagctg gccggcctgc tctggtgcct ggcctcgcgc 4860 cgccgtgtat
cgccccgccc tgggcggcaa ggctggcccg gtcggcacca gttgcgtgag 4920
cggaaagatg gccgcttccc ggccctgctc cagggggctc aaaatggagg acgcggcgct
4980 cgggagagcg ggcgggtgag tcacccacac aaaggaaagg ggcctttccg
tcctcagccg 5040 tcgcttcatg tgactccacg gagtaccggg cgccgtccag
gcacctcgat tagttctgga 5100 gcttttggag tacgtcgtct ttaggttggg
gggaggggtt ttatgcgatg gagtttcccc 5160 acactgagtg ggtggagact
gaagttaggc cagcttggca cttgatgtaa ttctccttgg 5220 aatttgccct
ttttgagttt ggatcttggt tcattctcaa gcctcagaca gtggttcaaa 5280
gtttttttct tccatttcag gtgtcgtgaa cacgtggtcg cggccgcgcc gccaccatgg
5340 agacagacac actcctgcta tgggtactgc tgctctgggt tccaggttcc
actggtgaca 5400 aaactcacac atgcccaccg tgcccagcac ctgaactcct
gggaggaccg tcagtcttcc 5460 tcttcccccc aaaacccaag gacaccctca
tgatctcccg gacccctgag gtcacatgcg 5520 tggtggtgga cgtgagccac
gaagaccctg aggtcaagtt caactggtac gtggacggcg 5580 tggaggtgca
taatgccaag acaaagccgc gggaggagca gtacaacagc acgtaccgtg 5640
tggtcagcgt cctcaccgtc ctgcaccagg actggctgaa tggcaaggag tacaagtgca
5700 aggtctccaa caaagccctc ccagccccca tcgagaaaac catctccaaa
gccaaagggc 5760 agccccgaga accacaggtg tacaccctgc ccccatcccg
cgatgagctg accaagaacc 5820 aggtcagcct gacctgcctg gtcaaaggct
tctatcccag cgacatcgcc gtggagtggg 5880 agagcaatgg gcagccggag
aacaactaca agaccacgcc tcccgtgttg gactccgacg 5940 gctccttctt
cctctacagc aagctcaccg tggacaagag caggtggcag caggggaacg 6000
tcttctcatg ctccgtgatg catgaggctc tgcacaacca ctacacgcag aagagcctct
6060 ccctgtctcc gggtaaatga ctcgagagat ctggccggct gggcccgttt
cgaaggtaag 6120 cctatcccta accctctcct cggtctcgat tctacgcgta
ccggtcatca tcaccatcac 6180 cattgagttt aaacccgctg atcagcctcg
actgtgcctt ctagttgcca gccatctgtt 6240 gtttgcccct cccccgtgcc
ttccttgacc ctggaaggtg ccactcccac tgtcctttcc 6300 taataaaatg
aggaaattgc atcgcattgt ctgagtaggt gtcattctat tctggggggt 6360
ggggtggggc aggacagcaa gggggaggat tgggaagaca atagcaggca tgctggggat
6420 gcggtgggct ctatggcttc tgaggcggaa agaaccagtg gcggtaatac
ggttatccac 6480 agaatcaggg gataacgcag gaaagaacat gtgagcaaaa
ggccagcaaa aggccaggaa 6540 ccgtaaaaag gccgcgttgc tggcgttttt
ccataggctc cgcccccctg acgagcatca 6600 caaaaatcga cgctcaagtc
agaggtggcg aaacccgaca ggactataaa gataccaggc 6660 gtttccccct
agaagctccc tcgtgcgctc tcctgttccg accctgccgc ttaccggata 6720
cctgtccgcc tttctccctt cgggaagcgt ggcgctttct catagctcac gctgtaggta
6780 tctcagttcg gtgtaggtcg ttcgctccaa gctgggctgt gtgcacgaac
cccccgttca 6840 gcccgaccgc tgcgccttat ccggtaacta tcgtcttgag
tccaacccgg taagacacga 6900 cttatcgcca ctggcagcag ccactggtaa
caggattagc agagcgaggt atgtaggcgg 6960 tgctacagag ttcttgaagt
ggtggcctaa ctacggctac actagaagaa cagtatttgg 7020 tatctgcgct
ctgctgaagc cagttacctt cggaaaaaga gttggtagct cttgatccgg 7080
caaacaaacc accgctggta gcggtggttt ttttgtttgc aagcagcaga ttacgcgcag
7140 aaaaaaagga tctcaagaag atcctttgat cttttctacg gggtctgacg
ctcagtggaa 7200 cgaaaactca cgttaaggga ttttggtcat gacattaacc
tataaaaata ggcgtatcac 7260 gaggcccttt cgtctcgcgc gtttcggtga
tgacggtgaa aacctctgac acatgcagct 7320 cccggagacg gtcacagctt
gtctgtaagc ggatgccggg agcagacaag cccgtcaggg 7380 cgcgtcagcg
ggtgttggcg ggtgtcgggg ctggcttaac tatgcggcat cagagcagat 7440
tgtactgaga gtgcaccata tatgcggtgt gaaataccgc acagatgcgt aaggagaaaa
7500 taccgcatca ggcgccattc gccattcagg ctgcgcaact gttgggaagg
gcgatcggtg 7560 cgggcctctt cgctattacg cca 7583 <210> SEQ ID
NO 2 <211> LENGTH: 688 <212> TYPE: PRT <213>
ORGANISM: Artificial Sequence <220> FEATURE: <223>
OTHER INFORMATION: pSYN-FIX-030 <220> FEATURE: <221>
NAME/KEY: SIGNAL <222> LOCATION: (-46)..(-19) 220>
<221> NAME/KEY: SIGNAL <222> LOCATION: (-18)..(-1)
<220> FEATURE: <221> NAME/KEY: mat_peptide <222>
LOCATION: (1)..(642) <400> SEQUENCE: 2 Met Gln Arg Val Asn
Met Ile Met Ala Glu Ser Pro Gly Leu Ile Thr -45 -40 -35 Ile Cys Leu
Leu Gly Tyr Leu Leu Ser Ala Glu Cys Thr Val Phe Leu -30 -25 -20 -15
Asp His Glu Asn Ala Asn Lys Ile Leu Asn Arg Pro Lys Arg Tyr Asn -10
-5 -1 1 Ser Gly Lys Leu Glu Glu Phe Val Gln Gly Asn Leu Glu Arg Glu
Cys 5 10 15 Met Glu Glu Lys Cys Ser Phe Glu Glu Ala Arg Glu Val Phe
Glu Asn 20 25 30 Thr Glu Arg Thr Thr Glu Phe Trp Lys Gln Tyr Val
Asp Gly Asp Gln 35 40 45 50 Cys Glu Ser Asn Pro Cys Leu Asn Gly Gly
Ser Cys Lys Asp Asp Ile 55 60 65 Asn Ser Tyr Glu Cys Trp Cys Pro
Phe Gly Phe Glu Gly Lys Asn Cys 70 75 80 Glu Leu Asp Val Thr Cys
Asn Ile Lys Asn Gly Arg Cys Glu Gln Phe 85 90 95 Cys Lys Asn Ser
Ala Asp Asn Lys Val Val Cys Ser Cys Thr Glu Gly 100 105 110 Tyr Arg
Leu Ala Glu Asn Gln Lys Ser Cys Glu Pro Ala Val Pro Phe 115 120 125
130 Pro Cys Gly Arg Val Ser Val Ser Gln Thr Ser Lys Leu Thr Arg Ala
135 140 145 Glu Thr Val Phe Pro Asp Val Asp Tyr Val Asn Ser Thr Glu
Ala Glu 150 155 160 Thr Ile Leu Asp Asn Ile Thr Gln Ser Thr Gln Ser
Phe Asn Asp Phe 165 170 175 Thr Arg Val Val Gly Gly Glu Asp Ala Lys
Pro Gly Gln Phe Pro Trp 180 185 190 Gln Val Val Leu Asn Gly Lys Val
Asp Ala Phe Cys Gly Gly Ser Ile 195 200 205 210 Val Asn Glu Lys Trp
Ile Val Thr Ala Ala His Cys Val Glu Thr Gly 215 220 225 Val Lys Ile
Thr Val Val Ala Gly Glu His Asn Ile Glu Glu Thr Glu 230 235 240 His
Thr Glu Gln Lys Arg Asn Val Ile Arg Ile Ile Pro His His Asn 245 250
255 Tyr Asn Ala Ala Ile Asn Lys Tyr Asn His Asp Ile Ala Leu Leu Glu
260 265 270 Leu Asp Glu Pro Leu Val Leu Asn Ser Tyr Val Thr Pro Ile
Cys Ile 275 280 285 290 Ala Asp Lys Glu Tyr Thr Asn Ile Phe Leu Lys
Phe Gly Ser Gly Tyr 295 300 305 Val Ser Gly Trp Gly Arg Val Phe His
Lys Gly Arg Ser Ala Leu Val 310 315 320 Leu Gln Tyr Leu Arg Val Pro
Leu Val Asp Arg Ala Thr Cys Leu Arg 325 330 335 Ser Thr Lys Phe Thr
Ile Tyr Asn Asn Met Phe Cys Ala Gly Phe His 340 345 350 Glu Gly Gly
Arg Asp Ser Cys Gln Gly Asp Ser Gly Gly Pro His Val 355 360 365 370
Thr Glu Val Glu Gly Thr Ser Phe Leu Thr Gly Ile Ile Ser Trp Gly 375
380 385 Glu Glu Cys Ala Met Lys Gly Lys Tyr Gly Ile Tyr Thr Lys Val
Ser 390 395 400 Arg Tyr Val Asn Trp Ile Lys Glu Lys Thr Lys Leu Thr
Asp Lys Thr 405 410 415 His Thr Cys Pro Pro Cys Pro Ala Pro Glu Leu
Leu Gly Gly Pro Ser 420 425 430 Val Phe Leu Phe Pro Pro Lys Pro Lys
Asp Thr Leu Met Ile Ser Arg 435 440 445 450 Thr Pro Glu Val Thr Cys
Val Val Val Asp Val Ser His Glu Asp Pro 455 460 465 Glu Val Lys Phe
Asn Trp Tyr Val Asp Gly Val Glu Val His Asn Ala 470 475 480 Lys Thr
Lys Pro Arg Glu Glu Gln Tyr Asn Ser Thr Tyr Arg Val Val 485 490 495
Ser Val Leu Thr Val Leu His Gln Asp Trp Leu Asn Gly Lys Glu Tyr 500
505 510 Lys Cys Lys Val Ser Asn Lys Ala Leu Pro Ala Pro Ile Glu Lys
Thr 515 520 525 530 Ile Ser Lys Ala Lys Gly Gln Pro Arg Glu Pro Gln
Val Tyr Thr Leu 535 540 545 Pro Pro Ser Arg Asp Glu Leu Thr Lys Asn
Gln Val Ser Leu Thr Cys 550 555 560 Leu Val Lys Gly Phe Tyr Pro Ser
Asp Ile Ala Val Glu Trp Glu Ser 565 570 575 Asn Gly Gln Pro Glu Asn
Asn Tyr Lys Thr Thr Pro Pro Val Leu Asp 580 585 590 Ser Asp Gly Ser
Phe Phe Leu Tyr Ser Lys Leu Thr Val Asp Lys Ser 595 600 605 610 Arg
Trp Gln Gln Gly Asn Val Phe Ser Cys Ser Val Met His Glu Ala 615 620
625 Leu His Asn His Tyr Thr Gln Lys Ser Leu Ser Leu Ser Pro Gly Lys
630 635 640 <210> SEQ ID NO 3 <211> LENGTH: 741
<212> TYPE: DNA <213> ORGANISM: Artificial Sequence
<220> FEATURE: <223> OTHER INFORMATION: Fc cassette
from pSYN-FIX-030 <400> SEQUENCE: 3 atggagacag acacactcct
gctatgggta ctgctgctct gggttccagg ttccactggt 60 gacaaaactc
acacatgccc accgtgccca gcacctgaac tcctgggagg accgtcagtc 120
ttcctcttcc ccccaaaacc caaggacacc ctcatgatct cccggacccc tgaggtcaca
180 tgcgtggtgg tggacgtgag ccacgaagac cctgaggtca agttcaactg
gtacgtggac 240 ggcgtggagg tgcataatgc caagacaaag ccgcgggagg
agcagtacaa cagcacgtac 300 cgtgtggtca gcgtcctcac cgtcctgcac
caggactggc tgaatggcaa ggagtacaag 360 tgcaaggtct ccaacaaagc
cctcccagcc cccatcgaga aaaccatctc caaagccaaa 420 gggcagcccc
gagaaccaca ggtgtacacc ctgcccccat cccgcgatga gctgaccaag 480
aaccaggtca gcctgacctg cctggtcaaa ggcttctatc ccagcgacat cgccgtggag
540 tgggagagca atgggcagcc ggagaacaac tacaagacca cgcctcccgt
gttggactcc 600 gacggctcct tcttcctcta cagcaagctc accgtggaca
agagcaggtg gcagcagggg 660 aacgtcttct catgctccgt gatgcatgag
gctctgcaca accactacac gcagaagagc 720 ctctccctgt ctccgggtaa a 741
<210> SEQ ID NO 4 <211> LENGTH: 247 <212> TYPE:
PRT <213> ORGANISM: Artificial Sequence <220> FEATURE:
<223> OTHER INFORMATION: Fc cassette from pSYN-FIX-030
<220> FEATURE: <221> NAME/KEY: SIGNAL <222>
LOCATION: (-20)..(-1) <220> FEATURE: <221> NAME/KEY:
mat_peptide <222> LOCATION: (1)..(227) <400> SEQUENCE:
4 Met Glu Thr Asp Thr Leu Leu Leu Trp Val Leu Leu Leu Trp Val Pro
-20 -15 -10 -5 Gly Ser Thr Gly Asp Lys Thr His Thr Cys Pro Pro Cys
Pro Ala Pro -1 1 5 10 Glu Leu Leu Gly Gly Pro Ser Val Phe Leu Phe
Pro Pro Lys Pro Lys 15 20 25 Asp Thr Leu Met Ile Ser Arg Thr Pro
Glu Val Thr Cys Val Val Val 30 35 40 Asp Val Ser His Glu Asp Pro
Glu Val Lys Phe Asn Trp Tyr Val Asp 45 50 55 60 Gly Val Glu Val His
Asn Ala Lys Thr Lys Pro Arg Glu Glu Gln Tyr 65 70 75 Asn Ser Thr
Tyr Arg Val Val Ser Val Leu Thr Val Leu His Gln Asp 80 85 90 Trp
Leu Asn Gly Lys Glu Tyr Lys Cys Lys Val Ser Asn Lys Ala Leu 95 100
105 Pro Ala Pro Ile Glu Lys Thr Ile Ser Lys Ala Lys Gly Gln Pro Arg
110 115 120 Glu Pro Gln Val Tyr Thr Leu Pro Pro Ser Arg Asp Glu Leu
Thr Lys 125 130 135 140 Asn Gln Val Ser Leu Thr Cys Leu Val Lys Gly
Phe Tyr Pro Ser Asp 145 150 155 Ile Ala Val Glu Trp Glu Ser Asn Gly
Gln Pro Glu Asn Asn Tyr Lys 160 165 170 Thr Thr Pro Pro Val Leu Asp
Ser Asp Gly Ser Phe Phe Leu Tyr Ser 175 180 185 Lys Leu Thr Val Asp
Lys Ser Arg Trp Gln Gln Gly Asn Val Phe Ser 190 195 200 Cys Ser Val
Met His Glu Ala Leu His Asn His Tyr Thr Gln Lys Ser 205 210 215 220
Leu Ser Leu Ser Pro Gly Lys 225 <210> SEQ ID NO 5 <211>
LENGTH: 5052 <212> TYPE: DNA <213> ORGANISM: Artificial
Sequence <220> FEATURE: <223> OTHER INFORMATION:
B-Domain Deleted FVIIIFc <400> SEQUENCE: 5 atgcaaatag
agctctccac ctgcttcttt ctgtgccttt tgcgattctg ctttagtgcc 60
accagaagat actacctggg tgcagtggaa ctgtcatggg actatatgca aagtgatctc
120 ggtgagctgc ctgtggacgc aagatttcct cctagagtgc caaaatcttt
tccattcaac 180 acctcagtcg tgtacaaaaa gactctgttt gtagaattca
cggatcacct tttcaacatc 240 gctaagccaa ggccaccctg gatgggtctg
ctaggtccta ccatccaggc tgaggtttat 300 gatacagtgg tcattacact
taagaacatg gcttcccatc ctgtcagtct tcatgctgtt 360 ggtgtatcct
actggaaagc ttctgaggga gctgaatatg atgatcagac cagtcaaagg 420
gagaaagaag atgataaagt cttccctggt ggaagccata catatgtctg gcaggtcctg
480 aaagagaatg gtccaatggc ctctgaccca ctgtgcctta cctactcata
tctttctcat 540 gtggacctgg taaaagactt gaattcaggc ctcattggag
ccctactagt atgtagagaa 600 gggagtctgg ccaaggaaaa gacacagacc
ttgcacaaat ttatactact ttttgctgta 660 tttgatgaag ggaaaagttg
gcactcagaa acaaagaact ccttgatgca ggatagggat 720 gctgcatctg
ctcgggcctg gcctaaaatg cacacagtca atggttatgt aaacaggtct 780
ctgccaggtc tgattggatg ccacaggaaa tcagtctatt ggcatgtgat tggaatgggc
840 accactcctg aagtgcactc aatattcctc gaaggtcaca catttcttgt
gaggaaccat 900 cgccaggcgt ccttggaaat ctcgccaata actttcctta
ctgctcaaac actcttgatg 960 gaccttggac agtttctact gttttgtcat
atctcttccc accaacatga tggcatggaa 1020 gcttatgtca aagtagacag
ctgtccagag gaaccccaac tacgaatgaa aaataatgaa 1080 gaagcggaag
actatgatga tgatcttact gattctgaaa tggatgtggt caggtttgat 1140
gatgacaact ctccttcctt tatccaaatt cgctcagttg ccaagaagca tcctaaaact
1200 tgggtacatt acattgctgc tgaagaggag gactgggact atgctccctt
agtcctcgcc 1260 cccgatgaca gaagttataa aagtcaatat ttgaacaatg
gccctcagcg gattggtagg 1320 aagtacaaaa aagtccgatt tatggcatac
acagatgaaa cctttaagac tcgtgaagct 1380 attcagcatg aatcaggaat
cttgggacct ttactttatg gggaagttgg agacacactg 1440 ttgattatat
ttaagaatca agcaagcaga ccatataaca tctaccctca cggaatcact 1500
gatgtccgtc ctttgtattc aaggagatta ccaaaaggtg taaaacattt gaaggatttt
1560 ccaattctgc caggagaaat attcaaatat aaatggacag tgactgtaga
agatgggcca 1620 actaaatcag atcctcggtg cctgacccgc tattactcta
gtttcgttaa tatggagaga 1680 gatctagctt caggactcat tggccctctc
ctcatctgct acaaagaatc tgtagatcaa 1740 agaggaaacc agataatgtc
agacaagagg aatgtcatcc tgttttctgt atttgatgag 1800 aaccgaagct
ggtacctcac agagaatata caacgctttc tccccaatcc agctggagtg 1860
cagcttgagg atccagagtt ccaagcctcc aacatcatgc acagcatcaa tggctatgtt
1920 tttgatagtt tgcagttgtc agtttgtttg catgaggtgg catactggta
cattctaagc 1980 attggagcac agactgactt cctttctgtc ttcttctctg
gatatacctt caaacacaaa 2040 atggtctatg aagacacact caccctattc
ccattctcag gagaaactgt cttcatgtcg 2100 atggaaaacc caggtctatg
gattctgggg tgccacaact cagactttcg gaacagaggc 2160 atgaccgcct
tactgaaggt ttctagttgt gacaagaaca ctggtgatta ttacgaggac 2220
agttatgaag atatttcagc atacttgctg agtaaaaaca atgccattga accaagaagc
2280 ttctctcaaa acccaccagt cttgaaacgc catcaacggg aaataactcg
tactactctt 2340 cagtcagatc aagaggaaat tgactatgat gataccatat
cagttgaaat gaagaaggaa 2400 gattttgaca tttatgatga ggatgaaaat
cagagccccc gcagctttca aaagaaaaca 2460 cgacactatt ttattgctgc
agtggagagg ctctgggatt atgggatgag tagctcccca 2520 catgttctaa
gaaacagggc tcagagtggc agtgtccctc agttcaagaa agttgttttc 2580
caggaattta ctgatggctc ctttactcag cccttatacc gtggagaact aaatgaacat
2640 ttgggactcc tggggccata tataagagca gaagttgaag ataatatcat
ggtaactttc 2700 agaaatcagg cctctcgtcc ctattccttc tattctagcc
ttatttctta tgaggaagat 2760 cagaggcaag gagcagaacc tagaaaaaac
tttgtcaagc ctaatgaaac caaaacttac 2820 ttttggaaag tgcaacatca
tatggcaccc actaaagatg agtttgactg caaagcctgg 2880 gcttatttct
ctgatgttga cctggaaaaa gatgtgcact caggcctgat tggacccctt 2940
ctggtctgcc acactaacac actgaaccct gctcatggga gacaagtgac agtacaggaa
3000 tttgctctgt ttttcaccat ctttgatgag accaaaagct ggtacttcac
tgaaaatatg 3060 gaaagaaact gcagggctcc ctgcaatatc cagatggaag
atcccacttt taaagagaat 3120 tatcgcttcc atgcaatcaa tggctacata
atggatacac tacctggctt agtaatggct 3180 caggatcaaa ggattcgatg
gtatctgctc agcatgggca gcaatgaaaa catccattct 3240 attcatttca
gtggacatgt gttcactgta cgaaaaaaag aggagtataa aatggcactg 3300
tacaatctct atccaggtgt ttttgagaca gtggaaatgt taccatccaa agctggaatt
3360 tggcgggtgg aatgccttat tggcgagcat ctacatgctg ggatgagcac
actttttctg 3420 gtgtacagca ataagtgtca gactcccctg ggaatggctt
ctggacacat tagagatttt 3480 cagattacag cttcaggaca atatggacag
tgggccccaa agctggccag acttcattat 3540 tccggatcaa tcaatgcctg
gagcaccaag gagccctttt cttggatcaa ggtggatctg 3600 ttggcaccaa
tgattattca cggcatcaag acccagggtg cccgtcagaa gttctccagc 3660
ctctacatct ctcagtttat catcatgtat agtcttgatg ggaagaagtg gcagacttat
3720 cgaggaaatt ccactggaac cttaatggtc ttctttggca atgtggattc
atctgggata 3780 aaacacaata tttttaaccc tccaattatt gctcgataca
tccgtttgca cccaactcat 3840 tatagcattc gcagcactct tcgcatggag
ttgatgggct gtgatttaaa tagttgcagc 3900 atgccattgg gaatggagag
taaagcaata tcagatgcac agattactgc ttcatcctac 3960 tttaccaata
tgtttgccac ctggtctcct tcaaaagctc gacttcacct ccaagggagg 4020
agtaatgcct ggagacctca ggtgaataat ccaaaagagt ggctgcaagt ggacttccag
4080 aagacaatga aagtcacagg agtaactact cagggagtaa aatctctgct
taccagcatg 4140 tatgtgaagg agttcctcat ctccagcagt caagatggcc
atcagtggac tctctttttt 4200 cagaatggca aagtaaaggt ttttcaggga
aatcaagact ccttcacacc tgtggtgaac 4260 tctctagacc caccgttact
gactcgctac cttcgaattc acccccagag ttgggtgcac 4320 cagattgccc
tgaggatgga ggttctgggc tgcgaggcac aggacctcta cgacaaaact 4380
cacacatgcc caccgtgccc agctccagaa ctcctgggcg gaccgtcagt cttcctcttc
4440 cccccaaaac ccaaggacac cctcatgatc tcccggaccc ctgaggtcac
atgcgtggtg 4500 gtggacgtga gccacgaaga ccctgaggtc aagttcaact
ggtacgtgga cggcgtggag 4560 gtgcataatg ccaagacaaa gccgcgggag
gagcagtaca acagcacgta ccgtgtggtc 4620 agcgtcctca ccgtcctgca
ccaggactgg ctgaatggca aggagtacaa gtgcaaggtc 4680 tccaacaaag
ccctcccagc ccccatcgag aaaaccatct ccaaagccaa agggcagccc 4740
cgagaaccac aggtgtacac cctgccccca tcccgggatg agctgaccaa gaaccaggtc
4800 agcctgacct gcctggtcaa aggcttctat cccagcgaca tcgccgtgga
gtgggagagc 4860 aatgggcagc cggagaacaa ctacaagacc acgcctcccg
tgttggactc cgacggctcc 4920 ttcttcctct acagcaagct caccgtggac
aagagcaggt ggcagcaggg gaacgtcttc 4980 tcatgctccg tgatgcatga
ggctctgcac aaccactaca cgcagaagag cctctccctg 5040 tctccgggta aa 5052
<210> SEQ ID NO 6 <211> LENGTH: 1684 <212> TYPE:
PRT <213> ORGANISM: Artificial Sequence <220> FEATURE:
<223> OTHER INFORMATION: B-Domain Deleted FVIIIFc <220>
FEATURE: <221> NAME/KEY: SIGNAL <222> LOCATION:
(-19)..(-1) <220> FEATURE: <221> NAME/KEY: mat_peptide
<222> LOCATION: (1)..(1665) <400> SEQUENCE: 6 Met Gln
Ile Glu Leu Ser Thr Cys Phe Phe Leu Cys Leu Leu Arg Phe -15 -10 -5
Cys Phe Ser Ala Thr Arg Arg Tyr Tyr Leu Gly Ala Val Glu Leu Ser -1
1 5 10 Trp Asp Tyr Met Gln Ser Asp Leu Gly Glu Leu Pro Val Asp Ala
Arg 15 20 25 Phe Pro Pro Arg Val Pro Lys Ser Phe Pro Phe Asn Thr
Ser Val Val 30 35 40 45 Tyr Lys Lys Thr Leu Phe Val Glu Phe Thr Asp
His Leu Phe Asn Ile 50 55 60 Ala Lys Pro Arg Pro Pro Trp Met Gly
Leu Leu Gly Pro Thr Ile Gln 65 70 75 Ala Glu Val Tyr Asp Thr Val
Val Ile Thr Leu Lys Asn Met Ala Ser 80 85 90 His Pro Val Ser Leu
His Ala Val Gly Val Ser Tyr Trp Lys Ala Ser 95 100 105 Glu Gly Ala
Glu Tyr Asp Asp Gln Thr Ser Gln Arg Glu Lys Glu Asp 110 115 120 125
Asp Lys Val Phe Pro Gly Gly Ser His Thr Tyr Val Trp Gln Val Leu 130
135 140 Lys Glu Asn Gly Pro Met Ala Ser Asp Pro Leu Cys Leu Thr Tyr
Ser 145 150 155 Tyr Leu Ser His Val Asp Leu Val Lys Asp Leu Asn Ser
Gly Leu Ile 160 165 170 Gly Ala Leu Leu Val Cys Arg Glu Gly Ser Leu
Ala Lys Glu Lys Thr 175 180 185 Gln Thr Leu His Lys Phe Ile Leu Leu
Phe Ala Val Phe Asp Glu Gly 190 195 200 205 Lys Ser Trp His Ser Glu
Thr Lys Asn Ser Leu Met Gln Asp Arg Asp 210 215 220 Ala Ala Ser Ala
Arg Ala Trp Pro Lys Met His Thr Val Asn Gly Tyr 225 230 235 Val Asn
Arg Ser Leu Pro Gly Leu Ile Gly Cys His Arg Lys Ser Val 240 245 250
Tyr Trp His Val Ile Gly Met Gly Thr Thr Pro Glu Val His Ser Ile 255
260 265 Phe Leu Glu Gly His Thr Phe Leu Val Arg Asn His Arg Gln Ala
Ser 270 275 280 285 Leu Glu Ile Ser Pro Ile Thr Phe Leu Thr Ala Gln
Thr Leu Leu Met 290 295 300 Asp Leu Gly Gln Phe Leu Leu Phe Cys His
Ile Ser Ser His Gln His 305 310 315 Asp Gly Met Glu Ala Tyr Val Lys
Val Asp Ser Cys Pro Glu Glu Pro 320 325 330 Gln Leu Arg Met Lys Asn
Asn Glu Glu Ala Glu Asp Tyr Asp Asp Asp 335 340 345 Leu Thr Asp Ser
Glu Met Asp Val Val Arg Phe Asp Asp Asp Asn Ser 350 355 360 365 Pro
Ser Phe Ile Gln Ile Arg Ser Val Ala Lys Lys His Pro Lys Thr 370 375
380 Trp Val His Tyr Ile Ala Ala Glu Glu Glu Asp Trp Asp Tyr Ala Pro
385 390 395 Leu Val Leu Ala Pro Asp Asp Arg Ser Tyr Lys Ser Gln Tyr
Leu Asn 400 405 410 Asn Gly Pro Gln Arg Ile Gly Arg Lys Tyr Lys Lys
Val Arg Phe Met 415 420 425 Ala Tyr Thr Asp Glu Thr Phe Lys Thr Arg
Glu Ala Ile Gln His Glu 430 435 440 445 Ser Gly Ile Leu Gly Pro Leu
Leu Tyr Gly Glu Val Gly Asp Thr Leu 450 455 460 Leu Ile Ile Phe Lys
Asn Gln Ala Ser Arg Pro Tyr Asn Ile Tyr Pro 465 470 475 His Gly Ile
Thr Asp Val Arg Pro Leu Tyr Ser Arg Arg Leu Pro Lys 480 485 490 Gly
Val Lys His Leu Lys Asp Phe Pro Ile Leu Pro Gly Glu Ile Phe 495 500
505 Lys Tyr Lys Trp Thr Val Thr Val Glu Asp Gly Pro Thr Lys Ser Asp
510 515 520 525 Pro Arg Cys Leu Thr Arg Tyr Tyr Ser Ser Phe Val Asn
Met Glu Arg 530 535 540 Asp Leu Ala Ser Gly Leu Ile Gly Pro Leu Leu
Ile Cys Tyr Lys Glu 545 550 555 Ser Val Asp Gln Arg Gly Asn Gln Ile
Met Ser Asp Lys Arg Asn Val 560 565 570 Ile Leu Phe Ser Val Phe Asp
Glu Asn Arg Ser Trp Tyr Leu Thr Glu 575 580 585 Asn Ile Gln Arg Phe
Leu Pro Asn Pro Ala Gly Val Gln Leu Glu Asp 590 595 600 605 Pro Glu
Phe Gln Ala Ser Asn Ile Met His Ser Ile Asn Gly Tyr Val 610 615 620
Phe Asp Ser Leu Gln Leu Ser Val Cys Leu His Glu Val Ala Tyr Trp 625
630 635 Tyr Ile Leu Ser Ile Gly Ala Gln Thr Asp Phe Leu Ser Val Phe
Phe 640 645 650 Ser Gly Tyr Thr Phe Lys His Lys Met Val Tyr Glu Asp
Thr Leu Thr 655 660 665 Leu Phe Pro Phe Ser Gly Glu Thr Val Phe Met
Ser Met Glu Asn Pro 670 675 680 685 Gly Leu Trp Ile Leu Gly Cys His
Asn Ser Asp Phe Arg Asn Arg Gly 690 695 700 Met Thr Ala Leu Leu Lys
Val Ser Ser Cys Asp Lys Asn Thr Gly Asp 705 710 715 Tyr Tyr Glu Asp
Ser Tyr Glu Asp Ile Ser Ala Tyr Leu Leu Ser Lys 720 725 730 Asn Asn
Ala Ile Glu Pro Arg Ser Phe Ser Gln Asn Pro Pro Val Leu 735 740 745
Lys Arg His Gln Arg Glu Ile Thr Arg Thr Thr Leu Gln Ser Asp Gln 750
755 760 765 Glu Glu Ile Asp Tyr Asp Asp Thr Ile Ser Val Glu Met Lys
Lys Glu 770 775 780 Asp Phe Asp Ile Tyr Asp Glu Asp Glu Asn Gln Ser
Pro Arg Ser Phe 785 790 795 Gln Lys Lys Thr Arg His Tyr Phe Ile Ala
Ala Val Glu Arg Leu Trp 800 805 810 Asp Tyr Gly Met Ser Ser Ser Pro
His Val Leu Arg Asn Arg Ala Gln 815 820 825 Ser Gly Ser Val Pro Gln
Phe Lys Lys Val Val Phe Gln Glu Phe Thr 830 835 840 845 Asp Gly Ser
Phe Thr Gln Pro Leu Tyr Arg Gly Glu Leu Asn Glu His 850 855 860 Leu
Gly Leu Leu Gly Pro Tyr Ile Arg Ala Glu Val Glu Asp Asn Ile 865 870
875 Met Val Thr Phe Arg Asn Gln Ala Ser Arg Pro Tyr Ser Phe Tyr Ser
880 885 890 Ser Leu Ile Ser Tyr Glu Glu Asp Gln Arg Gln Gly Ala Glu
Pro Arg 895 900 905 Lys Asn Phe Val Lys Pro Asn Glu Thr Lys Thr Tyr
Phe Trp Lys Val 910 915 920 925 Gln His His Met Ala Pro Thr Lys Asp
Glu Phe Asp Cys Lys Ala Trp 930 935 940 Ala Tyr Phe Ser Asp Val Asp
Leu Glu Lys Asp Val His Ser Gly Leu 945 950 955 Ile Gly Pro Leu Leu
Val Cys His Thr Asn Thr Leu Asn Pro Ala His 960 965 970 Gly Arg Gln
Val Thr Val Gln Glu Phe Ala Leu Phe Phe Thr Ile Phe 975 980 985 Asp
Glu Thr Lys Ser Trp Tyr Phe Thr Glu Asn Met Glu Arg Asn Cys 990 995
1000 1005 Arg Ala Pro Cys Asn Ile Gln Met Glu Asp Pro Thr Phe Lys
Glu 1010 1015 1020 Asn Tyr Arg Phe His Ala Ile Asn Gly Tyr Ile Met
Asp Thr Leu 1025 1030 1035 Pro Gly Leu Val Met Ala Gln Asp Gln Arg
Ile Arg Trp Tyr Leu 1040 1045 1050 Leu Ser Met Gly Ser Asn Glu Asn
Ile His Ser Ile His Phe Ser 1055 1060 1065 Gly His Val Phe Thr Val
Arg Lys Lys Glu Glu Tyr Lys Met Ala 1070 1075 1080 Leu Tyr Asn Leu
Tyr Pro Gly Val Phe Glu Thr Val Glu Met Leu 1085 1090 1095 Pro Ser
Lys Ala Gly Ile Trp Arg Val Glu Cys Leu Ile Gly Glu 1100 1105 1110
His Leu His Ala Gly Met Ser Thr Leu Phe Leu Val Tyr Ser Asn 1115
1120 1125 Lys Cys Gln Thr Pro Leu Gly Met Ala Ser Gly His Ile Arg
Asp 1130 1135 1140 Phe Gln Ile Thr Ala Ser Gly Gln Tyr Gly Gln Trp
Ala Pro Lys 1145 1150 1155 Leu Ala Arg Leu His Tyr Ser Gly Ser Ile
Asn Ala Trp Ser Thr 1160 1165 1170 Lys Glu Pro Phe Ser Trp Ile Lys
Val Asp Leu Leu Ala Pro Met 1175 1180 1185 Ile Ile His Gly Ile Lys
Thr Gln Gly Ala Arg Gln Lys Phe Ser 1190 1195 1200 Ser Leu Tyr Ile
Ser Gln Phe Ile Ile Met Tyr Ser Leu Asp Gly 1205 1210 1215 Lys Lys
Trp Gln Thr Tyr Arg Gly Asn Ser Thr Gly Thr Leu Met 1220 1225 1230
Val Phe Phe Gly Asn Val Asp Ser Ser Gly Ile Lys His Asn Ile 1235
1240 1245 Phe Asn Pro Pro Ile Ile Ala Arg Tyr Ile Arg Leu His Pro
Thr 1250 1255 1260 His Tyr Ser Ile Arg Ser Thr Leu Arg Met Glu Leu
Met Gly Cys 1265 1270 1275 Asp Leu Asn Ser Cys Ser Met Pro Leu Gly
Met Glu Ser Lys Ala 1280 1285 1290 Ile Ser Asp Ala Gln Ile Thr Ala
Ser Ser Tyr Phe Thr Asn Met 1295 1300 1305 Phe Ala Thr Trp Ser Pro
Ser Lys Ala Arg Leu His Leu Gln Gly 1310 1315 1320 Arg Ser Asn Ala
Trp Arg Pro Gln Val Asn Asn Pro Lys Glu Trp 1325 1330 1335 Leu Gln
Val Asp Phe Gln Lys Thr Met Lys Val Thr Gly Val Thr 1340 1345 1350
Thr Gln Gly Val Lys Ser Leu Leu Thr Ser Met Tyr Val Lys Glu 1355
1360 1365 Phe Leu Ile Ser Ser Ser Gln Asp Gly His Gln Trp Thr Leu
Phe 1370 1375 1380 Phe Gln Asn Gly Lys Val Lys Val Phe Gln Gly Asn
Gln Asp Ser 1385 1390 1395 Phe Thr Pro Val Val Asn Ser Leu Asp Pro
Pro Leu Leu Thr Arg 1400 1405 1410 Tyr Leu Arg Ile His Pro Gln Ser
Trp Val His Gln Ile Ala Leu 1415 1420 1425 Arg Met Glu Val Leu Gly
Cys Glu Ala Gln Asp Leu Tyr Asp Lys 1430 1435 1440 Thr His Thr Cys
Pro Pro Cys Pro Ala Pro Glu Leu Leu Gly Gly 1445 1450 1455 Pro Ser
Val Phe Leu Phe Pro Pro Lys Pro Lys Asp Thr Leu Met 1460 1465 1470
Ile Ser Arg Thr Pro Glu Val Thr Cys Val Val Val Asp Val Ser 1475
1480 1485 His Glu Asp Pro Glu Val Lys Phe Asn Trp Tyr Val Asp Gly
Val 1490 1495 1500 Glu Val His Asn Ala Lys Thr Lys Pro Arg Glu Glu
Gln Tyr Asn 1505 1510 1515 Ser Thr Tyr Arg Val Val Ser Val Leu Thr
Val Leu His Gln Asp 1520 1525 1530 Trp Leu Asn Gly Lys Glu Tyr Lys
Cys Lys Val Ser Asn Lys Ala 1535 1540 1545 Leu Pro Ala Pro Ile Glu
Lys Thr Ile Ser Lys Ala Lys Gly Gln 1550 1555 1560 Pro Arg Glu Pro
Gln Val Tyr Thr Leu Pro Pro Ser Arg Asp Glu 1565 1570 1575 Leu Thr
Lys Asn Gln Val Ser Leu Thr Cys Leu Val Lys Gly Phe 1580 1585 1590
Tyr Pro Ser Asp Ile Ala Val Glu Trp Glu Ser Asn Gly Gln Pro 1595
1600 1605 Glu Asn Asn Tyr Lys Thr Thr Pro Pro Val Leu Asp Ser Asp
Gly 1610 1615 1620 Ser Phe Phe Leu Tyr Ser Lys Leu Thr Val Asp Lys
Ser Arg Trp 1625 1630 1635 Gln Gln Gly Asn Val Phe Ser Cys Ser Val
Met His Glu Ala Leu 1640 1645 1650 His Asn His Tyr Thr Gln Lys Ser
Leu Ser Leu Ser Pro Gly Lys 1655 1660 1665 <210> SEQ ID NO 7
<211> LENGTH: 741 <212> TYPE: DNA <213> ORGANISM:
Artificial Sequence <220> FEATURE: <223> OTHER
INFORMATION: Fc Sequence <400> SEQUENCE: 7 atggagacag
acacactcct gctatgggta ctgctgctct gggttccagg ttccactggt 60
gacaaaactc acacatgccc accgtgccca gcacctgaac tcctgggagg accgtcagtc
120 ttcctcttcc ccccaaaacc caaggacacc ctcatgatct cccggacccc
tgaggtcaca 180 tgcgtggtgg tggacgtgag ccacgaagac cctgaggtca
agttcaactg gtacgtggac 240 ggcgtggagg tgcataatgc caagacaaag
ccgcgggagg agcagtacaa cagcacgtac 300 cgtgtggtca gcgtcctcac
cgtcctgcac caggactggc tgaatggcaa ggagtacaag 360 tgcaaggtct
ccaacaaagc cctcccagcc cccatcgaga aaaccatctc caaagccaaa 420
gggcagcccc gagaaccaca ggtgtacacc ctgcccccat cccgcgatga gctgaccaag
480 aaccaggtca gcctgacctg cctggtcaaa ggcttctatc ccagcgacat
cgccgtggag 540 tgggagagca atgggcagcc ggagaacaac tacaagacca
cgcctcccgt gttggactcc 600 gacggctcct tcttcctcta cagcaagctc
accgtggaca agagcaggtg gcagcagggg 660 aacgtcttct catgctccgt
gatgcatgag gctctgcaca accactacac gcagaagagc 720 ctctccctgt
ctccgggtaa a 741 <210> SEQ ID NO 8 <211> LENGTH: 247
<212> TYPE: PRT <213> ORGANISM: Artificial Sequence
<220> FEATURE: <223> OTHER INFORMATION: Fc chain
<220> FEATURE: <221> NAME/KEY: SIGNAL <222>
LOCATION: (-20)..(-1) <220> FEATURE: <221> NAME/KEY:
mat_peptide <222> LOCATION: (-1)..(227) <400> SEQUENCE:
8 Met Glu Thr Asp Thr Leu Leu Leu Trp Val Leu Leu Leu Trp Val Pro
-20 -15 -10 -5 Gly Ser Thr Gly Asp Lys Thr His Thr Cys Pro Pro Cys
Pro Ala Pro -1 1 5 10 Glu Leu Leu Gly Gly Pro Ser Val Phe Leu Phe
Pro Pro Lys Pro Lys 15 20 25 Asp Thr Leu Met Ile Ser Arg Thr Pro
Glu Val Thr Cys Val Val Val 30 35 40 Asp Val Ser His Glu Asp Pro
Glu Val Lys Phe Asn Trp Tyr Val Asp 45 50 55 60 Gly Val Glu Val His
Asn Ala Lys Thr Lys Pro Arg Glu Glu Gln Tyr 65 70 75 Asn Ser Thr
Tyr Arg Val Val Ser Val Leu Thr Val Leu His Gln Asp 80 85 90 Trp
Leu Asn Gly Lys Glu Tyr Lys Cys Lys Val Ser Asn Lys Ala Leu 95 100
105 Pro Ala Pro Ile Glu Lys Thr Ile Ser Lys Ala Lys Gly Gln Pro Arg
110 115 120 Glu Pro Gln Val Tyr Thr Leu Pro Pro Ser Arg Asp Glu Leu
Thr Lys 125 130 135 140 Asn Gln Val Ser Leu Thr Cys Leu Val Lys Gly
Phe Tyr Pro Ser Asp 145 150 155 Ile Ala Val Glu Trp Glu Ser Asn Gly
Gln Pro Glu Asn Asn Tyr Lys 160 165 170 Thr Thr Pro Pro Val Leu Asp
Ser Asp Gly Ser Phe Phe Leu Tyr Ser 175 180 185 Lys Leu Thr Val Asp
Lys Ser Arg Trp Gln Gln Gly Asn Val Phe Ser 190 195 200 Cys Ser Val
Met His Glu Ala Leu His Asn His Tyr Thr Gln Lys Ser 205 210 215 220
Leu Ser Leu Ser Pro Gly Lys 225 <210> SEQ ID NO 9 <211>
LENGTH: 7734 <212> TYPE: DNA <213> ORGANISM: Artificial
Sequence <220> FEATURE: <223> OTHER INFORMATION: Full
Length FVIIIFc <400> SEQUENCE: 9 atgcaaatag agctctccac
ctgcttcttt ctgtgccttt tgcgattctg ctttagtgcc 60 accagaagat
actacctggg tgcagtggaa ctgtcatggg actatatgca aagtgatctc 120
ggtgagctgc ctgtggacgc aagatttcct cctagagtgc caaaatcttt tccattcaac
180 acctcagtcg tgtacaaaaa gactctgttt gtagaattca cggatcacct
tttcaacatc 240 gctaagccaa ggccaccctg gatgggtctg ctaggtccta
ccatccaggc tgaggtttat 300 gatacagtgg tcattacact taagaacatg
gcttcccatc ctgtcagtct tcatgctgtt 360 ggtgtatcct actggaaagc
ttctgaggga gctgaatatg atgatcagac cagtcaaagg 420 gagaaagaag
atgataaagt cttccctggt ggaagccata catatgtctg gcaggtcctg 480
aaagagaatg gtccaatggc ctctgaccca ctgtgcctta cctactcata tctttctcat
540 gtggacctgg taaaagactt gaattcaggc ctcattggag ccctactagt
atgtagagaa 600 gggagtctgg ccaaggaaaa gacacagacc ttgcacaaat
ttatactact ttttgctgta 660 tttgatgaag ggaaaagttg gcactcagaa
acaaagaact ccttgatgca ggatagggat 720 gctgcatctg ctcgggcctg
gcctaaaatg cacacagtca atggttatgt aaacaggtct 780 ctgccaggtc
tgattggatg ccacaggaaa tcagtctatt ggcatgtgat tggaatgggc 840
accactcctg aagtgcactc aatattcctc gaaggtcaca catttcttgt gaggaaccat
900 cgccaggcgt ccttggaaat ctcgccaata actttcctta ctgctcaaac
actcttgatg 960 gaccttggac agtttctact gttttgtcat atctcttccc
accaacatga tggcatggaa 1020 gcttatgtca aagtagacag ctgtccagag
gaaccccaac tacgaatgaa aaataatgaa 1080 gaagcggaag actatgatga
tgatcttact gattctgaaa tggatgtggt caggtttgat 1140 gatgacaact
ctccttcctt tatccaaatt cgctcagttg ccaagaagca tcctaaaact 1200
tgggtacatt acattgctgc tgaagaggag gactgggact atgctccctt agtcctcgcc
1260 cccgatgaca gaagttataa aagtcaatat ttgaacaatg gccctcagcg
gattggtagg 1320 aagtacaaaa aagtccgatt tatggcatac acagatgaaa
cctttaagac tcgtgaagct 1380 attcagcatg aatcaggaat cttgggacct
ttactttatg gggaagttgg agacacactg 1440 ttgattatat ttaagaatca
agcaagcaga ccatataaca tctaccctca cggaatcact 1500 gatgtccgtc
ctttgtattc aaggagatta ccaaaaggtg taaaacattt gaaggatttt 1560
ccaattctgc caggagaaat attcaaatat aaatggacag tgactgtaga agatgggcca
1620 actaaatcag atcctcggtg cctgacccgc tattactcta gtttcgttaa
tatggagaga 1680 gatctagctt caggactcat tggccctctc ctcatctgct
acaaagaatc tgtagatcaa 1740 agaggaaacc agataatgtc agacaagagg
aatgtcatcc tgttttctgt atttgatgag 1800 aaccgaagct ggtacctcac
agagaatata caacgctttc tccccaatcc agctggagtg 1860 cagcttgagg
atccagagtt ccaagcctcc aacatcatgc acagcatcaa tggctatgtt 1920
tttgatagtt tgcagttgtc agtttgtttg catgaggtgg catactggta cattctaagc
1980 attggagcac agactgactt cctttctgtc ttcttctctg gatatacctt
caaacacaaa 2040 atggtctatg aagacacact caccctattc ccattctcag
gagaaactgt cttcatgtcg 2100 atggaaaacc caggtctatg gattctgggg
tgccacaact cagactttcg gaacagaggc 2160 atgaccgcct tactgaaggt
ttctagttgt gacaagaaca ctggtgatta ttacgaggac 2220 agttatgaag
atatttcagc atacttgctg agtaaaaaca atgccattga accaagaagc 2280
ttctcccaga attcaagaca ccctagcact aggcaaaagc aatttaatgc caccacaatt
2340 ccagaaaatg acatagagaa gactgaccct tggtttgcac acagaacacc
tatgcctaaa 2400 atacaaaatg tctcctctag tgatttgttg atgctcttgc
gacagagtcc tactccacat 2460 gggctatcct tatctgatct ccaagaagcc
aaatatgaga ctttttctga tgatccatca 2520 cctggagcaa tagacagtaa
taacagcctg tctgaaatga cacacttcag gccacagctc 2580 catcacagtg
gggacatggt atttacccct gagtcaggcc tccaattaag attaaatgag 2640
aaactgggga caactgcagc aacagagttg aagaaacttg atttcaaagt ttctagtaca
2700 tcaaataatc tgatttcaac aattccatca gacaatttgg cagcaggtac
tgataataca 2760 agttccttag gacccccaag tatgccagtt cattatgata
gtcaattaga taccactcta 2820 tttggcaaaa agtcatctcc ccttactgag
tctggtggac ctctgagctt gagtgaagaa 2880 aataatgatt caaagttgtt
agaatcaggt ttaatgaata gccaagaaag ttcatgggga 2940 aaaaatgtat
cgtcaacaga gagtggtagg ttatttaaag ggaaaagagc tcatggacct 3000
gctttgttga ctaaagataa tgccttattc aaagttagca tctctttgtt aaagacaaac
3060 aaaacttcca ataattcagc aactaataga aagactcaca ttgatggccc
atcattatta 3120 attgagaata gtccatcagt ctggcaaaat atattagaaa
gtgacactga gtttaaaaaa 3180 gtgacacctt tgattcatga cagaatgctt
atggacaaaa atgctacagc tttgaggcta 3240 aatcatatgt caaataaaac
tacttcatca aaaaacatgg aaatggtcca acagaaaaaa 3300 gagggcccca
ttccaccaga tgcacaaaat ccagatatgt cgttctttaa gatgctattc 3360
ttgccagaat cagcaaggtg gatacaaagg actcatggaa agaactctct gaactctggg
3420 caaggcccca gtccaaagca attagtatcc ttaggaccag aaaaatctgt
ggaaggtcag 3480 aatttcttgt ctgagaaaaa caaagtggta gtaggaaagg
gtgaatttac aaaggacgta 3540 ggactcaaag agatggtttt tccaagcagc
agaaacctat ttcttactaa cttggataat 3600 ttacatgaaa ataatacaca
caatcaagaa aaaaaaattc aggaagaaat agaaaagaag 3660 gaaacattaa
tccaagagaa tgtagttttg cctcagatac atacagtgac tggcactaag 3720
aatttcatga agaacctttt cttactgagc actaggcaaa atgtagaagg ttcatatgac
3780 ggggcatatg ctccagtact tcaagatttt aggtcattaa atgattcaac
aaatagaaca 3840 aagaaacaca cagctcattt ctcaaaaaaa ggggaggaag
aaaacttgga aggcttggga 3900 aatcaaacca agcaaattgt agagaaatat
gcatgcacca caaggatatc tcctaataca 3960 agccagcaga attttgtcac
gcaacgtagt aagagagctt tgaaacaatt cagactccca 4020 ctagaagaaa
cagaacttga aaaaaggata attgtggatg acacctcaac ccagtggtcc 4080
aaaaacatga aacatttgac cccgagcacc ctcacacaga tagactacaa tgagaaggag
4140 aaaggggcca ttactcagtc tcccttatca gattgcctta cgaggagtca
tagcatccct 4200 caagcaaata gatctccatt acccattgca aaggtatcat
catttccatc tattagacct 4260 atatatctga ccagggtcct attccaagac
aactcttctc atcttccagc agcatcttat 4320 agaaagaaag attctggggt
ccaagaaagc agtcatttct tacaaggagc caaaaaaaat 4380 aacctttctt
tagccattct aaccttggag atgactggtg atcaaagaga ggttggctcc 4440
ctggggacaa gtgccacaaa ttcagtcaca tacaagaaag ttgagaacac tgttctcccg
4500 aaaccagact tgcccaaaac atctggcaaa gttgaattgc ttccaaaagt
tcacatttat 4560 cagaaggacc tattccctac ggaaactagc aatgggtctc
ctggccatct ggatctcgtg 4620 gaagggagcc ttcttcaggg aacagaggga
gcgattaagt ggaatgaagc aaacagacct 4680 ggaaaagttc cctttctgag
agtagcaaca gaaagctctg caaagactcc ctccaagcta 4740 ttggatcctc
ttgcttggga taaccactat ggtactcaga taccaaaaga agagtggaaa 4800
tcccaagaga agtcaccaga aaaaacagct tttaagaaaa aggataccat tttgtccctg
4860 aacgcttgtg aaagcaatca tgcaatagca gcaataaatg agggacaaaa
taagcccgaa 4920 atagaagtca cctgggcaaa gcaaggtagg actgaaaggc
tgtgctctca aaacccacca 4980 gtcttgaaac gccatcaacg ggaaataact
cgtactactc ttcagtcaga tcaagaggaa 5040 attgactatg atgataccat
atcagttgaa atgaagaagg aagattttga catttatgat 5100 gaggatgaaa
atcagagccc ccgcagcttt caaaagaaaa cacgacacta ttttattgct 5160
gcagtggaga ggctctggga ttatgggatg agtagctccc cacatgttct aagaaacagg
5220 gctcagagtg gcagtgtccc tcagttcaag aaagttgttt tccaggaatt
tactgatggc 5280 tcctttactc agcccttata ccgtggagaa ctaaatgaac
atttgggact cctggggcca 5340 tatataagag cagaagttga agataatatc
atggtaactt tcagaaatca ggcctctcgt 5400 ccctattcct tctattctag
ccttatttct tatgaggaag atcagaggca aggagcagaa 5460 cctagaaaaa
actttgtcaa gcctaatgaa accaaaactt acttttggaa agtgcaacat 5520
catatggcac ccactaaaga tgagtttgac tgcaaagcct gggcttattt ctctgatgtt
5580 gacctggaaa aagatgtgca ctcaggcctg attggacccc ttctggtctg
ccacactaac 5640 acactgaacc ctgctcatgg gagacaagtg acagtacagg
aatttgctct gtttttcacc 5700 atctttgatg agaccaaaag ctggtacttc
actgaaaata tggaaagaaa ctgcagggct 5760 ccctgcaata tccagatgga
agatcccact tttaaagaga attatcgctt ccatgcaatc 5820 aatggctaca
taatggatac actacctggc ttagtaatgg ctcaggatca aaggattcga 5880
tggtatctgc tcagcatggg cagcaatgaa aacatccatt ctattcattt cagtggacat
5940 gtgttcactg tacgaaaaaa agaggagtat aaaatggcac tgtacaatct
ctatccaggt 6000 gtttttgaga cagtggaaat gttaccatcc aaagctggaa
tttggcgggt ggaatgcctt 6060 attggcgagc atctacatgc tgggatgagc
acactttttc tggtgtacag caataagtgt 6120 cagactcccc tgggaatggc
ttctggacac attagagatt ttcagattac agcttcagga 6180 caatatggac
agtgggcccc aaagctggcc agacttcatt attccggatc aatcaatgcc 6240
tggagcacca aggagccctt ttcttggatc aaggtggatc tgttggcacc aatgattatt
6300 cacggcatca agacccaggg tgcccgtcag aagttctcca gcctctacat
ctctcagttt 6360 atcatcatgt atagtcttga tgggaagaag tggcagactt
atcgaggaaa ttccactgga 6420 accttaatgg tcttctttgg caatgtggat
tcatctggga taaaacacaa tatttttaac 6480 cctccaatta ttgctcgata
catccgtttg cacccaactc attatagcat tcgcagcact 6540 cttcgcatgg
agttgatggg ctgtgattta aatagttgca gcatgccatt gggaatggag 6600
agtaaagcaa tatcagatgc acagattact gcttcatcct actttaccaa tatgtttgcc
6660 acctggtctc cttcaaaagc tcgacttcac ctccaaggga ggagtaatgc
ctggagacct 6720 caggtgaata atccaaaaga gtggctgcaa gtggacttcc
agaagacaat gaaagtcaca 6780 ggagtaacta ctcagggagt aaaatctctg
cttaccagca tgtatgtgaa ggagttcctc 6840 atctccagca gtcaagatgg
ccatcagtgg actctctttt ttcagaatgg caaagtaaag 6900 gtttttcagg
gaaatcaaga ctccttcaca cctgtggtga actctctaga cccaccgtta 6960
ctgactcgct accttcgaat tcacccccag agttgggtgc accagattgc cctgaggatg
7020 gaggttctgg gctgcgaggc acaggacctc tacgacaaaa ctcacacatg
cccaccgtgc 7080 ccagctccag aactcctggg cggaccgtca gtcttcctct
tccccccaaa acccaaggac 7140 accctcatga tctcccggac ccctgaggtc
acatgcgtgg tggtggacgt gagccacgaa 7200 gaccctgagg tcaagttcaa
ctggtacgtg gacggcgtgg aggtgcataa tgccaagaca 7260 aagccgcggg
aggagcagta caacagcacg taccgtgtgg tcagcgtcct caccgtcctg 7320
caccaggact ggctgaatgg caaggagtac aagtgcaagg tctccaacaa agccctccca
7380 gcccccatcg agaaaaccat ctccaaagcc aaagggcagc cccgagaacc
acaggtgtac 7440 accctgcccc catcccggga tgagctgacc aagaaccagg
tcagcctgac ctgcctggtc 7500 aaaggcttct atcccagcga catcgccgtg
gagtgggaga gcaatgggca gccggagaac 7560 aactacaaga ccacgcctcc
cgtgttggac tccgacggct ccttcttcct ctacagcaag 7620 ctcaccgtgg
acaagagcag gtggcagcag gggaacgtct tctcatgctc cgtgatgcat 7680
gaggctctgc acaaccacta cacgcagaag agcctctccc tgtctccggg taaa 7734
<210> SEQ ID NO 10 <211> LENGTH: 2578 <212> TYPE:
PRT <213> ORGANISM: Artificial Sequence <220> FEATURE:
<223> OTHER INFORMATION: Full Length FVIIIFc <220>
FEATURE: <221> NAME/KEY: SIGNAL <222> LOCATION:
(-19)..(-1) <220> FEATURE: <221> NAME/KEY: mat_peptide
<222> LOCATION: (1)..(2559) <400> SEQUENCE: 10 Met Gln
Ile Glu Leu Ser Thr Cys Phe Phe Leu Cys Leu Leu Arg Phe -15 -10 -5
Cys Phe Ser Ala Thr Arg Arg Tyr Tyr Leu Gly Ala Val Glu Leu Ser -1
1 5 10 Trp Asp Tyr Met Gln Ser Asp Leu Gly Glu Leu Pro Val Asp Ala
Arg 15 20 25 Phe Pro Pro Arg Val Pro Lys Ser Phe Pro Phe Asn Thr
Ser Val Val 30 35 40 45 Tyr Lys Lys Thr Leu Phe Val Glu Phe Thr Asp
His Leu Phe Asn Ile 50 55 60 Ala Lys Pro Arg Pro Pro Trp Met Gly
Leu Leu Gly Pro Thr Ile Gln 65 70 75 Ala Glu Val Tyr Asp Thr Val
Val Ile Thr Leu Lys Asn Met Ala Ser 80 85 90 His Pro Val Ser Leu
His Ala Val Gly Val Ser Tyr Trp Lys Ala Ser 95 100 105 Glu Gly Ala
Glu Tyr Asp Asp Gln Thr Ser Gln Arg Glu Lys Glu Asp 110 115 120 125
Asp Lys Val Phe Pro Gly Gly Ser His Thr Tyr Val Trp Gln Val Leu 130
135 140 Lys Glu Asn Gly Pro Met Ala Ser Asp Pro Leu Cys Leu Thr Tyr
Ser 145 150 155 Tyr Leu Ser His Val Asp Leu Val Lys Asp Leu Asn Ser
Gly Leu Ile 160 165 170 Gly Ala Leu Leu Val Cys Arg Glu Gly Ser Leu
Ala Lys Glu Lys Thr 175 180 185 Gln Thr Leu His Lys Phe Ile Leu Leu
Phe Ala Val Phe Asp Glu Gly 190 195 200 205 Lys Ser Trp His Ser Glu
Thr Lys Asn Ser Leu Met Gln Asp Arg Asp 210 215 220 Ala Ala Ser Ala
Arg Ala Trp Pro Lys Met His Thr Val Asn Gly Tyr 225 230 235 Val Asn
Arg Ser Leu Pro Gly Leu Ile Gly Cys His Arg Lys Ser Val 240 245 250
Tyr Trp His Val Ile Gly Met Gly Thr Thr Pro Glu Val His Ser Ile 255
260 265 Phe Leu Glu Gly His Thr Phe Leu Val Arg Asn His Arg Gln Ala
Ser 270 275 280 285 Leu Glu Ile Ser Pro Ile Thr Phe Leu Thr Ala Gln
Thr Leu Leu Met 290 295 300 Asp Leu Gly Gln Phe Leu Leu Phe Cys His
Ile Ser Ser His Gln His 305 310 315 Asp Gly Met Glu Ala Tyr Val Lys
Val Asp Ser Cys Pro Glu Glu Pro 320 325 330 Gln Leu Arg Met Lys Asn
Asn Glu Glu Ala Glu Asp Tyr Asp Asp Asp 335 340 345 Leu Thr Asp Ser
Glu Met Asp Val Val Arg Phe Asp Asp Asp Asn Ser 350 355 360 365 Pro
Ser Phe Ile Gln Ile Arg Ser Val Ala Lys Lys His Pro Lys Thr 370 375
380 Trp Val His Tyr Ile Ala Ala Glu Glu Glu Asp Trp Asp Tyr Ala Pro
385 390 395 Leu Val Leu Ala Pro Asp Asp Arg Ser Tyr Lys Ser Gln Tyr
Leu Asn 400 405 410 Asn Gly Pro Gln Arg Ile Gly Arg Lys Tyr Lys Lys
Val Arg Phe Met 415 420 425 Ala Tyr Thr Asp Glu Thr Phe Lys Thr Arg
Glu Ala Ile Gln His Glu 430 435 440 445 Ser Gly Ile Leu Gly Pro Leu
Leu Tyr Gly Glu Val Gly Asp Thr Leu 450 455 460 Leu Ile Ile Phe Lys
Asn Gln Ala Ser Arg Pro Tyr Asn Ile Tyr Pro 465 470 475 His Gly Ile
Thr Asp Val Arg Pro Leu Tyr Ser Arg Arg Leu Pro Lys 480 485 490 Gly
Val Lys His Leu Lys Asp Phe Pro Ile Leu Pro Gly Glu Ile Phe 495 500
505 Lys Tyr Lys Trp Thr Val Thr Val Glu Asp Gly Pro Thr Lys Ser Asp
510 515 520 525 Pro Arg Cys Leu Thr Arg Tyr Tyr Ser Ser Phe Val Asn
Met Glu Arg 530 535 540 Asp Leu Ala Ser Gly Leu Ile Gly Pro Leu Leu
Ile Cys Tyr Lys Glu 545 550 555 Ser Val Asp Gln Arg Gly Asn Gln Ile
Met Ser Asp Lys Arg Asn Val 560 565 570 Ile Leu Phe Ser Val Phe Asp
Glu Asn Arg Ser Trp Tyr Leu Thr Glu 575 580 585 Asn Ile Gln Arg Phe
Leu Pro Asn Pro Ala Gly Val Gln Leu Glu Asp 590 595 600 605 Pro Glu
Phe Gln Ala Ser Asn Ile Met His Ser Ile Asn Gly Tyr Val 610 615 620
Phe Asp Ser Leu Gln Leu Ser Val Cys Leu His Glu Val Ala Tyr Trp 625
630 635 Tyr Ile Leu Ser Ile Gly Ala Gln Thr Asp Phe Leu Ser Val Phe
Phe 640 645 650 Ser Gly Tyr Thr Phe Lys His Lys Met Val Tyr Glu Asp
Thr Leu Thr 655 660 665 Leu Phe Pro Phe Ser Gly Glu Thr Val Phe Met
Ser Met Glu Asn Pro 670 675 680 685 Gly Leu Trp Ile Leu Gly Cys His
Asn Ser Asp Phe Arg Asn Arg Gly 690 695 700 Met Thr Ala Leu Leu Lys
Val Ser Ser Cys Asp Lys Asn Thr Gly Asp 705 710 715 Tyr Tyr Glu Asp
Ser Tyr Glu Asp Ile Ser Ala Tyr Leu Leu Ser Lys 720 725 730 Asn Asn
Ala Ile Glu Pro Arg Ser Phe Ser Gln Asn Ser Arg His Pro 735 740 745
Ser Thr Arg Gln Lys Gln Phe Asn Ala Thr Thr Ile Pro Glu Asn Asp 750
755 760 765 Ile Glu Lys Thr Asp Pro Trp Phe Ala His Arg Thr Pro Met
Pro Lys 770 775 780 Ile Gln Asn Val Ser Ser Ser Asp Leu Leu Met Leu
Leu Arg Gln Ser 785 790 795 Pro Thr Pro His Gly Leu Ser Leu Ser Asp
Leu Gln Glu Ala Lys Tyr 800 805 810 Glu Thr Phe Ser Asp Asp Pro Ser
Pro Gly Ala Ile Asp Ser Asn Asn 815 820 825 Ser Leu Ser Glu Met Thr
His Phe Arg Pro Gln Leu His His Ser Gly 830 835 840 845 Asp Met Val
Phe Thr Pro Glu Ser Gly Leu Gln Leu Arg Leu Asn Glu 850 855 860 Lys
Leu Gly Thr Thr Ala Ala Thr Glu Leu Lys Lys Leu Asp Phe Lys 865 870
875 Val Ser Ser Thr Ser Asn Asn Leu Ile Ser Thr Ile Pro Ser Asp Asn
880 885 890 Leu Ala Ala Gly Thr Asp Asn Thr Ser Ser Leu Gly Pro Pro
Ser Met 895 900 905 Pro Val His Tyr Asp Ser Gln Leu Asp Thr Thr Leu
Phe Gly Lys Lys 910 915 920 925 Ser Ser Pro Leu Thr Glu Ser Gly Gly
Pro Leu Ser Leu Ser Glu Glu 930 935 940 Asn Asn Asp Ser Lys Leu Leu
Glu Ser Gly Leu Met Asn Ser Gln Glu 945 950 955 Ser Ser Trp Gly Lys
Asn Val Ser Ser Thr Glu Ser Gly Arg Leu Phe 960 965 970 Lys Gly Lys
Arg Ala His Gly Pro Ala Leu Leu Thr Lys Asp Asn Ala 975 980 985 Leu
Phe Lys Val Ser Ile Ser Leu Leu Lys Thr Asn Lys Thr Ser Asn 990 995
1000 1005 Asn Ser Ala Thr Asn Arg Lys Thr His Ile Asp Gly Pro Ser
Leu 1010 1015 1020 Leu Ile Glu Asn Ser Pro Ser Val Trp Gln Asn Ile
Leu Glu Ser 1025 1030 1035 Asp Thr Glu Phe Lys Lys Val Thr Pro Leu
Ile His Asp Arg Met 1040 1045 1050 Leu Met Asp Lys Asn Ala Thr Ala
Leu Arg Leu Asn His Met Ser 1055 1060 1065 Asn Lys Thr Thr Ser Ser
Lys Asn Met Glu Met Val Gln Gln Lys 1070 1075 1080 Lys Glu Gly Pro
Ile Pro Pro Asp Ala Gln Asn Pro Asp Met Ser 1085 1090 1095 Phe Phe
Lys Met Leu Phe Leu Pro Glu Ser Ala Arg Trp Ile Gln 1100 1105 1110
Arg Thr His Gly Lys Asn Ser Leu Asn Ser Gly Gln Gly Pro Ser 1115
1120 1125 Pro Lys Gln Leu Val Ser Leu Gly Pro Glu Lys Ser Val Glu
Gly 1130 1135 1140 Gln Asn Phe Leu Ser Glu Lys Asn Lys Val Val Val
Gly Lys Gly 1145 1150 1155 Glu Phe Thr Lys Asp Val Gly Leu Lys Glu
Met Val Phe Pro Ser 1160 1165 1170 Ser Arg Asn Leu Phe Leu Thr Asn
Leu Asp Asn Leu His Glu Asn 1175 1180 1185 Asn Thr His Asn Gln Glu
Lys Lys Ile Gln Glu Glu Ile Glu Lys 1190 1195 1200 Lys Glu Thr Leu
Ile Gln Glu Asn Val Val Leu Pro Gln Ile His 1205 1210 1215 Thr Val
Thr Gly Thr Lys Asn Phe Met Lys Asn Leu Phe Leu Leu 1220 1225 1230
Ser Thr Arg Gln Asn Val Glu Gly Ser Tyr Asp Gly Ala Tyr Ala 1235
1240 1245 Pro Val Leu Gln Asp Phe Arg Ser Leu Asn Asp Ser Thr Asn
Arg 1250 1255 1260 Thr Lys Lys His Thr Ala His Phe Ser Lys Lys Gly
Glu Glu Glu 1265 1270 1275 Asn Leu Glu Gly Leu Gly Asn Gln Thr Lys
Gln Ile Val Glu Lys 1280 1285 1290 Tyr Ala Cys Thr Thr Arg Ile Ser
Pro Asn Thr Ser Gln Gln Asn 1295 1300 1305 Phe Val Thr Gln Arg Ser
Lys Arg Ala Leu Lys Gln Phe Arg Leu 1310 1315 1320 Pro Leu Glu Glu
Thr Glu Leu Glu Lys Arg Ile Ile Val Asp Asp 1325 1330 1335 Thr Ser
Thr Gln Trp Ser Lys Asn Met Lys His Leu Thr Pro Ser 1340 1345 1350
Thr Leu Thr Gln Ile Asp Tyr Asn Glu Lys Glu Lys Gly Ala Ile 1355
1360 1365 Thr Gln Ser Pro Leu Ser Asp Cys Leu Thr Arg Ser His Ser
Ile 1370 1375 1380 Pro Gln Ala Asn Arg Ser Pro Leu Pro Ile Ala Lys
Val Ser Ser 1385 1390 1395 Phe Pro Ser Ile Arg Pro Ile Tyr Leu Thr
Arg Val Leu Phe Gln 1400 1405 1410 Asp Asn Ser Ser His Leu Pro Ala
Ala Ser Tyr Arg Lys Lys Asp 1415 1420 1425 Ser Gly Val Gln Glu Ser
Ser His Phe Leu Gln Gly Ala Lys Lys 1430 1435 1440 Asn Asn Leu Ser
Leu Ala Ile Leu Thr Leu Glu Met Thr Gly Asp 1445 1450 1455 Gln Arg
Glu Val Gly Ser Leu Gly Thr Ser Ala Thr Asn Ser Val 1460 1465 1470
Thr Tyr Lys Lys Val Glu Asn Thr Val Leu Pro Lys Pro Asp Leu 1475
1480 1485 Pro Lys Thr Ser Gly Lys Val Glu Leu Leu Pro Lys Val His
Ile 1490 1495 1500 Tyr Gln Lys Asp Leu Phe Pro Thr Glu Thr Ser Asn
Gly Ser Pro 1505 1510 1515 Gly His Leu Asp Leu Val Glu Gly Ser Leu
Leu Gln Gly Thr Glu 1520 1525 1530 Gly Ala Ile Lys Trp Asn Glu Ala
Asn Arg Pro Gly Lys Val Pro 1535 1540 1545 Phe Leu Arg Val Ala Thr
Glu Ser Ser Ala Lys Thr Pro Ser Lys 1550 1555 1560 Leu Leu Asp Pro
Leu Ala Trp Asp Asn His Tyr Gly Thr Gln Ile 1565 1570 1575 Pro Lys
Glu Glu Trp Lys Ser Gln Glu Lys Ser Pro Glu Lys Thr 1580 1585 1590
Ala Phe Lys Lys Lys Asp Thr Ile Leu Ser Leu Asn Ala Cys Glu 1595
1600 1605 Ser Asn His Ala Ile Ala Ala Ile Asn Glu Gly Gln Asn Lys
Pro 1610 1615 1620 Glu Ile Glu Val Thr Trp Ala Lys Gln Gly Arg Thr
Glu Arg Leu 1625 1630 1635 Cys Ser Gln Asn Pro Pro Val Leu Lys Arg
His Gln Arg Glu Ile 1640 1645 1650 Thr Arg Thr Thr Leu Gln Ser Asp
Gln Glu Glu Ile Asp Tyr Asp 1655 1660 1665 Asp Thr Ile Ser Val Glu
Met Lys Lys Glu Asp Phe Asp Ile Tyr 1670 1675 1680 Asp Glu Asp Glu
Asn Gln Ser Pro Arg Ser Phe Gln Lys Lys Thr 1685 1690 1695 Arg His
Tyr Phe Ile Ala Ala Val Glu Arg Leu Trp Asp Tyr Gly 1700 1705 1710
Met Ser Ser Ser Pro His Val Leu Arg Asn Arg Ala Gln Ser Gly 1715
1720 1725 Ser Val Pro Gln Phe Lys Lys Val Val Phe Gln Glu Phe Thr
Asp 1730 1735 1740 Gly Ser Phe Thr Gln Pro Leu Tyr Arg Gly Glu Leu
Asn Glu His 1745 1750 1755 Leu Gly Leu Leu Gly Pro Tyr Ile Arg Ala
Glu Val Glu Asp Asn 1760 1765 1770 Ile Met Val Thr Phe Arg Asn Gln
Ala Ser Arg Pro Tyr Ser Phe 1775 1780 1785 Tyr Ser Ser Leu Ile Ser
Tyr Glu Glu Asp Gln Arg Gln Gly Ala 1790 1795 1800 Glu Pro Arg Lys
Asn Phe Val Lys Pro Asn Glu Thr Lys Thr Tyr 1805 1810 1815 Phe Trp
Lys Val Gln His His Met Ala Pro Thr Lys Asp Glu Phe 1820 1825 1830
Asp Cys Lys Ala Trp Ala Tyr Phe Ser Asp Val Asp Leu Glu Lys 1835
1840 1845 Asp Val His Ser Gly Leu Ile Gly Pro Leu Leu Val Cys His
Thr 1850 1855 1860 Asn Thr Leu Asn Pro Ala His Gly Arg Gln Val Thr
Val Gln Glu 1865 1870 1875 Phe Ala Leu Phe Phe Thr Ile Phe Asp Glu
Thr Lys Ser Trp Tyr 1880 1885 1890 Phe Thr Glu Asn Met Glu Arg Asn
Cys Arg Ala Pro Cys Asn Ile 1895 1900 1905 Gln Met Glu Asp Pro Thr
Phe Lys Glu Asn Tyr Arg Phe His Ala 1910 1915 1920 Ile Asn Gly Tyr
Ile Met Asp Thr Leu Pro Gly Leu Val Met Ala 1925 1930 1935 Gln Asp
Gln Arg Ile Arg Trp Tyr Leu Leu Ser Met Gly Ser Asn 1940 1945 1950
Glu Asn Ile His Ser Ile His Phe Ser Gly His Val Phe Thr Val 1955
1960 1965 Arg Lys Lys Glu Glu Tyr Lys Met Ala Leu Tyr Asn Leu Tyr
Pro 1970 1975 1980 Gly Val Phe Glu Thr Val Glu Met Leu Pro Ser Lys
Ala Gly Ile 1985 1990 1995 Trp Arg Val Glu Cys Leu Ile Gly Glu His
Leu His Ala Gly Met 2000 2005 2010 Ser Thr Leu Phe Leu Val Tyr Ser
Asn Lys Cys Gln Thr Pro Leu 2015 2020 2025 Gly Met Ala Ser Gly His
Ile Arg Asp Phe Gln Ile Thr Ala Ser 2030 2035 2040 Gly Gln Tyr Gly
Gln Trp Ala Pro Lys Leu Ala Arg Leu His Tyr 2045 2050 2055 Ser Gly
Ser Ile Asn Ala Trp Ser Thr Lys Glu Pro Phe Ser Trp 2060 2065 2070
Ile Lys Val Asp Leu Leu Ala Pro Met Ile Ile His Gly Ile Lys 2075
2080 2085 Thr Gln Gly Ala Arg Gln Lys Phe Ser Ser Leu Tyr Ile Ser
Gln 2090 2095 2100 Phe Ile Ile Met Tyr Ser Leu Asp Gly Lys Lys Trp
Gln Thr Tyr 2105 2110 2115 Arg Gly Asn Ser Thr Gly Thr Leu Met Val
Phe Phe Gly Asn Val 2120 2125 2130 Asp Ser Ser Gly Ile Lys His Asn
Ile Phe Asn Pro Pro Ile Ile 2135 2140 2145 Ala Arg Tyr Ile Arg Leu
His Pro Thr His Tyr Ser Ile Arg Ser 2150 2155 2160 Thr Leu Arg Met
Glu Leu Met Gly Cys Asp Leu Asn Ser Cys Ser 2165 2170 2175 Met Pro
Leu Gly Met Glu Ser Lys Ala Ile Ser Asp Ala Gln Ile 2180 2185 2190
Thr Ala Ser Ser Tyr Phe Thr Asn Met Phe Ala Thr Trp Ser Pro 2195
2200 2205 Ser Lys Ala Arg Leu His Leu Gln Gly Arg Ser Asn Ala Trp
Arg 2210 2215 2220 Pro Gln Val Asn Asn Pro Lys Glu Trp Leu Gln Val
Asp Phe Gln 2225 2230 2235 Lys Thr Met Lys Val Thr Gly Val Thr Thr
Gln Gly Val Lys Ser 2240 2245 2250 Leu Leu Thr Ser Met Tyr Val Lys
Glu Phe Leu Ile Ser Ser Ser 2255 2260 2265 Gln Asp Gly His Gln Trp
Thr Leu Phe Phe Gln Asn Gly Lys Val 2270 2275 2280 Lys Val Phe Gln
Gly Asn Gln Asp Ser Phe Thr Pro Val Val Asn 2285 2290 2295 Ser Leu
Asp Pro Pro Leu Leu Thr Arg Tyr Leu Arg Ile His Pro 2300 2305 2310
Gln Ser Trp Val His Gln Ile Ala Leu Arg Met Glu Val Leu Gly 2315
2320 2325 Cys Glu Ala Gln Asp Leu Tyr Asp Lys Thr His Thr Cys Pro
Pro 2330 2335 2340 Cys Pro Ala Pro Glu Leu Leu Gly Gly Pro Ser Val
Phe Leu Phe 2345 2350 2355 Pro Pro Lys Pro Lys Asp Thr Leu Met Ile
Ser Arg Thr Pro Glu 2360 2365 2370 Val Thr Cys Val Val Val Asp Val
Ser His Glu Asp Pro Glu Val 2375 2380 2385 Lys Phe Asn Trp Tyr Val
Asp Gly Val Glu Val His Asn Ala Lys 2390 2395 2400 Thr Lys Pro Arg
Glu Glu Gln Tyr Asn Ser Thr Tyr Arg Val Val 2405 2410 2415 Ser Val
Leu Thr Val Leu His Gln Asp Trp Leu Asn Gly Lys Glu 2420 2425 2430
Tyr Lys Cys Lys Val Ser Asn Lys Ala Leu Pro Ala Pro Ile Glu 2435
2440 2445 Lys Thr Ile Ser Lys Ala Lys Gly Gln Pro Arg Glu Pro Gln
Val 2450 2455 2460 Tyr Thr Leu Pro Pro Ser Arg Asp Glu Leu Thr Lys
Asn Gln Val 2465 2470 2475 Ser Leu Thr Cys Leu Val Lys Gly Phe Tyr
Pro Ser Asp Ile Ala 2480 2485 2490 Val Glu Trp Glu Ser Asn Gly Gln
Pro Glu Asn Asn Tyr Lys Thr 2495 2500 2505 Thr Pro Pro Val Leu Asp
Ser Asp Gly Ser Phe Phe Leu Tyr Ser 2510 2515 2520 Lys Leu Thr Val
Asp Lys Ser Arg Trp Gln Gln Gly Asn Val Phe 2525 2530 2535 Ser Cys
Ser Val Met His Glu Ala Leu His Asn His Tyr Thr Gln 2540 2545 2550
Lys Ser Leu Ser Leu Ser Pro Gly Lys 2555 <210> SEQ ID NO 11
<211> LENGTH: 21 <212> TYPE: PRT <213> ORGANISM:
Artificial Sequence <220> FEATURE: <223> OTHER
INFORMATION: Partial B domain <400> SEQUENCE: 11 Ser Phe Ser
Gln Asn Ser Arg His Pro Ser Gln Asn Pro Pro Val Leu 1 5 10 15 Lys
Arg His Gln Arg 20 <210> SEQ ID NO 12 <211> LENGTH: 11
<212> TYPE: PRT <213> ORGANISM: Artificial Sequence
<220> FEATURE: <223> OTHER INFORMATION: albumin-binding
peptide <400> SEQUENCE: 12 Asp Ile Cys Leu Pro Arg Trp Gly
Cys Leu Trp 1 5 10 <210> SEQ ID NO 13 <211> LENGTH: 32
<212> TYPE: PRT <213> ORGANISM: Artificial Sequence
<220> FEATURE: <223> OTHER INFORMATION: CTP peptide
<400> SEQUENCE: 13 Asp Pro Arg Phe Gln Asp Ser Ser Ser Ser
Lys Ala Pro Pro Pro Ser 1 5 10 15 Leu Pro Ser Pro Ser Arg Leu Pro
Gly Pro Ser Asp Thr Pro Ile Leu 20 25 30 <210> SEQ ID NO 14
<211> LENGTH: 28 <212> TYPE: PRT <213> ORGANISM:
Artificial Sequence <220> FEATURE: <223> OTHER
INFORMATION: CTP peptide <400> SEQUENCE: 14 Ser Ser Ser Ser
Lys Ala Pro Pro Pro Ser Leu Pro Ser Pro Ser Arg 1 5 10 15 Leu Pro
Gly Pro Ser Asp Thr Pro Ile Leu Pro Gln 20 25 <210> SEQ ID NO
15 <211> LENGTH: 20 <212> TYPE: PRT <213>
ORGANISM: Artificial Sequence <220> FEATURE: <223>
OTHER INFORMATION: PAS peptide <400> SEQUENCE: 15 Ala Ser Pro
Ala Ala Pro Ala Pro Ala Ser Pro Ala Ala Pro Ala Pro 1 5 10 15 Ser
Ala Pro Ala 20 <210> SEQ ID NO 16 <211> LENGTH: 20
<212> TYPE: PRT <213> ORGANISM: Artificial Sequence
<220> FEATURE: <223> OTHER INFORMATION: PAS peptide
<400> SEQUENCE: 16 Ala Ala Pro Ala Ser Pro Ala Pro Ala Ala
Pro Ser Ala Pro Ala Pro 1 5 10 15 Ala Ala Pro Ser 20 <210>
SEQ ID NO 17 <211> LENGTH: 20 <212> TYPE: PRT
<213> ORGANISM: Artificial Sequence <220> FEATURE:
<223> OTHER INFORMATION: PAS peptide <400> SEQUENCE: 17
Ala Pro Ser Ser Pro Ser Pro Ser Ala Pro Ser Ser Pro Ser Pro Ala 1 5
10 15 Ser Pro Ser Ser 20 <210> SEQ ID NO 18 <211>
LENGTH: 19 <212> TYPE: PRT <213> ORGANISM: Artificial
Sequence <220> FEATURE: <223> OTHER INFORMATION: PAS
peptide <400> SEQUENCE: 18 Ala Pro Ser Ser Pro Ser Pro Ser
Ala Pro Ser Ser Pro Ser Pro Ala 1 5 10 15 Ser Pro Ser <210>
SEQ ID NO 19 <211> LENGTH: 20 <212> TYPE: PRT
<213> ORGANISM: Artificial Sequence <220> FEATURE:
<223> OTHER INFORMATION: PAS peptide <400> SEQUENCE: 19
Ser Ser Pro Ser Ala Pro Ser Pro Ser Ser Pro Ala Ser Pro Ser Pro 1 5
10 15 Ser Ser Pro Ala 20 <210> SEQ ID NO 20 <211>
LENGTH: 24 <212> TYPE: PRT <213> ORGANISM: Artificial
Sequence <220> FEATURE: <223> OTHER INFORMATION: PAS
peptide <400> SEQUENCE: 20 Ala Ala Ser Pro Ala Ala Pro Ser
Ala Pro Pro Ala Ala Ala Ser Pro 1 5 10 15 Ala Ala Pro Ser Ala Pro
Pro Ala 20 <210> SEQ ID NO 21 <211> LENGTH: 20
<212> TYPE: PRT <213> ORGANISM: Artificial Sequence
<220> FEATURE: <223> OTHER INFORMATION: PAS peptide
<400> SEQUENCE: 21 Ala Ser Ala Ala Ala Pro Ala Ala Ala Ser
Ala Ala Ala Ser Ala Pro 1 5 10 15 Ser Ala Ala Ala 20
1 SEQUENCE LISTING <160> NUMBER OF SEQ ID NOS: 21 <210>
SEQ ID NO 1 <211> LENGTH: 7583 <212> TYPE: DNA
<213> ORGANISM: Artificial Sequence <220> FEATURE:
<223> OTHER INFORMATION: pSYN-FIX-030 <400> SEQUENCE: 1
gcgcgcgttg acattgatta ttgactagtt attaatagta atcaattacg gggtcattag
60 ttcatagccc atatatggag ttccgcgtta cataacttac ggtaaatggc
ccgcctggct 120 gaccgcccaa cgacccccgc ccattgacgt caataatgac
gtatgttccc atagtaacgc 180 caatagggac tttccattga cgtcaatggg
tggagtattt acggtaaact gcccacttgg 240 cagtacatca agtgtatcat
atgccaagta cgccccctat tgacgtcaat gacggtaaat 300 ggcccgcctg
gcattatgcc cagtacatga ccttatggga ctttcctact tggcagtaca 360
tctacgtatt agtcatcgct attaccatgg tgatgcggtt ttggcagtac atcaatgggc
420 gtggatagcg gtttgactca cggggatttc caagtctcca ccccattgac
gtcaatggga 480 gtttgttttg gcaccaaaat caacgggact ttccaaaatg
tcgtaacaac tccgccccat 540 tgacgcaaat gggcggtagg cgtgtacggt
gggaggtcta tataagcaga gctctctggc 600 taactagaga acccactgct
tactggctta tcgaaattaa tacgactcac tatagggaga 660 cccaagcttc
gcgacgtacg gccgccacca tgcagcgcgt gaacatgatc atggcagaat 720
caccaggcct catcaccatc tgccttttag gatatctact cagtgctgaa tgtacaggtt
780 tgtttccttt tttaaaatac attgagtatg cttgcctttt agatatagaa
atatctgatg 840 ctgtcttctt cactaaattt tgattacatg atttgacagc
aatattgaag agtctaacag 900 ccagcacgca ggttggtaag tactgtggga
acatcacaga ttttggctcc atgccctaaa 960 gagaaattgg ctttcagatt
atttggatta aaaacaaaga ctttcttaag agatgtaaaa 1020 ttttcatgat
gttttctttt ttgctaaaac taaagaatta ttcttttaca tttcagtttt 1080
tcttgatcat gaaaacgcca acaaaattct gaatcggcca aagaggtata attcaggtaa
1140 attggaagag tttgttcaag ggaatctaga gagagaatgt atggaagaaa
agtgtagttt 1200 tgaagaagca cgagaagttt ttgaaaacac tgaaagaaca
actgaatttt ggaagcagta 1260 tgttgatgga gatcagtgtg agtccaatcc
atgtttaaat ggcggcagtt gcaaggatga 1320 cattaattcc tatgaatgtt
ggtgtccctt tggatttgaa ggaaagaact gtgaattaga 1380 tgtaacatgt
aacattaaga atggcagatg cgagcagttt tgtaaaaata gtgctgataa 1440
caaggtggtt tgctcctgta ctgagggata tcgacttgca gaaaaccaga agtcctgtga
1500 accagcagtg ccatttccat gtggaagagt ttctgtttca caaacttcta
agctcacccg 1560 tgctgagact gtttttcctg atgtggacta tgtaaattct
actgaagctg aaaccatttt 1620 ggataacatc actcaaagca cccaatcatt
taatgacttc actcgggttg ttggtggaga 1680 agatgccaaa ccaggtcaat
tcccttggca ggttgttttg aatggtaaag ttgatgcatt 1740 ctgtggaggc
tctatcgtta atgaaaaatg gattgtaact gctgcccact gtgttgaaac 1800
tggtgttaaa attacagttg tcgcaggtga acataatatt gaggagacag aacatacaga
1860 gcaaaagcga aatgtgattc gaattattcc tcaccacaac tacaatgcag
ctattaataa 1920 gtacaaccat gacattgccc ttctggaact ggacgaaccc
ttagtgctaa acagctacgt 1980 tacacctatt tgcattgctg acaaggaata
cacgaacatc ttcctcaaat ttggatctgg 2040 ctatgtaagt ggctggggaa
gagtcttcca caaagggaga tcagctttag ttcttcagta 2100 ccttagagtt
ccacttgttg accgagccac atgtcttcga tctacaaagt tcaccatcta 2160
taacaacatg ttctgtgctg gcttccatga aggaggtaga gattcatgtc aaggagatag
2220 tgggggaccc catgttactg aagtggaagg gaccagtttc ttaactggaa
ttattagctg 2280 gggtgaagag tgtgcaatga aaggcaaata tggaatatat
accaaggtgt cccggtatgt 2340 caactggatt aaggaaaaaa caaagctcac
tgacaaaact cacacatgcc caccgtgccc 2400 agctccggaa ctcctgggcg
gaccgtcagt cttcctcttc cccccaaaac ccaaggacac 2460 cctcatgatc
tcccggaccc ctgaggtcac atgcgtggtg gtggacgtga gccacgaaga 2520
ccctgaggtc aagttcaact ggtacgtgga cggcgtggag gtgcataatg ccaagacaaa
2580 gccgcgggag gagcagtaca acagcacgta ccgtgtggtc agcgtcctca
ccgtcctgca 2640 ccaggactgg ctgaatggca aggagtacaa gtgcaaggtc
tccaacaaag ccctcccagc 2700 ccccatcgag aaaaccatct ccaaagccaa
agggcagccc cgagaaccac aggtgtacac 2760 cctgccccca tcccgggatg
agctgaccaa gaaccaggtc agcctgacct gcctggtcaa 2820 aggcttctat
cccagcgaca tcgccgtgga gtgggagagc aatgggcagc cggagaacaa 2880
ctacaagacc acgcctcccg tgttggactc cgacggctcc ttcttcctct acagcaagct
2940 caccgtggac aagagcaggt ggcagcaggg gaacgtcttc tcatgctccg
tgatgcatga 3000 ggctctgcac aaccactaca cgcagaagag cctctccctg
tctccgggta aatgagaatt 3060 cagacatgat aagatacatt gatgagtttg
gacaaaccac aactagaatg cagtgaaaaa 3120 aatgctttat ttgtgaaatt
tgtgatgcta ttgctttatt tgtaaccatt ataagctgca 3180 ataaacaagt
tggggtgggc gaagaactcc agcatgagat ccccgcgctg gaggatcatc 3240
cagccggcgt cccggaaaac gattccgaag cccaaccttt catagaaggc ggcggtggaa
3300 tcgaaatctc gtagcacgtg tcagtcctgc tcctcggcca cgaagtgcac
gcagttgccg 3360 gccgggtcgc gcagggcgaa ctcccgcccc cacggctgct
cgccgatctc ggtcatggcc 3420 ggcccggagg cgtcccggaa gttcgtggac
acgacctccg accactcggc gtacagctcg 3480 tccaggccgc gcacccacac
ccaggccagg gtgttgtccg gcaccacctg gtcctggacc 3540 gcgctgatga
acagggtcac gtcgtcccgg accacaccgg cgaagtcgtc ctccacgaag 3600
tcccgggaga acccgagccg gtcggtccag aactcgaccg ctccggcgac gtcgcgcgcg
3660 gtgagcaccg gaacggcact ggtcaacttg gccatggttt agttcctcac
cttgtcgtat 3720 tatactatgc cgatatacta tgccgatgat taattgtcaa
cacgtgctga tcagatccga 3780 aaatggatat acaagctccc gggagctttt
tgcaaaagcc taggcctcca aaaaagcctc 3840 ctcactactt ctggaatagc
tcagaggcag aggcggcctc ggcctctgca taaataaaaa 3900 aaattagtca
gccatggggc ggagaatggg cggaactggg cggagttagg ggcgggatgg 3960
gcggagttag gggcgggact atggttgctg actaattgag atgcatgctt tgcatacttc
4020 tgcctgctgg ggagcctggg gactttccac acctggttgc tgactaattg
agatgcatgc 4080 tttgcatact tctgcctgct ggggagcctg gggactttcc
acaccctcgt cgagctagct 4140 tcgtgaggct ccggtgcccg tcagtgggca
gagcgcacat cgcccacagt ccccgagaag 4200 ttggggggag gggtcggcaa
ttgaaccggt gcctagagaa ggtggcgcgg ggtaaactgg 4260 gaaagtgatg
tcgtgtactg gctccgcctt tttcccgagg gtgggggaga accgtatata 4320
agtgcagtag tcgccgtgaa cgttcttttt cgcaacgggt ttgccgccag aacacaggta
4380 agtgccgtgt gtggttcccg cgggcctggc ctctttacgg gttatggccc
ttgcgtgcct 4440 tgaattactt ccacctggct ccagtacgtg attcttgatc
ccgagctgga gccaggggcg 4500 ggccttgcgc tttaggagcc ccttcgcctc
gtgcttgagt tgaggcctgg cctgggcgct 4560 ggggccgccg cgtgcgaatc
tggtggcacc ttcgcgcctg tctcgctgct ttcgataagt 4620 ctctagccat
ttaaaatttt tgatgacctg ctgcgacgct ttttttctgg caagatagtc 4680
ttgtaaatgc gggccaggat ctgcacactg gtatttcggt ttttggggcc gcgggcggcg
4740 acggggcccg tgcgtcccag cgcacatgtt cggcgaggcg gggcctgcga
gcgcggccac 4800 cgagaatcgg acgggggtag tctcaagctg gccggcctgc
tctggtgcct ggcctcgcgc 4860 cgccgtgtat cgccccgccc tgggcggcaa
ggctggcccg gtcggcacca gttgcgtgag 4920 cggaaagatg gccgcttccc
ggccctgctc cagggggctc aaaatggagg acgcggcgct 4980 cgggagagcg
ggcgggtgag tcacccacac aaaggaaagg ggcctttccg tcctcagccg 5040
tcgcttcatg tgactccacg gagtaccggg cgccgtccag gcacctcgat tagttctgga
5100 gcttttggag tacgtcgtct ttaggttggg gggaggggtt ttatgcgatg
gagtttcccc 5160 acactgagtg ggtggagact gaagttaggc cagcttggca
cttgatgtaa ttctccttgg 5220 aatttgccct ttttgagttt ggatcttggt
tcattctcaa gcctcagaca gtggttcaaa 5280 gtttttttct tccatttcag
gtgtcgtgaa cacgtggtcg cggccgcgcc gccaccatgg 5340 agacagacac
actcctgcta tgggtactgc tgctctgggt tccaggttcc actggtgaca 5400
aaactcacac atgcccaccg tgcccagcac ctgaactcct gggaggaccg tcagtcttcc
5460 tcttcccccc aaaacccaag gacaccctca tgatctcccg gacccctgag
gtcacatgcg 5520 tggtggtgga cgtgagccac gaagaccctg aggtcaagtt
caactggtac gtggacggcg 5580 tggaggtgca taatgccaag acaaagccgc
gggaggagca gtacaacagc acgtaccgtg 5640 tggtcagcgt cctcaccgtc
ctgcaccagg actggctgaa tggcaaggag tacaagtgca 5700 aggtctccaa
caaagccctc ccagccccca tcgagaaaac catctccaaa gccaaagggc 5760
agccccgaga accacaggtg tacaccctgc ccccatcccg cgatgagctg accaagaacc
5820 aggtcagcct gacctgcctg gtcaaaggct tctatcccag cgacatcgcc
gtggagtggg 5880 agagcaatgg gcagccggag aacaactaca agaccacgcc
tcccgtgttg gactccgacg 5940 gctccttctt cctctacagc aagctcaccg
tggacaagag caggtggcag caggggaacg 6000 tcttctcatg ctccgtgatg
catgaggctc tgcacaacca ctacacgcag aagagcctct 6060 ccctgtctcc
gggtaaatga ctcgagagat ctggccggct gggcccgttt cgaaggtaag 6120
cctatcccta accctctcct cggtctcgat tctacgcgta ccggtcatca tcaccatcac
6180 cattgagttt aaacccgctg atcagcctcg actgtgcctt ctagttgcca
gccatctgtt 6240 gtttgcccct cccccgtgcc ttccttgacc ctggaaggtg
ccactcccac tgtcctttcc 6300 taataaaatg aggaaattgc atcgcattgt
ctgagtaggt gtcattctat tctggggggt 6360 ggggtggggc aggacagcaa
gggggaggat tgggaagaca atagcaggca tgctggggat 6420 gcggtgggct
ctatggcttc tgaggcggaa agaaccagtg gcggtaatac ggttatccac 6480
agaatcaggg gataacgcag gaaagaacat gtgagcaaaa ggccagcaaa aggccaggaa
6540 ccgtaaaaag gccgcgttgc tggcgttttt ccataggctc cgcccccctg
acgagcatca 6600 caaaaatcga cgctcaagtc agaggtggcg aaacccgaca
ggactataaa gataccaggc 6660 gtttccccct agaagctccc tcgtgcgctc
tcctgttccg accctgccgc ttaccggata 6720 cctgtccgcc tttctccctt
cgggaagcgt ggcgctttct catagctcac gctgtaggta 6780 tctcagttcg
gtgtaggtcg ttcgctccaa gctgggctgt gtgcacgaac cccccgttca 6840
gcccgaccgc tgcgccttat ccggtaacta tcgtcttgag tccaacccgg taagacacga
6900 cttatcgcca ctggcagcag ccactggtaa caggattagc agagcgaggt
atgtaggcgg 6960 tgctacagag ttcttgaagt ggtggcctaa ctacggctac
actagaagaa cagtatttgg 7020 tatctgcgct ctgctgaagc cagttacctt
cggaaaaaga gttggtagct cttgatccgg 7080
caaacaaacc accgctggta gcggtggttt ttttgtttgc aagcagcaga ttacgcgcag
7140 aaaaaaagga tctcaagaag atcctttgat cttttctacg gggtctgacg
ctcagtggaa 7200 cgaaaactca cgttaaggga ttttggtcat gacattaacc
tataaaaata ggcgtatcac 7260 gaggcccttt cgtctcgcgc gtttcggtga
tgacggtgaa aacctctgac acatgcagct 7320 cccggagacg gtcacagctt
gtctgtaagc ggatgccggg agcagacaag cccgtcaggg 7380 cgcgtcagcg
ggtgttggcg ggtgtcgggg ctggcttaac tatgcggcat cagagcagat 7440
tgtactgaga gtgcaccata tatgcggtgt gaaataccgc acagatgcgt aaggagaaaa
7500 taccgcatca ggcgccattc gccattcagg ctgcgcaact gttgggaagg
gcgatcggtg 7560 cgggcctctt cgctattacg cca 7583 <210> SEQ ID
NO 2 <211> LENGTH: 688 <212> TYPE: PRT <213>
ORGANISM: Artificial Sequence <220> FEATURE: <223>
OTHER INFORMATION: pSYN-FIX-030 <220> FEATURE: <221>
NAME/KEY: SIGNAL <222> LOCATION: (-46)..(-19) 220>
<221> NAME/KEY: SIGNAL <222> LOCATION: (-18)..(-1)
<220> FEATURE: <221> NAME/KEY: mat_peptide <222>
LOCATION: (1)..(642) <400> SEQUENCE: 2 Met Gln Arg Val Asn
Met Ile Met Ala Glu Ser Pro Gly Leu Ile Thr -45 -40 -35 Ile Cys Leu
Leu Gly Tyr Leu Leu Ser Ala Glu Cys Thr Val Phe Leu -30 -25 -20 -15
Asp His Glu Asn Ala Asn Lys Ile Leu Asn Arg Pro Lys Arg Tyr Asn -10
-5 -1 1 Ser Gly Lys Leu Glu Glu Phe Val Gln Gly Asn Leu Glu Arg Glu
Cys 5 10 15 Met Glu Glu Lys Cys Ser Phe Glu Glu Ala Arg Glu Val Phe
Glu Asn 20 25 30 Thr Glu Arg Thr Thr Glu Phe Trp Lys Gln Tyr Val
Asp Gly Asp Gln 35 40 45 50 Cys Glu Ser Asn Pro Cys Leu Asn Gly Gly
Ser Cys Lys Asp Asp Ile 55 60 65 Asn Ser Tyr Glu Cys Trp Cys Pro
Phe Gly Phe Glu Gly Lys Asn Cys 70 75 80 Glu Leu Asp Val Thr Cys
Asn Ile Lys Asn Gly Arg Cys Glu Gln Phe 85 90 95 Cys Lys Asn Ser
Ala Asp Asn Lys Val Val Cys Ser Cys Thr Glu Gly 100 105 110 Tyr Arg
Leu Ala Glu Asn Gln Lys Ser Cys Glu Pro Ala Val Pro Phe 115 120 125
130 Pro Cys Gly Arg Val Ser Val Ser Gln Thr Ser Lys Leu Thr Arg Ala
135 140 145 Glu Thr Val Phe Pro Asp Val Asp Tyr Val Asn Ser Thr Glu
Ala Glu 150 155 160 Thr Ile Leu Asp Asn Ile Thr Gln Ser Thr Gln Ser
Phe Asn Asp Phe 165 170 175 Thr Arg Val Val Gly Gly Glu Asp Ala Lys
Pro Gly Gln Phe Pro Trp 180 185 190 Gln Val Val Leu Asn Gly Lys Val
Asp Ala Phe Cys Gly Gly Ser Ile 195 200 205 210 Val Asn Glu Lys Trp
Ile Val Thr Ala Ala His Cys Val Glu Thr Gly 215 220 225 Val Lys Ile
Thr Val Val Ala Gly Glu His Asn Ile Glu Glu Thr Glu 230 235 240 His
Thr Glu Gln Lys Arg Asn Val Ile Arg Ile Ile Pro His His Asn 245 250
255 Tyr Asn Ala Ala Ile Asn Lys Tyr Asn His Asp Ile Ala Leu Leu Glu
260 265 270 Leu Asp Glu Pro Leu Val Leu Asn Ser Tyr Val Thr Pro Ile
Cys Ile 275 280 285 290 Ala Asp Lys Glu Tyr Thr Asn Ile Phe Leu Lys
Phe Gly Ser Gly Tyr 295 300 305 Val Ser Gly Trp Gly Arg Val Phe His
Lys Gly Arg Ser Ala Leu Val 310 315 320 Leu Gln Tyr Leu Arg Val Pro
Leu Val Asp Arg Ala Thr Cys Leu Arg 325 330 335 Ser Thr Lys Phe Thr
Ile Tyr Asn Asn Met Phe Cys Ala Gly Phe His 340 345 350 Glu Gly Gly
Arg Asp Ser Cys Gln Gly Asp Ser Gly Gly Pro His Val 355 360 365 370
Thr Glu Val Glu Gly Thr Ser Phe Leu Thr Gly Ile Ile Ser Trp Gly 375
380 385 Glu Glu Cys Ala Met Lys Gly Lys Tyr Gly Ile Tyr Thr Lys Val
Ser 390 395 400 Arg Tyr Val Asn Trp Ile Lys Glu Lys Thr Lys Leu Thr
Asp Lys Thr 405 410 415 His Thr Cys Pro Pro Cys Pro Ala Pro Glu Leu
Leu Gly Gly Pro Ser 420 425 430 Val Phe Leu Phe Pro Pro Lys Pro Lys
Asp Thr Leu Met Ile Ser Arg 435 440 445 450 Thr Pro Glu Val Thr Cys
Val Val Val Asp Val Ser His Glu Asp Pro 455 460 465 Glu Val Lys Phe
Asn Trp Tyr Val Asp Gly Val Glu Val His Asn Ala 470 475 480 Lys Thr
Lys Pro Arg Glu Glu Gln Tyr Asn Ser Thr Tyr Arg Val Val 485 490 495
Ser Val Leu Thr Val Leu His Gln Asp Trp Leu Asn Gly Lys Glu Tyr 500
505 510 Lys Cys Lys Val Ser Asn Lys Ala Leu Pro Ala Pro Ile Glu Lys
Thr 515 520 525 530 Ile Ser Lys Ala Lys Gly Gln Pro Arg Glu Pro Gln
Val Tyr Thr Leu 535 540 545 Pro Pro Ser Arg Asp Glu Leu Thr Lys Asn
Gln Val Ser Leu Thr Cys 550 555 560 Leu Val Lys Gly Phe Tyr Pro Ser
Asp Ile Ala Val Glu Trp Glu Ser 565 570 575 Asn Gly Gln Pro Glu Asn
Asn Tyr Lys Thr Thr Pro Pro Val Leu Asp 580 585 590 Ser Asp Gly Ser
Phe Phe Leu Tyr Ser Lys Leu Thr Val Asp Lys Ser 595 600 605 610 Arg
Trp Gln Gln Gly Asn Val Phe Ser Cys Ser Val Met His Glu Ala 615 620
625 Leu His Asn His Tyr Thr Gln Lys Ser Leu Ser Leu Ser Pro Gly Lys
630 635 640 <210> SEQ ID NO 3 <211> LENGTH: 741
<212> TYPE: DNA <213> ORGANISM: Artificial Sequence
<220> FEATURE: <223> OTHER INFORMATION: Fc cassette
from pSYN-FIX-030 <400> SEQUENCE: 3 atggagacag acacactcct
gctatgggta ctgctgctct gggttccagg ttccactggt 60 gacaaaactc
acacatgccc accgtgccca gcacctgaac tcctgggagg accgtcagtc 120
ttcctcttcc ccccaaaacc caaggacacc ctcatgatct cccggacccc tgaggtcaca
180 tgcgtggtgg tggacgtgag ccacgaagac cctgaggtca agttcaactg
gtacgtggac 240 ggcgtggagg tgcataatgc caagacaaag ccgcgggagg
agcagtacaa cagcacgtac 300 cgtgtggtca gcgtcctcac cgtcctgcac
caggactggc tgaatggcaa ggagtacaag 360 tgcaaggtct ccaacaaagc
cctcccagcc cccatcgaga aaaccatctc caaagccaaa 420 gggcagcccc
gagaaccaca ggtgtacacc ctgcccccat cccgcgatga gctgaccaag 480
aaccaggtca gcctgacctg cctggtcaaa ggcttctatc ccagcgacat cgccgtggag
540 tgggagagca atgggcagcc ggagaacaac tacaagacca cgcctcccgt
gttggactcc 600 gacggctcct tcttcctcta cagcaagctc accgtggaca
agagcaggtg gcagcagggg 660 aacgtcttct catgctccgt gatgcatgag
gctctgcaca accactacac gcagaagagc 720 ctctccctgt ctccgggtaa a 741
<210> SEQ ID NO 4 <211> LENGTH: 247 <212> TYPE:
PRT <213> ORGANISM: Artificial Sequence <220> FEATURE:
<223> OTHER INFORMATION: Fc cassette from pSYN-FIX-030
<220> FEATURE: <221> NAME/KEY: SIGNAL <222>
LOCATION: (-20)..(-1) <220> FEATURE: <221> NAME/KEY:
mat_peptide <222> LOCATION: (1)..(227) <400> SEQUENCE:
4 Met Glu Thr Asp Thr Leu Leu Leu Trp Val Leu Leu Leu Trp Val Pro
-20 -15 -10 -5 Gly Ser Thr Gly Asp Lys Thr His Thr Cys Pro Pro Cys
Pro Ala Pro -1 1 5 10 Glu Leu Leu Gly Gly Pro Ser Val Phe Leu Phe
Pro Pro Lys Pro Lys 15 20 25 Asp Thr Leu Met Ile Ser Arg Thr Pro
Glu Val Thr Cys Val Val Val 30 35 40 Asp Val Ser His Glu Asp Pro
Glu Val Lys Phe Asn Trp Tyr Val Asp 45 50 55 60 Gly Val Glu Val His
Asn Ala Lys Thr Lys Pro Arg Glu Glu Gln Tyr 65 70 75 Asn Ser Thr
Tyr Arg Val Val Ser Val Leu Thr Val Leu His Gln Asp 80 85 90 Trp
Leu Asn Gly Lys Glu Tyr Lys Cys Lys Val Ser Asn Lys Ala Leu 95 100
105 Pro Ala Pro Ile Glu Lys Thr Ile Ser Lys Ala Lys Gly Gln Pro Arg
110 115 120 Glu Pro Gln Val Tyr Thr Leu Pro Pro Ser Arg Asp Glu Leu
Thr Lys 125 130 135 140 Asn Gln Val Ser Leu Thr Cys Leu Val Lys Gly
Phe Tyr Pro Ser Asp 145 150 155
Ile Ala Val Glu Trp Glu Ser Asn Gly Gln Pro Glu Asn Asn Tyr Lys 160
165 170 Thr Thr Pro Pro Val Leu Asp Ser Asp Gly Ser Phe Phe Leu Tyr
Ser 175 180 185 Lys Leu Thr Val Asp Lys Ser Arg Trp Gln Gln Gly Asn
Val Phe Ser 190 195 200 Cys Ser Val Met His Glu Ala Leu His Asn His
Tyr Thr Gln Lys Ser 205 210 215 220 Leu Ser Leu Ser Pro Gly Lys 225
<210> SEQ ID NO 5 <211> LENGTH: 5052 <212> TYPE:
DNA <213> ORGANISM: Artificial Sequence <220> FEATURE:
<223> OTHER INFORMATION: B-Domain Deleted FVIIIFc <400>
SEQUENCE: 5 atgcaaatag agctctccac ctgcttcttt ctgtgccttt tgcgattctg
ctttagtgcc 60 accagaagat actacctggg tgcagtggaa ctgtcatggg
actatatgca aagtgatctc 120 ggtgagctgc ctgtggacgc aagatttcct
cctagagtgc caaaatcttt tccattcaac 180 acctcagtcg tgtacaaaaa
gactctgttt gtagaattca cggatcacct tttcaacatc 240 gctaagccaa
ggccaccctg gatgggtctg ctaggtccta ccatccaggc tgaggtttat 300
gatacagtgg tcattacact taagaacatg gcttcccatc ctgtcagtct tcatgctgtt
360 ggtgtatcct actggaaagc ttctgaggga gctgaatatg atgatcagac
cagtcaaagg 420 gagaaagaag atgataaagt cttccctggt ggaagccata
catatgtctg gcaggtcctg 480 aaagagaatg gtccaatggc ctctgaccca
ctgtgcctta cctactcata tctttctcat 540 gtggacctgg taaaagactt
gaattcaggc ctcattggag ccctactagt atgtagagaa 600 gggagtctgg
ccaaggaaaa gacacagacc ttgcacaaat ttatactact ttttgctgta 660
tttgatgaag ggaaaagttg gcactcagaa acaaagaact ccttgatgca ggatagggat
720 gctgcatctg ctcgggcctg gcctaaaatg cacacagtca atggttatgt
aaacaggtct 780 ctgccaggtc tgattggatg ccacaggaaa tcagtctatt
ggcatgtgat tggaatgggc 840 accactcctg aagtgcactc aatattcctc
gaaggtcaca catttcttgt gaggaaccat 900 cgccaggcgt ccttggaaat
ctcgccaata actttcctta ctgctcaaac actcttgatg 960 gaccttggac
agtttctact gttttgtcat atctcttccc accaacatga tggcatggaa 1020
gcttatgtca aagtagacag ctgtccagag gaaccccaac tacgaatgaa aaataatgaa
1080 gaagcggaag actatgatga tgatcttact gattctgaaa tggatgtggt
caggtttgat 1140 gatgacaact ctccttcctt tatccaaatt cgctcagttg
ccaagaagca tcctaaaact 1200 tgggtacatt acattgctgc tgaagaggag
gactgggact atgctccctt agtcctcgcc 1260 cccgatgaca gaagttataa
aagtcaatat ttgaacaatg gccctcagcg gattggtagg 1320 aagtacaaaa
aagtccgatt tatggcatac acagatgaaa cctttaagac tcgtgaagct 1380
attcagcatg aatcaggaat cttgggacct ttactttatg gggaagttgg agacacactg
1440 ttgattatat ttaagaatca agcaagcaga ccatataaca tctaccctca
cggaatcact 1500 gatgtccgtc ctttgtattc aaggagatta ccaaaaggtg
taaaacattt gaaggatttt 1560 ccaattctgc caggagaaat attcaaatat
aaatggacag tgactgtaga agatgggcca 1620 actaaatcag atcctcggtg
cctgacccgc tattactcta gtttcgttaa tatggagaga 1680 gatctagctt
caggactcat tggccctctc ctcatctgct acaaagaatc tgtagatcaa 1740
agaggaaacc agataatgtc agacaagagg aatgtcatcc tgttttctgt atttgatgag
1800 aaccgaagct ggtacctcac agagaatata caacgctttc tccccaatcc
agctggagtg 1860 cagcttgagg atccagagtt ccaagcctcc aacatcatgc
acagcatcaa tggctatgtt 1920 tttgatagtt tgcagttgtc agtttgtttg
catgaggtgg catactggta cattctaagc 1980 attggagcac agactgactt
cctttctgtc ttcttctctg gatatacctt caaacacaaa 2040 atggtctatg
aagacacact caccctattc ccattctcag gagaaactgt cttcatgtcg 2100
atggaaaacc caggtctatg gattctgggg tgccacaact cagactttcg gaacagaggc
2160 atgaccgcct tactgaaggt ttctagttgt gacaagaaca ctggtgatta
ttacgaggac 2220 agttatgaag atatttcagc atacttgctg agtaaaaaca
atgccattga accaagaagc 2280 ttctctcaaa acccaccagt cttgaaacgc
catcaacggg aaataactcg tactactctt 2340 cagtcagatc aagaggaaat
tgactatgat gataccatat cagttgaaat gaagaaggaa 2400 gattttgaca
tttatgatga ggatgaaaat cagagccccc gcagctttca aaagaaaaca 2460
cgacactatt ttattgctgc agtggagagg ctctgggatt atgggatgag tagctcccca
2520 catgttctaa gaaacagggc tcagagtggc agtgtccctc agttcaagaa
agttgttttc 2580 caggaattta ctgatggctc ctttactcag cccttatacc
gtggagaact aaatgaacat 2640 ttgggactcc tggggccata tataagagca
gaagttgaag ataatatcat ggtaactttc 2700 agaaatcagg cctctcgtcc
ctattccttc tattctagcc ttatttctta tgaggaagat 2760 cagaggcaag
gagcagaacc tagaaaaaac tttgtcaagc ctaatgaaac caaaacttac 2820
ttttggaaag tgcaacatca tatggcaccc actaaagatg agtttgactg caaagcctgg
2880 gcttatttct ctgatgttga cctggaaaaa gatgtgcact caggcctgat
tggacccctt 2940 ctggtctgcc acactaacac actgaaccct gctcatggga
gacaagtgac agtacaggaa 3000 tttgctctgt ttttcaccat ctttgatgag
accaaaagct ggtacttcac tgaaaatatg 3060 gaaagaaact gcagggctcc
ctgcaatatc cagatggaag atcccacttt taaagagaat 3120 tatcgcttcc
atgcaatcaa tggctacata atggatacac tacctggctt agtaatggct 3180
caggatcaaa ggattcgatg gtatctgctc agcatgggca gcaatgaaaa catccattct
3240 attcatttca gtggacatgt gttcactgta cgaaaaaaag aggagtataa
aatggcactg 3300 tacaatctct atccaggtgt ttttgagaca gtggaaatgt
taccatccaa agctggaatt 3360 tggcgggtgg aatgccttat tggcgagcat
ctacatgctg ggatgagcac actttttctg 3420 gtgtacagca ataagtgtca
gactcccctg ggaatggctt ctggacacat tagagatttt 3480 cagattacag
cttcaggaca atatggacag tgggccccaa agctggccag acttcattat 3540
tccggatcaa tcaatgcctg gagcaccaag gagccctttt cttggatcaa ggtggatctg
3600 ttggcaccaa tgattattca cggcatcaag acccagggtg cccgtcagaa
gttctccagc 3660 ctctacatct ctcagtttat catcatgtat agtcttgatg
ggaagaagtg gcagacttat 3720 cgaggaaatt ccactggaac cttaatggtc
ttctttggca atgtggattc atctgggata 3780 aaacacaata tttttaaccc
tccaattatt gctcgataca tccgtttgca cccaactcat 3840 tatagcattc
gcagcactct tcgcatggag ttgatgggct gtgatttaaa tagttgcagc 3900
atgccattgg gaatggagag taaagcaata tcagatgcac agattactgc ttcatcctac
3960 tttaccaata tgtttgccac ctggtctcct tcaaaagctc gacttcacct
ccaagggagg 4020 agtaatgcct ggagacctca ggtgaataat ccaaaagagt
ggctgcaagt ggacttccag 4080 aagacaatga aagtcacagg agtaactact
cagggagtaa aatctctgct taccagcatg 4140 tatgtgaagg agttcctcat
ctccagcagt caagatggcc atcagtggac tctctttttt 4200 cagaatggca
aagtaaaggt ttttcaggga aatcaagact ccttcacacc tgtggtgaac 4260
tctctagacc caccgttact gactcgctac cttcgaattc acccccagag ttgggtgcac
4320 cagattgccc tgaggatgga ggttctgggc tgcgaggcac aggacctcta
cgacaaaact 4380 cacacatgcc caccgtgccc agctccagaa ctcctgggcg
gaccgtcagt cttcctcttc 4440 cccccaaaac ccaaggacac cctcatgatc
tcccggaccc ctgaggtcac atgcgtggtg 4500 gtggacgtga gccacgaaga
ccctgaggtc aagttcaact ggtacgtgga cggcgtggag 4560 gtgcataatg
ccaagacaaa gccgcgggag gagcagtaca acagcacgta ccgtgtggtc 4620
agcgtcctca ccgtcctgca ccaggactgg ctgaatggca aggagtacaa gtgcaaggtc
4680 tccaacaaag ccctcccagc ccccatcgag aaaaccatct ccaaagccaa
agggcagccc 4740 cgagaaccac aggtgtacac cctgccccca tcccgggatg
agctgaccaa gaaccaggtc 4800 agcctgacct gcctggtcaa aggcttctat
cccagcgaca tcgccgtgga gtgggagagc 4860 aatgggcagc cggagaacaa
ctacaagacc acgcctcccg tgttggactc cgacggctcc 4920 ttcttcctct
acagcaagct caccgtggac aagagcaggt ggcagcaggg gaacgtcttc 4980
tcatgctccg tgatgcatga ggctctgcac aaccactaca cgcagaagag cctctccctg
5040 tctccgggta aa 5052 <210> SEQ ID NO 6 <211> LENGTH:
1684 <212> TYPE: PRT <213> ORGANISM: Artificial
Sequence <220> FEATURE: <223> OTHER INFORMATION:
B-Domain Deleted FVIIIFc <220> FEATURE: <221> NAME/KEY:
SIGNAL <222> LOCATION: (-19)..(-1) <220> FEATURE:
<221> NAME/KEY: mat_peptide <222> LOCATION: (1)..(1665)
<400> SEQUENCE: 6 Met Gln Ile Glu Leu Ser Thr Cys Phe Phe Leu
Cys Leu Leu Arg Phe -15 -10 -5 Cys Phe Ser Ala Thr Arg Arg Tyr Tyr
Leu Gly Ala Val Glu Leu Ser -1 1 5 10 Trp Asp Tyr Met Gln Ser Asp
Leu Gly Glu Leu Pro Val Asp Ala Arg 15 20 25 Phe Pro Pro Arg Val
Pro Lys Ser Phe Pro Phe Asn Thr Ser Val Val 30 35 40 45 Tyr Lys Lys
Thr Leu Phe Val Glu Phe Thr Asp His Leu Phe Asn Ile 50 55 60 Ala
Lys Pro Arg Pro Pro Trp Met Gly Leu Leu Gly Pro Thr Ile Gln 65 70
75 Ala Glu Val Tyr Asp Thr Val Val Ile Thr Leu Lys Asn Met Ala Ser
80 85 90 His Pro Val Ser Leu His Ala Val Gly Val Ser Tyr Trp Lys
Ala Ser 95 100 105 Glu Gly Ala Glu Tyr Asp Asp Gln Thr Ser Gln Arg
Glu Lys Glu Asp 110 115 120 125 Asp Lys Val Phe Pro Gly Gly Ser His
Thr Tyr Val Trp Gln Val Leu 130 135 140 Lys Glu Asn Gly Pro Met Ala
Ser Asp Pro Leu Cys Leu Thr Tyr Ser 145 150 155 Tyr Leu Ser His Val
Asp Leu Val Lys Asp Leu Asn Ser Gly Leu Ile 160 165 170 Gly Ala Leu
Leu Val Cys Arg Glu Gly Ser Leu Ala Lys Glu Lys Thr 175 180 185
Gln Thr Leu His Lys Phe Ile Leu Leu Phe Ala Val Phe Asp Glu Gly 190
195 200 205 Lys Ser Trp His Ser Glu Thr Lys Asn Ser Leu Met Gln Asp
Arg Asp 210 215 220 Ala Ala Ser Ala Arg Ala Trp Pro Lys Met His Thr
Val Asn Gly Tyr 225 230 235 Val Asn Arg Ser Leu Pro Gly Leu Ile Gly
Cys His Arg Lys Ser Val 240 245 250 Tyr Trp His Val Ile Gly Met Gly
Thr Thr Pro Glu Val His Ser Ile 255 260 265 Phe Leu Glu Gly His Thr
Phe Leu Val Arg Asn His Arg Gln Ala Ser 270 275 280 285 Leu Glu Ile
Ser Pro Ile Thr Phe Leu Thr Ala Gln Thr Leu Leu Met 290 295 300 Asp
Leu Gly Gln Phe Leu Leu Phe Cys His Ile Ser Ser His Gln His 305 310
315 Asp Gly Met Glu Ala Tyr Val Lys Val Asp Ser Cys Pro Glu Glu Pro
320 325 330 Gln Leu Arg Met Lys Asn Asn Glu Glu Ala Glu Asp Tyr Asp
Asp Asp 335 340 345 Leu Thr Asp Ser Glu Met Asp Val Val Arg Phe Asp
Asp Asp Asn Ser 350 355 360 365 Pro Ser Phe Ile Gln Ile Arg Ser Val
Ala Lys Lys His Pro Lys Thr 370 375 380 Trp Val His Tyr Ile Ala Ala
Glu Glu Glu Asp Trp Asp Tyr Ala Pro 385 390 395 Leu Val Leu Ala Pro
Asp Asp Arg Ser Tyr Lys Ser Gln Tyr Leu Asn 400 405 410 Asn Gly Pro
Gln Arg Ile Gly Arg Lys Tyr Lys Lys Val Arg Phe Met 415 420 425 Ala
Tyr Thr Asp Glu Thr Phe Lys Thr Arg Glu Ala Ile Gln His Glu 430 435
440 445 Ser Gly Ile Leu Gly Pro Leu Leu Tyr Gly Glu Val Gly Asp Thr
Leu 450 455 460 Leu Ile Ile Phe Lys Asn Gln Ala Ser Arg Pro Tyr Asn
Ile Tyr Pro 465 470 475 His Gly Ile Thr Asp Val Arg Pro Leu Tyr Ser
Arg Arg Leu Pro Lys 480 485 490 Gly Val Lys His Leu Lys Asp Phe Pro
Ile Leu Pro Gly Glu Ile Phe 495 500 505 Lys Tyr Lys Trp Thr Val Thr
Val Glu Asp Gly Pro Thr Lys Ser Asp 510 515 520 525 Pro Arg Cys Leu
Thr Arg Tyr Tyr Ser Ser Phe Val Asn Met Glu Arg 530 535 540 Asp Leu
Ala Ser Gly Leu Ile Gly Pro Leu Leu Ile Cys Tyr Lys Glu 545 550 555
Ser Val Asp Gln Arg Gly Asn Gln Ile Met Ser Asp Lys Arg Asn Val 560
565 570 Ile Leu Phe Ser Val Phe Asp Glu Asn Arg Ser Trp Tyr Leu Thr
Glu 575 580 585 Asn Ile Gln Arg Phe Leu Pro Asn Pro Ala Gly Val Gln
Leu Glu Asp 590 595 600 605 Pro Glu Phe Gln Ala Ser Asn Ile Met His
Ser Ile Asn Gly Tyr Val 610 615 620 Phe Asp Ser Leu Gln Leu Ser Val
Cys Leu His Glu Val Ala Tyr Trp 625 630 635 Tyr Ile Leu Ser Ile Gly
Ala Gln Thr Asp Phe Leu Ser Val Phe Phe 640 645 650 Ser Gly Tyr Thr
Phe Lys His Lys Met Val Tyr Glu Asp Thr Leu Thr 655 660 665 Leu Phe
Pro Phe Ser Gly Glu Thr Val Phe Met Ser Met Glu Asn Pro 670 675 680
685 Gly Leu Trp Ile Leu Gly Cys His Asn Ser Asp Phe Arg Asn Arg Gly
690 695 700 Met Thr Ala Leu Leu Lys Val Ser Ser Cys Asp Lys Asn Thr
Gly Asp 705 710 715 Tyr Tyr Glu Asp Ser Tyr Glu Asp Ile Ser Ala Tyr
Leu Leu Ser Lys 720 725 730 Asn Asn Ala Ile Glu Pro Arg Ser Phe Ser
Gln Asn Pro Pro Val Leu 735 740 745 Lys Arg His Gln Arg Glu Ile Thr
Arg Thr Thr Leu Gln Ser Asp Gln 750 755 760 765 Glu Glu Ile Asp Tyr
Asp Asp Thr Ile Ser Val Glu Met Lys Lys Glu 770 775 780 Asp Phe Asp
Ile Tyr Asp Glu Asp Glu Asn Gln Ser Pro Arg Ser Phe 785 790 795 Gln
Lys Lys Thr Arg His Tyr Phe Ile Ala Ala Val Glu Arg Leu Trp 800 805
810 Asp Tyr Gly Met Ser Ser Ser Pro His Val Leu Arg Asn Arg Ala Gln
815 820 825 Ser Gly Ser Val Pro Gln Phe Lys Lys Val Val Phe Gln Glu
Phe Thr 830 835 840 845 Asp Gly Ser Phe Thr Gln Pro Leu Tyr Arg Gly
Glu Leu Asn Glu His 850 855 860 Leu Gly Leu Leu Gly Pro Tyr Ile Arg
Ala Glu Val Glu Asp Asn Ile 865 870 875 Met Val Thr Phe Arg Asn Gln
Ala Ser Arg Pro Tyr Ser Phe Tyr Ser 880 885 890 Ser Leu Ile Ser Tyr
Glu Glu Asp Gln Arg Gln Gly Ala Glu Pro Arg 895 900 905 Lys Asn Phe
Val Lys Pro Asn Glu Thr Lys Thr Tyr Phe Trp Lys Val 910 915 920 925
Gln His His Met Ala Pro Thr Lys Asp Glu Phe Asp Cys Lys Ala Trp 930
935 940 Ala Tyr Phe Ser Asp Val Asp Leu Glu Lys Asp Val His Ser Gly
Leu 945 950 955 Ile Gly Pro Leu Leu Val Cys His Thr Asn Thr Leu Asn
Pro Ala His 960 965 970 Gly Arg Gln Val Thr Val Gln Glu Phe Ala Leu
Phe Phe Thr Ile Phe 975 980 985 Asp Glu Thr Lys Ser Trp Tyr Phe Thr
Glu Asn Met Glu Arg Asn Cys 990 995 1000 1005 Arg Ala Pro Cys Asn
Ile Gln Met Glu Asp Pro Thr Phe Lys Glu 1010 1015 1020 Asn Tyr Arg
Phe His Ala Ile Asn Gly Tyr Ile Met Asp Thr Leu 1025 1030 1035 Pro
Gly Leu Val Met Ala Gln Asp Gln Arg Ile Arg Trp Tyr Leu 1040 1045
1050 Leu Ser Met Gly Ser Asn Glu Asn Ile His Ser Ile His Phe Ser
1055 1060 1065 Gly His Val Phe Thr Val Arg Lys Lys Glu Glu Tyr Lys
Met Ala 1070 1075 1080 Leu Tyr Asn Leu Tyr Pro Gly Val Phe Glu Thr
Val Glu Met Leu 1085 1090 1095 Pro Ser Lys Ala Gly Ile Trp Arg Val
Glu Cys Leu Ile Gly Glu 1100 1105 1110 His Leu His Ala Gly Met Ser
Thr Leu Phe Leu Val Tyr Ser Asn 1115 1120 1125 Lys Cys Gln Thr Pro
Leu Gly Met Ala Ser Gly His Ile Arg Asp 1130 1135 1140 Phe Gln Ile
Thr Ala Ser Gly Gln Tyr Gly Gln Trp Ala Pro Lys 1145 1150 1155 Leu
Ala Arg Leu His Tyr Ser Gly Ser Ile Asn Ala Trp Ser Thr 1160 1165
1170 Lys Glu Pro Phe Ser Trp Ile Lys Val Asp Leu Leu Ala Pro Met
1175 1180 1185 Ile Ile His Gly Ile Lys Thr Gln Gly Ala Arg Gln Lys
Phe Ser 1190 1195 1200 Ser Leu Tyr Ile Ser Gln Phe Ile Ile Met Tyr
Ser Leu Asp Gly 1205 1210 1215 Lys Lys Trp Gln Thr Tyr Arg Gly Asn
Ser Thr Gly Thr Leu Met 1220 1225 1230 Val Phe Phe Gly Asn Val Asp
Ser Ser Gly Ile Lys His Asn Ile 1235 1240 1245 Phe Asn Pro Pro Ile
Ile Ala Arg Tyr Ile Arg Leu His Pro Thr 1250 1255 1260 His Tyr Ser
Ile Arg Ser Thr Leu Arg Met Glu Leu Met Gly Cys 1265 1270 1275 Asp
Leu Asn Ser Cys Ser Met Pro Leu Gly Met Glu Ser Lys Ala 1280 1285
1290 Ile Ser Asp Ala Gln Ile Thr Ala Ser Ser Tyr Phe Thr Asn Met
1295 1300 1305 Phe Ala Thr Trp Ser Pro Ser Lys Ala Arg Leu His Leu
Gln Gly 1310 1315 1320 Arg Ser Asn Ala Trp Arg Pro Gln Val Asn Asn
Pro Lys Glu Trp 1325 1330 1335 Leu Gln Val Asp Phe Gln Lys Thr Met
Lys Val Thr Gly Val Thr 1340 1345 1350 Thr Gln Gly Val Lys Ser Leu
Leu Thr Ser Met Tyr Val Lys Glu 1355 1360 1365 Phe Leu Ile Ser Ser
Ser Gln Asp Gly His Gln Trp Thr Leu Phe 1370 1375 1380 Phe Gln Asn
Gly Lys Val Lys Val Phe Gln Gly Asn Gln Asp Ser 1385 1390 1395 Phe
Thr Pro Val Val Asn Ser Leu Asp Pro Pro Leu Leu Thr Arg 1400 1405
1410 Tyr Leu Arg Ile His Pro Gln Ser Trp Val His Gln Ile Ala Leu
1415 1420 1425 Arg Met Glu Val Leu Gly Cys Glu Ala Gln Asp Leu Tyr
Asp Lys 1430 1435 1440 Thr His Thr Cys Pro Pro Cys Pro Ala Pro Glu
Leu Leu Gly Gly 1445 1450 1455 Pro Ser Val Phe Leu Phe Pro Pro Lys
Pro Lys Asp Thr Leu Met 1460 1465 1470 Ile Ser Arg Thr Pro Glu Val
Thr Cys Val Val Val Asp Val Ser 1475 1480 1485 His Glu Asp Pro Glu
Val Lys Phe Asn Trp Tyr Val Asp Gly Val 1490 1495 1500
Glu Val His Asn Ala Lys Thr Lys Pro Arg Glu Glu Gln Tyr Asn 1505
1510 1515 Ser Thr Tyr Arg Val Val Ser Val Leu Thr Val Leu His Gln
Asp 1520 1525 1530 Trp Leu Asn Gly Lys Glu Tyr Lys Cys Lys Val Ser
Asn Lys Ala 1535 1540 1545 Leu Pro Ala Pro Ile Glu Lys Thr Ile Ser
Lys Ala Lys Gly Gln 1550 1555 1560 Pro Arg Glu Pro Gln Val Tyr Thr
Leu Pro Pro Ser Arg Asp Glu 1565 1570 1575 Leu Thr Lys Asn Gln Val
Ser Leu Thr Cys Leu Val Lys Gly Phe 1580 1585 1590 Tyr Pro Ser Asp
Ile Ala Val Glu Trp Glu Ser Asn Gly Gln Pro 1595 1600 1605 Glu Asn
Asn Tyr Lys Thr Thr Pro Pro Val Leu Asp Ser Asp Gly 1610 1615 1620
Ser Phe Phe Leu Tyr Ser Lys Leu Thr Val Asp Lys Ser Arg Trp 1625
1630 1635 Gln Gln Gly Asn Val Phe Ser Cys Ser Val Met His Glu Ala
Leu 1640 1645 1650 His Asn His Tyr Thr Gln Lys Ser Leu Ser Leu Ser
Pro Gly Lys 1655 1660 1665 <210> SEQ ID NO 7 <211>
LENGTH: 741 <212> TYPE: DNA <213> ORGANISM: Artificial
Sequence <220> FEATURE: <223> OTHER INFORMATION: Fc
Sequence <400> SEQUENCE: 7 atggagacag acacactcct gctatgggta
ctgctgctct gggttccagg ttccactggt 60 gacaaaactc acacatgccc
accgtgccca gcacctgaac tcctgggagg accgtcagtc 120 ttcctcttcc
ccccaaaacc caaggacacc ctcatgatct cccggacccc tgaggtcaca 180
tgcgtggtgg tggacgtgag ccacgaagac cctgaggtca agttcaactg gtacgtggac
240 ggcgtggagg tgcataatgc caagacaaag ccgcgggagg agcagtacaa
cagcacgtac 300 cgtgtggtca gcgtcctcac cgtcctgcac caggactggc
tgaatggcaa ggagtacaag 360 tgcaaggtct ccaacaaagc cctcccagcc
cccatcgaga aaaccatctc caaagccaaa 420 gggcagcccc gagaaccaca
ggtgtacacc ctgcccccat cccgcgatga gctgaccaag 480 aaccaggtca
gcctgacctg cctggtcaaa ggcttctatc ccagcgacat cgccgtggag 540
tgggagagca atgggcagcc ggagaacaac tacaagacca cgcctcccgt gttggactcc
600 gacggctcct tcttcctcta cagcaagctc accgtggaca agagcaggtg
gcagcagggg 660 aacgtcttct catgctccgt gatgcatgag gctctgcaca
accactacac gcagaagagc 720 ctctccctgt ctccgggtaa a 741 <210>
SEQ ID NO 8 <211> LENGTH: 247 <212> TYPE: PRT
<213> ORGANISM: Artificial Sequence <220> FEATURE:
<223> OTHER INFORMATION: Fc chain <220> FEATURE:
<221> NAME/KEY: SIGNAL <222> LOCATION: (-20)..(-1)
<220> FEATURE: <221> NAME/KEY: mat_peptide <222>
LOCATION: (-1)..(227) <400> SEQUENCE: 8 Met Glu Thr Asp Thr
Leu Leu Leu Trp Val Leu Leu Leu Trp Val Pro -20 -15 -10 -5 Gly Ser
Thr Gly Asp Lys Thr His Thr Cys Pro Pro Cys Pro Ala Pro -1 1 5 10
Glu Leu Leu Gly Gly Pro Ser Val Phe Leu Phe Pro Pro Lys Pro Lys 15
20 25 Asp Thr Leu Met Ile Ser Arg Thr Pro Glu Val Thr Cys Val Val
Val 30 35 40 Asp Val Ser His Glu Asp Pro Glu Val Lys Phe Asn Trp
Tyr Val Asp 45 50 55 60 Gly Val Glu Val His Asn Ala Lys Thr Lys Pro
Arg Glu Glu Gln Tyr 65 70 75 Asn Ser Thr Tyr Arg Val Val Ser Val
Leu Thr Val Leu His Gln Asp 80 85 90 Trp Leu Asn Gly Lys Glu Tyr
Lys Cys Lys Val Ser Asn Lys Ala Leu 95 100 105 Pro Ala Pro Ile Glu
Lys Thr Ile Ser Lys Ala Lys Gly Gln Pro Arg 110 115 120 Glu Pro Gln
Val Tyr Thr Leu Pro Pro Ser Arg Asp Glu Leu Thr Lys 125 130 135 140
Asn Gln Val Ser Leu Thr Cys Leu Val Lys Gly Phe Tyr Pro Ser Asp 145
150 155 Ile Ala Val Glu Trp Glu Ser Asn Gly Gln Pro Glu Asn Asn Tyr
Lys 160 165 170 Thr Thr Pro Pro Val Leu Asp Ser Asp Gly Ser Phe Phe
Leu Tyr Ser 175 180 185 Lys Leu Thr Val Asp Lys Ser Arg Trp Gln Gln
Gly Asn Val Phe Ser 190 195 200 Cys Ser Val Met His Glu Ala Leu His
Asn His Tyr Thr Gln Lys Ser 205 210 215 220 Leu Ser Leu Ser Pro Gly
Lys 225 <210> SEQ ID NO 9 <211> LENGTH: 7734
<212> TYPE: DNA <213> ORGANISM: Artificial Sequence
<220> FEATURE: <223> OTHER INFORMATION: Full Length
FVIIIFc <400> SEQUENCE: 9 atgcaaatag agctctccac ctgcttcttt
ctgtgccttt tgcgattctg ctttagtgcc 60 accagaagat actacctggg
tgcagtggaa ctgtcatggg actatatgca aagtgatctc 120 ggtgagctgc
ctgtggacgc aagatttcct cctagagtgc caaaatcttt tccattcaac 180
acctcagtcg tgtacaaaaa gactctgttt gtagaattca cggatcacct tttcaacatc
240 gctaagccaa ggccaccctg gatgggtctg ctaggtccta ccatccaggc
tgaggtttat 300 gatacagtgg tcattacact taagaacatg gcttcccatc
ctgtcagtct tcatgctgtt 360 ggtgtatcct actggaaagc ttctgaggga
gctgaatatg atgatcagac cagtcaaagg 420 gagaaagaag atgataaagt
cttccctggt ggaagccata catatgtctg gcaggtcctg 480 aaagagaatg
gtccaatggc ctctgaccca ctgtgcctta cctactcata tctttctcat 540
gtggacctgg taaaagactt gaattcaggc ctcattggag ccctactagt atgtagagaa
600 gggagtctgg ccaaggaaaa gacacagacc ttgcacaaat ttatactact
ttttgctgta 660 tttgatgaag ggaaaagttg gcactcagaa acaaagaact
ccttgatgca ggatagggat 720 gctgcatctg ctcgggcctg gcctaaaatg
cacacagtca atggttatgt aaacaggtct 780 ctgccaggtc tgattggatg
ccacaggaaa tcagtctatt ggcatgtgat tggaatgggc 840 accactcctg
aagtgcactc aatattcctc gaaggtcaca catttcttgt gaggaaccat 900
cgccaggcgt ccttggaaat ctcgccaata actttcctta ctgctcaaac actcttgatg
960 gaccttggac agtttctact gttttgtcat atctcttccc accaacatga
tggcatggaa 1020 gcttatgtca aagtagacag ctgtccagag gaaccccaac
tacgaatgaa aaataatgaa 1080 gaagcggaag actatgatga tgatcttact
gattctgaaa tggatgtggt caggtttgat 1140 gatgacaact ctccttcctt
tatccaaatt cgctcagttg ccaagaagca tcctaaaact 1200 tgggtacatt
acattgctgc tgaagaggag gactgggact atgctccctt agtcctcgcc 1260
cccgatgaca gaagttataa aagtcaatat ttgaacaatg gccctcagcg gattggtagg
1320 aagtacaaaa aagtccgatt tatggcatac acagatgaaa cctttaagac
tcgtgaagct 1380 attcagcatg aatcaggaat cttgggacct ttactttatg
gggaagttgg agacacactg 1440 ttgattatat ttaagaatca agcaagcaga
ccatataaca tctaccctca cggaatcact 1500 gatgtccgtc ctttgtattc
aaggagatta ccaaaaggtg taaaacattt gaaggatttt 1560 ccaattctgc
caggagaaat attcaaatat aaatggacag tgactgtaga agatgggcca 1620
actaaatcag atcctcggtg cctgacccgc tattactcta gtttcgttaa tatggagaga
1680 gatctagctt caggactcat tggccctctc ctcatctgct acaaagaatc
tgtagatcaa 1740 agaggaaacc agataatgtc agacaagagg aatgtcatcc
tgttttctgt atttgatgag 1800 aaccgaagct ggtacctcac agagaatata
caacgctttc tccccaatcc agctggagtg 1860 cagcttgagg atccagagtt
ccaagcctcc aacatcatgc acagcatcaa tggctatgtt 1920 tttgatagtt
tgcagttgtc agtttgtttg catgaggtgg catactggta cattctaagc 1980
attggagcac agactgactt cctttctgtc ttcttctctg gatatacctt caaacacaaa
2040 atggtctatg aagacacact caccctattc ccattctcag gagaaactgt
cttcatgtcg 2100 atggaaaacc caggtctatg gattctgggg tgccacaact
cagactttcg gaacagaggc 2160 atgaccgcct tactgaaggt ttctagttgt
gacaagaaca ctggtgatta ttacgaggac 2220 agttatgaag atatttcagc
atacttgctg agtaaaaaca atgccattga accaagaagc 2280 ttctcccaga
attcaagaca ccctagcact aggcaaaagc aatttaatgc caccacaatt 2340
ccagaaaatg acatagagaa gactgaccct tggtttgcac acagaacacc tatgcctaaa
2400 atacaaaatg tctcctctag tgatttgttg atgctcttgc gacagagtcc
tactccacat 2460 gggctatcct tatctgatct ccaagaagcc aaatatgaga
ctttttctga tgatccatca 2520 cctggagcaa tagacagtaa taacagcctg
tctgaaatga cacacttcag gccacagctc 2580 catcacagtg gggacatggt
atttacccct gagtcaggcc tccaattaag attaaatgag 2640 aaactgggga
caactgcagc aacagagttg aagaaacttg atttcaaagt ttctagtaca 2700
tcaaataatc tgatttcaac aattccatca gacaatttgg cagcaggtac tgataataca
2760 agttccttag gacccccaag tatgccagtt cattatgata gtcaattaga
taccactcta 2820 tttggcaaaa agtcatctcc ccttactgag tctggtggac
ctctgagctt gagtgaagaa 2880 aataatgatt caaagttgtt agaatcaggt
ttaatgaata gccaagaaag ttcatgggga 2940 aaaaatgtat cgtcaacaga
gagtggtagg ttatttaaag ggaaaagagc tcatggacct 3000 gctttgttga
ctaaagataa tgccttattc aaagttagca tctctttgtt aaagacaaac 3060
aaaacttcca ataattcagc aactaataga aagactcaca ttgatggccc atcattatta
3120 attgagaata gtccatcagt ctggcaaaat atattagaaa gtgacactga
gtttaaaaaa 3180 gtgacacctt tgattcatga cagaatgctt atggacaaaa
atgctacagc tttgaggcta 3240
aatcatatgt caaataaaac tacttcatca aaaaacatgg aaatggtcca acagaaaaaa
3300 gagggcccca ttccaccaga tgcacaaaat ccagatatgt cgttctttaa
gatgctattc 3360 ttgccagaat cagcaaggtg gatacaaagg actcatggaa
agaactctct gaactctggg 3420 caaggcccca gtccaaagca attagtatcc
ttaggaccag aaaaatctgt ggaaggtcag 3480 aatttcttgt ctgagaaaaa
caaagtggta gtaggaaagg gtgaatttac aaaggacgta 3540 ggactcaaag
agatggtttt tccaagcagc agaaacctat ttcttactaa cttggataat 3600
ttacatgaaa ataatacaca caatcaagaa aaaaaaattc aggaagaaat agaaaagaag
3660 gaaacattaa tccaagagaa tgtagttttg cctcagatac atacagtgac
tggcactaag 3720 aatttcatga agaacctttt cttactgagc actaggcaaa
atgtagaagg ttcatatgac 3780 ggggcatatg ctccagtact tcaagatttt
aggtcattaa atgattcaac aaatagaaca 3840 aagaaacaca cagctcattt
ctcaaaaaaa ggggaggaag aaaacttgga aggcttggga 3900 aatcaaacca
agcaaattgt agagaaatat gcatgcacca caaggatatc tcctaataca 3960
agccagcaga attttgtcac gcaacgtagt aagagagctt tgaaacaatt cagactccca
4020 ctagaagaaa cagaacttga aaaaaggata attgtggatg acacctcaac
ccagtggtcc 4080 aaaaacatga aacatttgac cccgagcacc ctcacacaga
tagactacaa tgagaaggag 4140 aaaggggcca ttactcagtc tcccttatca
gattgcctta cgaggagtca tagcatccct 4200 caagcaaata gatctccatt
acccattgca aaggtatcat catttccatc tattagacct 4260 atatatctga
ccagggtcct attccaagac aactcttctc atcttccagc agcatcttat 4320
agaaagaaag attctggggt ccaagaaagc agtcatttct tacaaggagc caaaaaaaat
4380 aacctttctt tagccattct aaccttggag atgactggtg atcaaagaga
ggttggctcc 4440 ctggggacaa gtgccacaaa ttcagtcaca tacaagaaag
ttgagaacac tgttctcccg 4500 aaaccagact tgcccaaaac atctggcaaa
gttgaattgc ttccaaaagt tcacatttat 4560 cagaaggacc tattccctac
ggaaactagc aatgggtctc ctggccatct ggatctcgtg 4620 gaagggagcc
ttcttcaggg aacagaggga gcgattaagt ggaatgaagc aaacagacct 4680
ggaaaagttc cctttctgag agtagcaaca gaaagctctg caaagactcc ctccaagcta
4740 ttggatcctc ttgcttggga taaccactat ggtactcaga taccaaaaga
agagtggaaa 4800 tcccaagaga agtcaccaga aaaaacagct tttaagaaaa
aggataccat tttgtccctg 4860 aacgcttgtg aaagcaatca tgcaatagca
gcaataaatg agggacaaaa taagcccgaa 4920 atagaagtca cctgggcaaa
gcaaggtagg actgaaaggc tgtgctctca aaacccacca 4980 gtcttgaaac
gccatcaacg ggaaataact cgtactactc ttcagtcaga tcaagaggaa 5040
attgactatg atgataccat atcagttgaa atgaagaagg aagattttga catttatgat
5100 gaggatgaaa atcagagccc ccgcagcttt caaaagaaaa cacgacacta
ttttattgct 5160 gcagtggaga ggctctggga ttatgggatg agtagctccc
cacatgttct aagaaacagg 5220 gctcagagtg gcagtgtccc tcagttcaag
aaagttgttt tccaggaatt tactgatggc 5280 tcctttactc agcccttata
ccgtggagaa ctaaatgaac atttgggact cctggggcca 5340 tatataagag
cagaagttga agataatatc atggtaactt tcagaaatca ggcctctcgt 5400
ccctattcct tctattctag ccttatttct tatgaggaag atcagaggca aggagcagaa
5460 cctagaaaaa actttgtcaa gcctaatgaa accaaaactt acttttggaa
agtgcaacat 5520 catatggcac ccactaaaga tgagtttgac tgcaaagcct
gggcttattt ctctgatgtt 5580 gacctggaaa aagatgtgca ctcaggcctg
attggacccc ttctggtctg ccacactaac 5640 acactgaacc ctgctcatgg
gagacaagtg acagtacagg aatttgctct gtttttcacc 5700 atctttgatg
agaccaaaag ctggtacttc actgaaaata tggaaagaaa ctgcagggct 5760
ccctgcaata tccagatgga agatcccact tttaaagaga attatcgctt ccatgcaatc
5820 aatggctaca taatggatac actacctggc ttagtaatgg ctcaggatca
aaggattcga 5880 tggtatctgc tcagcatggg cagcaatgaa aacatccatt
ctattcattt cagtggacat 5940 gtgttcactg tacgaaaaaa agaggagtat
aaaatggcac tgtacaatct ctatccaggt 6000 gtttttgaga cagtggaaat
gttaccatcc aaagctggaa tttggcgggt ggaatgcctt 6060 attggcgagc
atctacatgc tgggatgagc acactttttc tggtgtacag caataagtgt 6120
cagactcccc tgggaatggc ttctggacac attagagatt ttcagattac agcttcagga
6180 caatatggac agtgggcccc aaagctggcc agacttcatt attccggatc
aatcaatgcc 6240 tggagcacca aggagccctt ttcttggatc aaggtggatc
tgttggcacc aatgattatt 6300 cacggcatca agacccaggg tgcccgtcag
aagttctcca gcctctacat ctctcagttt 6360 atcatcatgt atagtcttga
tgggaagaag tggcagactt atcgaggaaa ttccactgga 6420 accttaatgg
tcttctttgg caatgtggat tcatctggga taaaacacaa tatttttaac 6480
cctccaatta ttgctcgata catccgtttg cacccaactc attatagcat tcgcagcact
6540 cttcgcatgg agttgatggg ctgtgattta aatagttgca gcatgccatt
gggaatggag 6600 agtaaagcaa tatcagatgc acagattact gcttcatcct
actttaccaa tatgtttgcc 6660 acctggtctc cttcaaaagc tcgacttcac
ctccaaggga ggagtaatgc ctggagacct 6720 caggtgaata atccaaaaga
gtggctgcaa gtggacttcc agaagacaat gaaagtcaca 6780 ggagtaacta
ctcagggagt aaaatctctg cttaccagca tgtatgtgaa ggagttcctc 6840
atctccagca gtcaagatgg ccatcagtgg actctctttt ttcagaatgg caaagtaaag
6900 gtttttcagg gaaatcaaga ctccttcaca cctgtggtga actctctaga
cccaccgtta 6960 ctgactcgct accttcgaat tcacccccag agttgggtgc
accagattgc cctgaggatg 7020 gaggttctgg gctgcgaggc acaggacctc
tacgacaaaa ctcacacatg cccaccgtgc 7080 ccagctccag aactcctggg
cggaccgtca gtcttcctct tccccccaaa acccaaggac 7140 accctcatga
tctcccggac ccctgaggtc acatgcgtgg tggtggacgt gagccacgaa 7200
gaccctgagg tcaagttcaa ctggtacgtg gacggcgtgg aggtgcataa tgccaagaca
7260 aagccgcggg aggagcagta caacagcacg taccgtgtgg tcagcgtcct
caccgtcctg 7320 caccaggact ggctgaatgg caaggagtac aagtgcaagg
tctccaacaa agccctccca 7380 gcccccatcg agaaaaccat ctccaaagcc
aaagggcagc cccgagaacc acaggtgtac 7440 accctgcccc catcccggga
tgagctgacc aagaaccagg tcagcctgac ctgcctggtc 7500 aaaggcttct
atcccagcga catcgccgtg gagtgggaga gcaatgggca gccggagaac 7560
aactacaaga ccacgcctcc cgtgttggac tccgacggct ccttcttcct ctacagcaag
7620 ctcaccgtgg acaagagcag gtggcagcag gggaacgtct tctcatgctc
cgtgatgcat 7680 gaggctctgc acaaccacta cacgcagaag agcctctccc
tgtctccggg taaa 7734 <210> SEQ ID NO 10 <211> LENGTH:
2578 <212> TYPE: PRT <213> ORGANISM: Artificial
Sequence <220> FEATURE: <223> OTHER INFORMATION: Full
Length FVIIIFc <220> FEATURE: <221> NAME/KEY: SIGNAL
<222> LOCATION: (-19)..(-1) <220> FEATURE: <221>
NAME/KEY: mat_peptide <222> LOCATION: (1)..(2559) <400>
SEQUENCE: 10 Met Gln Ile Glu Leu Ser Thr Cys Phe Phe Leu Cys Leu
Leu Arg Phe -15 -10 -5 Cys Phe Ser Ala Thr Arg Arg Tyr Tyr Leu Gly
Ala Val Glu Leu Ser -1 1 5 10 Trp Asp Tyr Met Gln Ser Asp Leu Gly
Glu Leu Pro Val Asp Ala Arg 15 20 25 Phe Pro Pro Arg Val Pro Lys
Ser Phe Pro Phe Asn Thr Ser Val Val 30 35 40 45 Tyr Lys Lys Thr Leu
Phe Val Glu Phe Thr Asp His Leu Phe Asn Ile 50 55 60 Ala Lys Pro
Arg Pro Pro Trp Met Gly Leu Leu Gly Pro Thr Ile Gln 65 70 75 Ala
Glu Val Tyr Asp Thr Val Val Ile Thr Leu Lys Asn Met Ala Ser 80 85
90 His Pro Val Ser Leu His Ala Val Gly Val Ser Tyr Trp Lys Ala Ser
95 100 105 Glu Gly Ala Glu Tyr Asp Asp Gln Thr Ser Gln Arg Glu Lys
Glu Asp 110 115 120 125 Asp Lys Val Phe Pro Gly Gly Ser His Thr Tyr
Val Trp Gln Val Leu 130 135 140 Lys Glu Asn Gly Pro Met Ala Ser Asp
Pro Leu Cys Leu Thr Tyr Ser 145 150 155 Tyr Leu Ser His Val Asp Leu
Val Lys Asp Leu Asn Ser Gly Leu Ile 160 165 170 Gly Ala Leu Leu Val
Cys Arg Glu Gly Ser Leu Ala Lys Glu Lys Thr 175 180 185 Gln Thr Leu
His Lys Phe Ile Leu Leu Phe Ala Val Phe Asp Glu Gly 190 195 200 205
Lys Ser Trp His Ser Glu Thr Lys Asn Ser Leu Met Gln Asp Arg Asp 210
215 220 Ala Ala Ser Ala Arg Ala Trp Pro Lys Met His Thr Val Asn Gly
Tyr 225 230 235 Val Asn Arg Ser Leu Pro Gly Leu Ile Gly Cys His Arg
Lys Ser Val 240 245 250 Tyr Trp His Val Ile Gly Met Gly Thr Thr Pro
Glu Val His Ser Ile 255 260 265 Phe Leu Glu Gly His Thr Phe Leu Val
Arg Asn His Arg Gln Ala Ser 270 275 280 285 Leu Glu Ile Ser Pro Ile
Thr Phe Leu Thr Ala Gln Thr Leu Leu Met 290 295 300 Asp Leu Gly Gln
Phe Leu Leu Phe Cys His Ile Ser Ser His Gln His 305 310 315 Asp Gly
Met Glu Ala Tyr Val Lys Val Asp Ser Cys Pro Glu Glu Pro 320 325 330
Gln Leu Arg Met Lys Asn Asn Glu Glu Ala Glu Asp Tyr Asp Asp Asp 335
340 345 Leu Thr Asp Ser Glu Met Asp Val Val Arg Phe Asp Asp Asp Asn
Ser 350 355 360 365 Pro Ser Phe Ile Gln Ile Arg Ser Val Ala Lys Lys
His Pro Lys Thr 370 375 380 Trp Val His Tyr Ile Ala Ala Glu Glu Glu
Asp Trp Asp Tyr Ala Pro 385 390 395 Leu Val Leu Ala Pro Asp Asp Arg
Ser Tyr Lys Ser Gln Tyr Leu Asn 400 405 410 Asn Gly Pro Gln Arg Ile
Gly Arg Lys Tyr Lys Lys Val Arg Phe Met 415 420 425
Ala Tyr Thr Asp Glu Thr Phe Lys Thr Arg Glu Ala Ile Gln His Glu 430
435 440 445 Ser Gly Ile Leu Gly Pro Leu Leu Tyr Gly Glu Val Gly Asp
Thr Leu 450 455 460 Leu Ile Ile Phe Lys Asn Gln Ala Ser Arg Pro Tyr
Asn Ile Tyr Pro 465 470 475 His Gly Ile Thr Asp Val Arg Pro Leu Tyr
Ser Arg Arg Leu Pro Lys 480 485 490 Gly Val Lys His Leu Lys Asp Phe
Pro Ile Leu Pro Gly Glu Ile Phe 495 500 505 Lys Tyr Lys Trp Thr Val
Thr Val Glu Asp Gly Pro Thr Lys Ser Asp 510 515 520 525 Pro Arg Cys
Leu Thr Arg Tyr Tyr Ser Ser Phe Val Asn Met Glu Arg 530 535 540 Asp
Leu Ala Ser Gly Leu Ile Gly Pro Leu Leu Ile Cys Tyr Lys Glu 545 550
555 Ser Val Asp Gln Arg Gly Asn Gln Ile Met Ser Asp Lys Arg Asn Val
560 565 570 Ile Leu Phe Ser Val Phe Asp Glu Asn Arg Ser Trp Tyr Leu
Thr Glu 575 580 585 Asn Ile Gln Arg Phe Leu Pro Asn Pro Ala Gly Val
Gln Leu Glu Asp 590 595 600 605 Pro Glu Phe Gln Ala Ser Asn Ile Met
His Ser Ile Asn Gly Tyr Val 610 615 620 Phe Asp Ser Leu Gln Leu Ser
Val Cys Leu His Glu Val Ala Tyr Trp 625 630 635 Tyr Ile Leu Ser Ile
Gly Ala Gln Thr Asp Phe Leu Ser Val Phe Phe 640 645 650 Ser Gly Tyr
Thr Phe Lys His Lys Met Val Tyr Glu Asp Thr Leu Thr 655 660 665 Leu
Phe Pro Phe Ser Gly Glu Thr Val Phe Met Ser Met Glu Asn Pro 670 675
680 685 Gly Leu Trp Ile Leu Gly Cys His Asn Ser Asp Phe Arg Asn Arg
Gly 690 695 700 Met Thr Ala Leu Leu Lys Val Ser Ser Cys Asp Lys Asn
Thr Gly Asp 705 710 715 Tyr Tyr Glu Asp Ser Tyr Glu Asp Ile Ser Ala
Tyr Leu Leu Ser Lys 720 725 730 Asn Asn Ala Ile Glu Pro Arg Ser Phe
Ser Gln Asn Ser Arg His Pro 735 740 745 Ser Thr Arg Gln Lys Gln Phe
Asn Ala Thr Thr Ile Pro Glu Asn Asp 750 755 760 765 Ile Glu Lys Thr
Asp Pro Trp Phe Ala His Arg Thr Pro Met Pro Lys 770 775 780 Ile Gln
Asn Val Ser Ser Ser Asp Leu Leu Met Leu Leu Arg Gln Ser 785 790 795
Pro Thr Pro His Gly Leu Ser Leu Ser Asp Leu Gln Glu Ala Lys Tyr 800
805 810 Glu Thr Phe Ser Asp Asp Pro Ser Pro Gly Ala Ile Asp Ser Asn
Asn 815 820 825 Ser Leu Ser Glu Met Thr His Phe Arg Pro Gln Leu His
His Ser Gly 830 835 840 845 Asp Met Val Phe Thr Pro Glu Ser Gly Leu
Gln Leu Arg Leu Asn Glu 850 855 860 Lys Leu Gly Thr Thr Ala Ala Thr
Glu Leu Lys Lys Leu Asp Phe Lys 865 870 875 Val Ser Ser Thr Ser Asn
Asn Leu Ile Ser Thr Ile Pro Ser Asp Asn 880 885 890 Leu Ala Ala Gly
Thr Asp Asn Thr Ser Ser Leu Gly Pro Pro Ser Met 895 900 905 Pro Val
His Tyr Asp Ser Gln Leu Asp Thr Thr Leu Phe Gly Lys Lys 910 915 920
925 Ser Ser Pro Leu Thr Glu Ser Gly Gly Pro Leu Ser Leu Ser Glu Glu
930 935 940 Asn Asn Asp Ser Lys Leu Leu Glu Ser Gly Leu Met Asn Ser
Gln Glu 945 950 955 Ser Ser Trp Gly Lys Asn Val Ser Ser Thr Glu Ser
Gly Arg Leu Phe 960 965 970 Lys Gly Lys Arg Ala His Gly Pro Ala Leu
Leu Thr Lys Asp Asn Ala 975 980 985 Leu Phe Lys Val Ser Ile Ser Leu
Leu Lys Thr Asn Lys Thr Ser Asn 990 995 1000 1005 Asn Ser Ala Thr
Asn Arg Lys Thr His Ile Asp Gly Pro Ser Leu 1010 1015 1020 Leu Ile
Glu Asn Ser Pro Ser Val Trp Gln Asn Ile Leu Glu Ser 1025 1030 1035
Asp Thr Glu Phe Lys Lys Val Thr Pro Leu Ile His Asp Arg Met 1040
1045 1050 Leu Met Asp Lys Asn Ala Thr Ala Leu Arg Leu Asn His Met
Ser 1055 1060 1065 Asn Lys Thr Thr Ser Ser Lys Asn Met Glu Met Val
Gln Gln Lys 1070 1075 1080 Lys Glu Gly Pro Ile Pro Pro Asp Ala Gln
Asn Pro Asp Met Ser 1085 1090 1095 Phe Phe Lys Met Leu Phe Leu Pro
Glu Ser Ala Arg Trp Ile Gln 1100 1105 1110 Arg Thr His Gly Lys Asn
Ser Leu Asn Ser Gly Gln Gly Pro Ser 1115 1120 1125 Pro Lys Gln Leu
Val Ser Leu Gly Pro Glu Lys Ser Val Glu Gly 1130 1135 1140 Gln Asn
Phe Leu Ser Glu Lys Asn Lys Val Val Val Gly Lys Gly 1145 1150 1155
Glu Phe Thr Lys Asp Val Gly Leu Lys Glu Met Val Phe Pro Ser 1160
1165 1170 Ser Arg Asn Leu Phe Leu Thr Asn Leu Asp Asn Leu His Glu
Asn 1175 1180 1185 Asn Thr His Asn Gln Glu Lys Lys Ile Gln Glu Glu
Ile Glu Lys 1190 1195 1200 Lys Glu Thr Leu Ile Gln Glu Asn Val Val
Leu Pro Gln Ile His 1205 1210 1215 Thr Val Thr Gly Thr Lys Asn Phe
Met Lys Asn Leu Phe Leu Leu 1220 1225 1230 Ser Thr Arg Gln Asn Val
Glu Gly Ser Tyr Asp Gly Ala Tyr Ala 1235 1240 1245 Pro Val Leu Gln
Asp Phe Arg Ser Leu Asn Asp Ser Thr Asn Arg 1250 1255 1260 Thr Lys
Lys His Thr Ala His Phe Ser Lys Lys Gly Glu Glu Glu 1265 1270 1275
Asn Leu Glu Gly Leu Gly Asn Gln Thr Lys Gln Ile Val Glu Lys 1280
1285 1290 Tyr Ala Cys Thr Thr Arg Ile Ser Pro Asn Thr Ser Gln Gln
Asn 1295 1300 1305 Phe Val Thr Gln Arg Ser Lys Arg Ala Leu Lys Gln
Phe Arg Leu 1310 1315 1320 Pro Leu Glu Glu Thr Glu Leu Glu Lys Arg
Ile Ile Val Asp Asp 1325 1330 1335 Thr Ser Thr Gln Trp Ser Lys Asn
Met Lys His Leu Thr Pro Ser 1340 1345 1350 Thr Leu Thr Gln Ile Asp
Tyr Asn Glu Lys Glu Lys Gly Ala Ile 1355 1360 1365 Thr Gln Ser Pro
Leu Ser Asp Cys Leu Thr Arg Ser His Ser Ile 1370 1375 1380 Pro Gln
Ala Asn Arg Ser Pro Leu Pro Ile Ala Lys Val Ser Ser 1385 1390 1395
Phe Pro Ser Ile Arg Pro Ile Tyr Leu Thr Arg Val Leu Phe Gln 1400
1405 1410 Asp Asn Ser Ser His Leu Pro Ala Ala Ser Tyr Arg Lys Lys
Asp 1415 1420 1425 Ser Gly Val Gln Glu Ser Ser His Phe Leu Gln Gly
Ala Lys Lys 1430 1435 1440 Asn Asn Leu Ser Leu Ala Ile Leu Thr Leu
Glu Met Thr Gly Asp 1445 1450 1455 Gln Arg Glu Val Gly Ser Leu Gly
Thr Ser Ala Thr Asn Ser Val 1460 1465 1470 Thr Tyr Lys Lys Val Glu
Asn Thr Val Leu Pro Lys Pro Asp Leu 1475 1480 1485 Pro Lys Thr Ser
Gly Lys Val Glu Leu Leu Pro Lys Val His Ile 1490 1495 1500 Tyr Gln
Lys Asp Leu Phe Pro Thr Glu Thr Ser Asn Gly Ser Pro 1505 1510 1515
Gly His Leu Asp Leu Val Glu Gly Ser Leu Leu Gln Gly Thr Glu 1520
1525 1530 Gly Ala Ile Lys Trp Asn Glu Ala Asn Arg Pro Gly Lys Val
Pro 1535 1540 1545 Phe Leu Arg Val Ala Thr Glu Ser Ser Ala Lys Thr
Pro Ser Lys 1550 1555 1560 Leu Leu Asp Pro Leu Ala Trp Asp Asn His
Tyr Gly Thr Gln Ile 1565 1570 1575 Pro Lys Glu Glu Trp Lys Ser Gln
Glu Lys Ser Pro Glu Lys Thr 1580 1585 1590 Ala Phe Lys Lys Lys Asp
Thr Ile Leu Ser Leu Asn Ala Cys Glu 1595 1600 1605 Ser Asn His Ala
Ile Ala Ala Ile Asn Glu Gly Gln Asn Lys Pro 1610 1615 1620 Glu Ile
Glu Val Thr Trp Ala Lys Gln Gly Arg Thr Glu Arg Leu 1625 1630 1635
Cys Ser Gln Asn Pro Pro Val Leu Lys Arg His Gln Arg Glu Ile 1640
1645 1650 Thr Arg Thr Thr Leu Gln Ser Asp Gln Glu Glu Ile Asp Tyr
Asp 1655 1660 1665 Asp Thr Ile Ser Val Glu Met Lys Lys Glu Asp Phe
Asp Ile Tyr 1670 1675 1680 Asp Glu Asp Glu Asn Gln Ser Pro Arg Ser
Phe Gln Lys Lys Thr 1685 1690 1695 Arg His Tyr Phe Ile Ala Ala Val
Glu Arg Leu Trp Asp Tyr Gly 1700 1705 1710 Met Ser Ser Ser Pro His
Val Leu Arg Asn Arg Ala Gln Ser Gly 1715 1720 1725
Ser Val Pro Gln Phe Lys Lys Val Val Phe Gln Glu Phe Thr Asp 1730
1735 1740 Gly Ser Phe Thr Gln Pro Leu Tyr Arg Gly Glu Leu Asn Glu
His 1745 1750 1755 Leu Gly Leu Leu Gly Pro Tyr Ile Arg Ala Glu Val
Glu Asp Asn 1760 1765 1770 Ile Met Val Thr Phe Arg Asn Gln Ala Ser
Arg Pro Tyr Ser Phe 1775 1780 1785 Tyr Ser Ser Leu Ile Ser Tyr Glu
Glu Asp Gln Arg Gln Gly Ala 1790 1795 1800 Glu Pro Arg Lys Asn Phe
Val Lys Pro Asn Glu Thr Lys Thr Tyr 1805 1810 1815 Phe Trp Lys Val
Gln His His Met Ala Pro Thr Lys Asp Glu Phe 1820 1825 1830 Asp Cys
Lys Ala Trp Ala Tyr Phe Ser Asp Val Asp Leu Glu Lys 1835 1840 1845
Asp Val His Ser Gly Leu Ile Gly Pro Leu Leu Val Cys His Thr 1850
1855 1860 Asn Thr Leu Asn Pro Ala His Gly Arg Gln Val Thr Val Gln
Glu 1865 1870 1875 Phe Ala Leu Phe Phe Thr Ile Phe Asp Glu Thr Lys
Ser Trp Tyr 1880 1885 1890 Phe Thr Glu Asn Met Glu Arg Asn Cys Arg
Ala Pro Cys Asn Ile 1895 1900 1905 Gln Met Glu Asp Pro Thr Phe Lys
Glu Asn Tyr Arg Phe His Ala 1910 1915 1920 Ile Asn Gly Tyr Ile Met
Asp Thr Leu Pro Gly Leu Val Met Ala 1925 1930 1935 Gln Asp Gln Arg
Ile Arg Trp Tyr Leu Leu Ser Met Gly Ser Asn 1940 1945 1950 Glu Asn
Ile His Ser Ile His Phe Ser Gly His Val Phe Thr Val 1955 1960 1965
Arg Lys Lys Glu Glu Tyr Lys Met Ala Leu Tyr Asn Leu Tyr Pro 1970
1975 1980 Gly Val Phe Glu Thr Val Glu Met Leu Pro Ser Lys Ala Gly
Ile 1985 1990 1995 Trp Arg Val Glu Cys Leu Ile Gly Glu His Leu His
Ala Gly Met 2000 2005 2010 Ser Thr Leu Phe Leu Val Tyr Ser Asn Lys
Cys Gln Thr Pro Leu 2015 2020 2025 Gly Met Ala Ser Gly His Ile Arg
Asp Phe Gln Ile Thr Ala Ser 2030 2035 2040 Gly Gln Tyr Gly Gln Trp
Ala Pro Lys Leu Ala Arg Leu His Tyr 2045 2050 2055 Ser Gly Ser Ile
Asn Ala Trp Ser Thr Lys Glu Pro Phe Ser Trp 2060 2065 2070 Ile Lys
Val Asp Leu Leu Ala Pro Met Ile Ile His Gly Ile Lys 2075 2080 2085
Thr Gln Gly Ala Arg Gln Lys Phe Ser Ser Leu Tyr Ile Ser Gln 2090
2095 2100 Phe Ile Ile Met Tyr Ser Leu Asp Gly Lys Lys Trp Gln Thr
Tyr 2105 2110 2115 Arg Gly Asn Ser Thr Gly Thr Leu Met Val Phe Phe
Gly Asn Val 2120 2125 2130 Asp Ser Ser Gly Ile Lys His Asn Ile Phe
Asn Pro Pro Ile Ile 2135 2140 2145 Ala Arg Tyr Ile Arg Leu His Pro
Thr His Tyr Ser Ile Arg Ser 2150 2155 2160 Thr Leu Arg Met Glu Leu
Met Gly Cys Asp Leu Asn Ser Cys Ser 2165 2170 2175 Met Pro Leu Gly
Met Glu Ser Lys Ala Ile Ser Asp Ala Gln Ile 2180 2185 2190 Thr Ala
Ser Ser Tyr Phe Thr Asn Met Phe Ala Thr Trp Ser Pro 2195 2200 2205
Ser Lys Ala Arg Leu His Leu Gln Gly Arg Ser Asn Ala Trp Arg 2210
2215 2220 Pro Gln Val Asn Asn Pro Lys Glu Trp Leu Gln Val Asp Phe
Gln 2225 2230 2235 Lys Thr Met Lys Val Thr Gly Val Thr Thr Gln Gly
Val Lys Ser 2240 2245 2250 Leu Leu Thr Ser Met Tyr Val Lys Glu Phe
Leu Ile Ser Ser Ser 2255 2260 2265 Gln Asp Gly His Gln Trp Thr Leu
Phe Phe Gln Asn Gly Lys Val 2270 2275 2280 Lys Val Phe Gln Gly Asn
Gln Asp Ser Phe Thr Pro Val Val Asn 2285 2290 2295 Ser Leu Asp Pro
Pro Leu Leu Thr Arg Tyr Leu Arg Ile His Pro 2300 2305 2310 Gln Ser
Trp Val His Gln Ile Ala Leu Arg Met Glu Val Leu Gly 2315 2320 2325
Cys Glu Ala Gln Asp Leu Tyr Asp Lys Thr His Thr Cys Pro Pro 2330
2335 2340 Cys Pro Ala Pro Glu Leu Leu Gly Gly Pro Ser Val Phe Leu
Phe 2345 2350 2355 Pro Pro Lys Pro Lys Asp Thr Leu Met Ile Ser Arg
Thr Pro Glu 2360 2365 2370 Val Thr Cys Val Val Val Asp Val Ser His
Glu Asp Pro Glu Val 2375 2380 2385 Lys Phe Asn Trp Tyr Val Asp Gly
Val Glu Val His Asn Ala Lys 2390 2395 2400 Thr Lys Pro Arg Glu Glu
Gln Tyr Asn Ser Thr Tyr Arg Val Val 2405 2410 2415 Ser Val Leu Thr
Val Leu His Gln Asp Trp Leu Asn Gly Lys Glu 2420 2425 2430 Tyr Lys
Cys Lys Val Ser Asn Lys Ala Leu Pro Ala Pro Ile Glu 2435 2440 2445
Lys Thr Ile Ser Lys Ala Lys Gly Gln Pro Arg Glu Pro Gln Val 2450
2455 2460 Tyr Thr Leu Pro Pro Ser Arg Asp Glu Leu Thr Lys Asn Gln
Val 2465 2470 2475 Ser Leu Thr Cys Leu Val Lys Gly Phe Tyr Pro Ser
Asp Ile Ala 2480 2485 2490 Val Glu Trp Glu Ser Asn Gly Gln Pro Glu
Asn Asn Tyr Lys Thr 2495 2500 2505 Thr Pro Pro Val Leu Asp Ser Asp
Gly Ser Phe Phe Leu Tyr Ser 2510 2515 2520 Lys Leu Thr Val Asp Lys
Ser Arg Trp Gln Gln Gly Asn Val Phe 2525 2530 2535 Ser Cys Ser Val
Met His Glu Ala Leu His Asn His Tyr Thr Gln 2540 2545 2550 Lys Ser
Leu Ser Leu Ser Pro Gly Lys 2555 <210> SEQ ID NO 11
<211> LENGTH: 21 <212> TYPE: PRT <213> ORGANISM:
Artificial Sequence <220> FEATURE: <223> OTHER
INFORMATION: Partial B domain <400> SEQUENCE: 11 Ser Phe Ser
Gln Asn Ser Arg His Pro Ser Gln Asn Pro Pro Val Leu 1 5 10 15 Lys
Arg His Gln Arg 20 <210> SEQ ID NO 12 <211> LENGTH: 11
<212> TYPE: PRT <213> ORGANISM: Artificial Sequence
<220> FEATURE: <223> OTHER INFORMATION: albumin-binding
peptide <400> SEQUENCE: 12 Asp Ile Cys Leu Pro Arg Trp Gly
Cys Leu Trp 1 5 10 <210> SEQ ID NO 13 <211> LENGTH: 32
<212> TYPE: PRT <213> ORGANISM: Artificial Sequence
<220> FEATURE: <223> OTHER INFORMATION: CTP peptide
<400> SEQUENCE: 13 Asp Pro Arg Phe Gln Asp Ser Ser Ser Ser
Lys Ala Pro Pro Pro Ser 1 5 10 15 Leu Pro Ser Pro Ser Arg Leu Pro
Gly Pro Ser Asp Thr Pro Ile Leu 20 25 30 <210> SEQ ID NO 14
<211> LENGTH: 28 <212> TYPE: PRT <213> ORGANISM:
Artificial Sequence <220> FEATURE: <223> OTHER
INFORMATION: CTP peptide <400> SEQUENCE: 14 Ser Ser Ser Ser
Lys Ala Pro Pro Pro Ser Leu Pro Ser Pro Ser Arg 1 5 10 15 Leu Pro
Gly Pro Ser Asp Thr Pro Ile Leu Pro Gln 20 25 <210> SEQ ID NO
15 <211> LENGTH: 20 <212> TYPE: PRT <213>
ORGANISM: Artificial Sequence <220> FEATURE: <223>
OTHER INFORMATION: PAS peptide <400> SEQUENCE: 15 Ala Ser Pro
Ala Ala Pro Ala Pro Ala Ser Pro Ala Ala Pro Ala Pro 1 5 10 15 Ser
Ala Pro Ala 20 <210> SEQ ID NO 16 <211> LENGTH: 20
<212> TYPE: PRT <213> ORGANISM: Artificial Sequence
<220> FEATURE: <223> OTHER INFORMATION: PAS peptide
<400> SEQUENCE: 16 Ala Ala Pro Ala Ser Pro Ala Pro Ala Ala
Pro Ser Ala Pro Ala Pro 1 5 10 15 Ala Ala Pro Ser 20 <210>
SEQ ID NO 17 <211> LENGTH: 20 <212> TYPE: PRT
<213> ORGANISM: Artificial Sequence <220> FEATURE:
<223> OTHER INFORMATION: PAS peptide <400> SEQUENCE: 17
Ala Pro Ser Ser Pro Ser Pro Ser Ala Pro Ser Ser Pro Ser Pro Ala 1 5
10 15 Ser Pro Ser Ser 20 <210> SEQ ID NO 18 <211>
LENGTH: 19 <212> TYPE: PRT <213> ORGANISM: Artificial
Sequence <220> FEATURE: <223> OTHER INFORMATION: PAS
peptide <400> SEQUENCE: 18 Ala Pro Ser Ser Pro Ser Pro Ser
Ala Pro Ser Ser Pro Ser Pro Ala 1 5 10 15 Ser Pro Ser <210>
SEQ ID NO 19 <211> LENGTH: 20 <212> TYPE: PRT
<213> ORGANISM: Artificial Sequence <220> FEATURE:
<223> OTHER INFORMATION: PAS peptide <400> SEQUENCE: 19
Ser Ser Pro Ser Ala Pro Ser Pro Ser Ser Pro Ala Ser Pro Ser Pro 1 5
10 15 Ser Ser Pro Ala 20 <210> SEQ ID NO 20 <211>
LENGTH: 24 <212> TYPE: PRT <213> ORGANISM: Artificial
Sequence <220> FEATURE: <223> OTHER INFORMATION: PAS
peptide <400> SEQUENCE: 20 Ala Ala Ser Pro Ala Ala Pro Ser
Ala Pro Pro Ala Ala Ala Ser Pro 1 5 10 15 Ala Ala Pro Ser Ala Pro
Pro Ala 20 <210> SEQ ID NO 21 <211> LENGTH: 20
<212> TYPE: PRT <213> ORGANISM: Artificial Sequence
<220> FEATURE: <223> OTHER INFORMATION: PAS peptide
<400> SEQUENCE: 21 Ala Ser Ala Ala Ala Pro Ala Ala Ala Ser
Ala Ala Ala Ser Ala Pro 1 5 10 15 Ser Ala Ala Ala 20
D00000
D00001
D00002
D00003
D00004
D00005
D00006
D00007
D00008
D00009

D00010

D00011

D00012

D00013

D00014

D00015

D00016

D00017

D00018

D00019

D00020

D00021

D00022

D00023

D00024

D00025
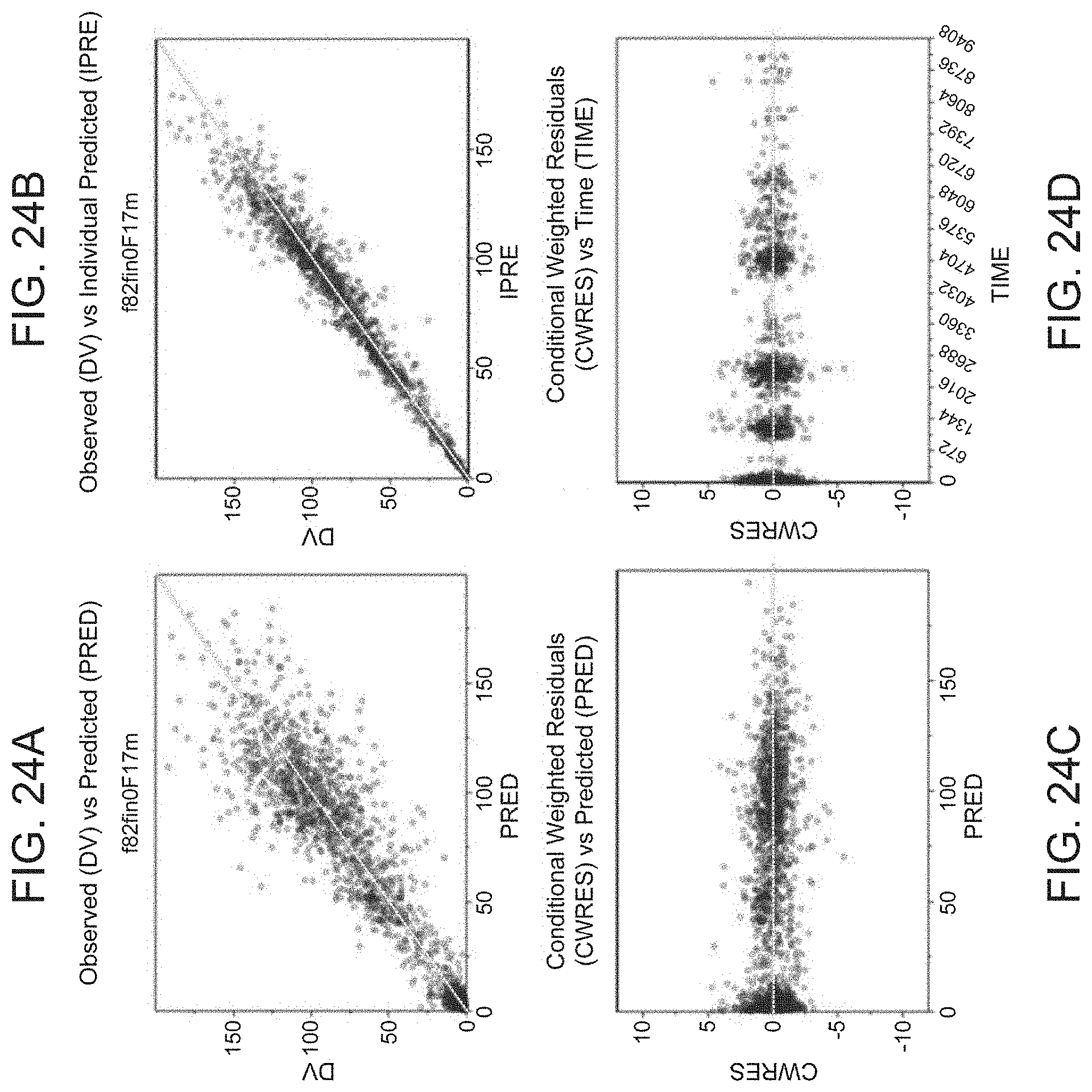
D00026

D00027

D00028

D00029
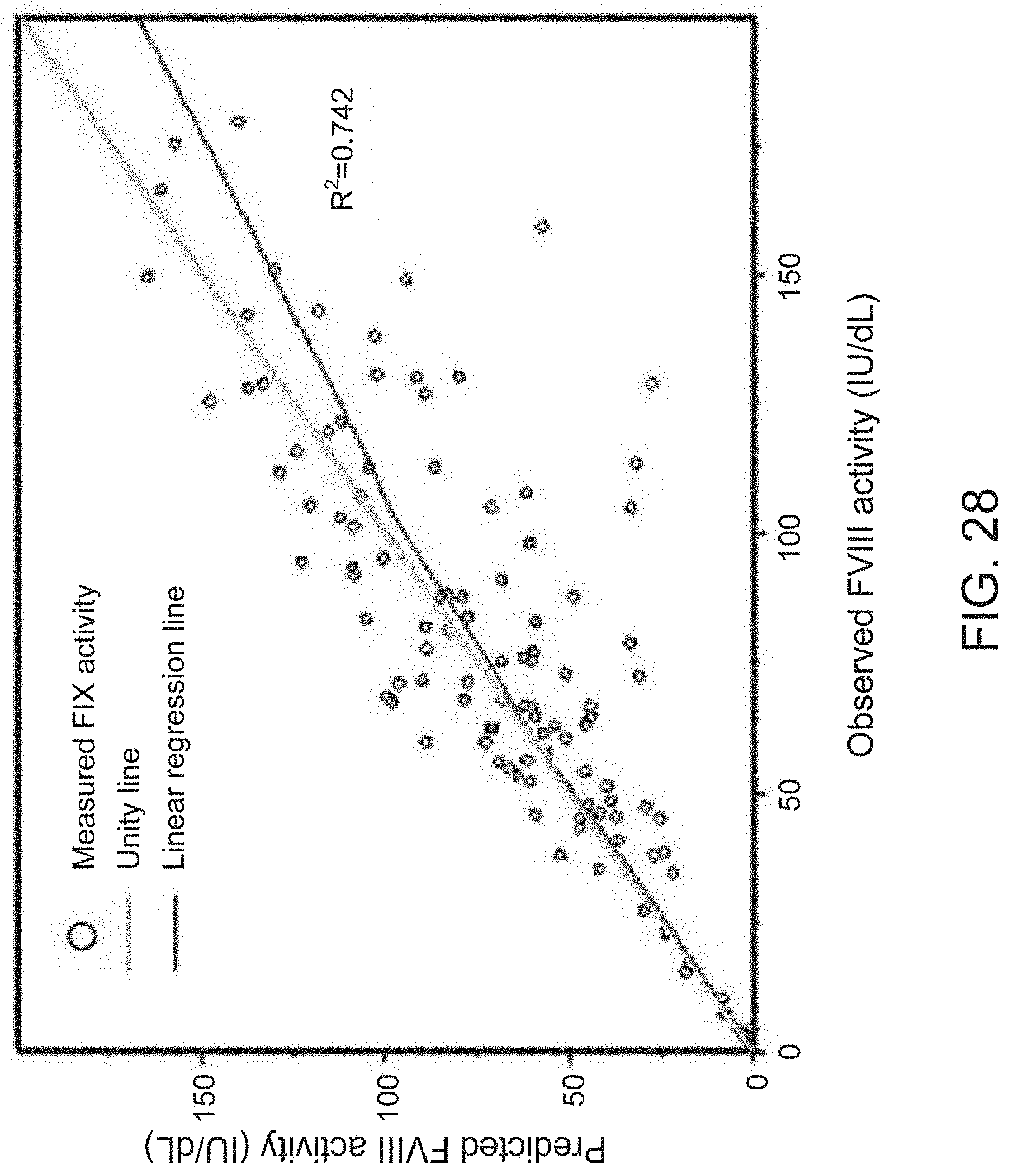
D00030

D00031

D00032

D00033
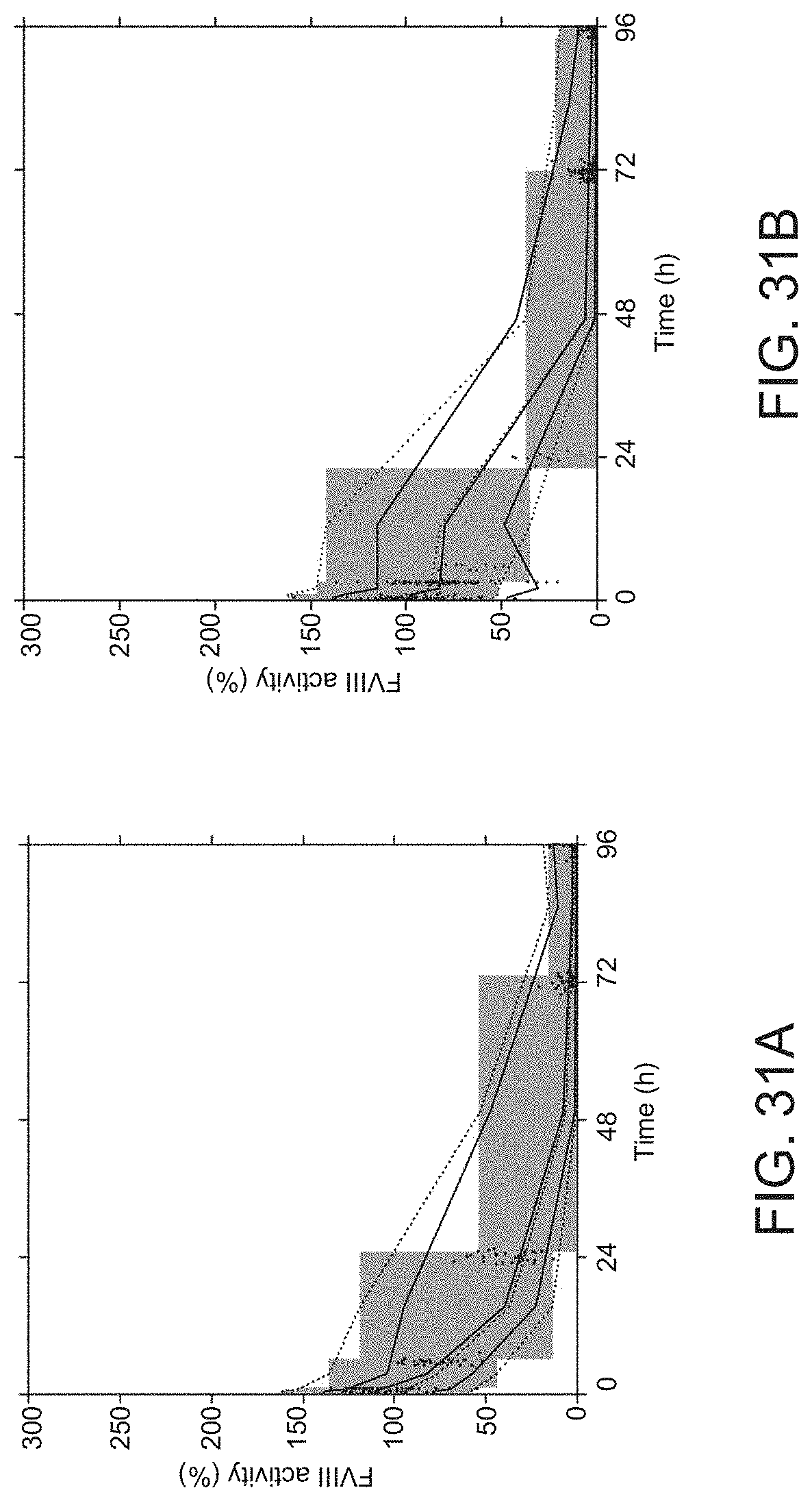
D00034

D00035

D00036

D00037

D00038

D00039

D00040

D00041

D00042

D00043

D00044

D00045

D00046

D00047

D00048

D00049

D00050

D00051

D00052

D00053

D00054

D00055

D00056

D00057

D00058

D00059

D00060

D00061

D00062

D00063

D00064

D00065

D00066












S00001
XML
uspto.report is an independent third-party trademark research tool that is not affiliated, endorsed, or sponsored by the United States Patent and Trademark Office (USPTO) or any other governmental organization. The information provided by uspto.report is based on publicly available data at the time of writing and is intended for informational purposes only.
While we strive to provide accurate and up-to-date information, we do not guarantee the accuracy, completeness, reliability, or suitability of the information displayed on this site. The use of this site is at your own risk. Any reliance you place on such information is therefore strictly at your own risk.
All official trademark data, including owner information, should be verified by visiting the official USPTO website at www.uspto.gov. This site is not intended to replace professional legal advice and should not be used as a substitute for consulting with a legal professional who is knowledgeable about trademark law.