Suturing Device with Split Arm and Method of Suturing Tissue
Stafford; Joshua
U.S. patent application number 16/533132 was filed with the patent office on 2019-11-28 for suturing device with split arm and method of suturing tissue. The applicant listed for this patent is Abbott Laboratories. Invention is credited to Joshua Stafford.
| Application Number | 20190357900 16/533132 |
| Document ID | / |
| Family ID | 34710673 |
| Filed Date | 2019-11-28 |






| United States Patent Application | 20190357900 |
| Kind Code | A1 |
| Stafford; Joshua | November 28, 2019 |
Suturing Device with Split Arm and Method of Suturing Tissue
Abstract
A device for suturing an opening in a tissue, having an elongated shaft, at least two arms are moveable to a deployed position in which the arms are non-perpendicular to the shaft. The arms have needle receiving portions. Needles are advanceable longitudinally along the shaft toward the needle receiving portions, the needles exiting through side walls of the shaft at a location proximal to the arms.
| Inventors: | Stafford; Joshua; (Menlo Park, CA) | ||||||||||
| Applicant: |
|
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Family ID: | 34710673 | ||||||||||
| Appl. No.: | 16/533132 | ||||||||||
| Filed: | August 6, 2019 |
Related U.S. Patent Documents
| Application Number | Filing Date | Patent Number | ||
|---|---|---|---|---|
| 15192481 | Jun 24, 2016 | 10413288 | ||
| 16533132 | ||||
| 14094352 | Dec 2, 2013 | 9375211 | ||
| 15192481 | ||||
| 13615530 | Sep 13, 2012 | 8597309 | ||
| 14094352 | ||||
| 12247012 | Oct 7, 2008 | 8419753 | ||
| 13615530 | ||||
| 10746210 | Dec 23, 2003 | 7449024 | ||
| 12247012 | ||||
| Current U.S. Class: | 1/1 |
| Current CPC Class: | A61B 2017/00672 20130101; A61B 2017/0477 20130101; A61B 2017/00663 20130101; A61B 17/0469 20130101; A61B 2017/00637 20130101; A61B 17/0057 20130101; A61B 2017/00641 20130101 |
| International Class: | A61B 17/04 20060101 A61B017/04; A61B 17/00 20060101 A61B017/00 |
Claims
1. An apparatus for suturing a puncture in a blood vessel, comprising: a body; a tissue locating assembly associated with the body and being movable between a pre-deployed position and a deployed position, the tissue locating assembly comprising: a first tissue locating member; and a second tissue locating member, wherein in the deployed position the first tissue locating member and the second tissue locating member orientate the body at a non-perpendicular angle with respect to an axis of the blood vessel into which the apparatus is deployed with the first tissue locating member being positioned longitudinally along an inside of a wall of the blood vessel; and a first needle configured to penetrate tissue, the first needle being configured to be withdrawn proximally from the tissue locating assembly and into the body following tissue penetration to draw a suture, disposed distal the puncture with the tissue locating assembly in the deployed position, proximally into the body.
2. The device of claim 1, wherein the first tissue locating member and the second tissue locating member are independently deployable.
3. The device of claim 1, wherein the second tissue locating member is positioned longitudinally along the inside of the wall of the blood vessel.
4. The device of claim 1, wherein the first tissue locating member is inclined less than 90 degrees to the longitudinal axis of the body in the deployed position.
5. The device of claim 4, wherein second tissue locating member is inclined more than 90 degrees to the longitudinal axis of the body in the deployed position.
6. The device of claim 1, further comprising a second needle.
7. An apparatus for suturing a puncture in a blood vessel, comprising: an elongate body; a tissue locating assembly having a pre-deployed position and a deployed position, the tissue locating assembly comprising: a first tissue locating member extending radially outwardly in a first direction transverse to a longitudinal axis of the elongate body; and a second tissue locating member extending radially outwardly in a second direction transverse to the longitudinal axis of the elongate body, the second tissue locating member being on an opposite side of the longitudinal axis from the first tissue locating member, wherein in the deployed position the first tissue locating member and the second tissue locating member orientate the body at a non-perpendicular angle with respect to an axis of the blood vessel into which the tissue locating assembly is deployed; a first needle configured to be moved proximally through tissue and proximally away from the tissue locating assembly and into the body to draw a suture, disposed distal the puncture with the tissue locating assembly in the deployed position, proximally into the body; and an actuation assembly slidable with respect to the elongate body and configured to move the first tissue locating member to transition between the pre-deployed position and the deployed position.
8. The device of claim 7, wherein the first tissue locating member and the second tissue locating member are independently deployable.
9. The device of claim 7, wherein the second tissue locating member is positioned longitudinally along the inside of the wall of the blood vessel.
10. The device of claim 7, wherein the first tissue locating member is inclined less than 90 degrees to the longitudinal axis of the body in the deployed position.
11. The device of claim 10, wherein second tissue locating member is inclined more than 90 degrees to the longitudinal axis of the body in the deployed position.
12. The apparatus of claim 7, wherein the first direction of the first tissue locating member positions the first tissue locating member at a first angle with respect to the longitudinal axis and the second direction of the second tissue locating member positions the second tissue locating member at a second angle with respect to the longitudinal axis, the second angle being shallower than the first angle.
13. The apparatus of claim 7, wherein the first direction of the first tissue locating member positions the first tissue locating member at an acute angle with respect to the longitudinal axis.
14. The apparatus of claim 7, wherein the second direction of the second tissue locating member positions the second tissue locating member at an obtuse angle with respect to the longitudinal axis.
15. The apparatus of claim 7, wherein the first tissue locating member pivots with respect to the second tissue locating member when transitioning between the pre-deployed position and the deployed position.
16. The apparatus of claim 7, wherein the first tissue locating member and the second tissue locating member are asymmetrical.
17. An apparatus for suturing a puncture in a blood vessel, comprising: an elongate body; a first needle and a second needle; a tissue locating assembly having a pre-deployed position and a deployed position, the tissue locating assembly orientating the body at a non-perpendicular angle with respect to an axis of the blood vessel into which the tissue locating assembly is deployed, the tissue locating assembly accommodating for movement of the first needle and the second needle and withdrawal of a suture, disposed distal the puncture with the tissue locating assembly in the deployed position, proximally into the body, the tissue locating assembly comprising: a first tissue locating member extending radially outwardly at an acute angle with respect to a longitudinal axis of the elongate body in the deployed position; and a second tissue locating member extending radially outwardly at an obtuse angle with respect to the longitudinal axis of the elongate body in the deployed position, the second tissue locating member being on an opposite side of the longitudinal axis from the first tissue locating member, each of the first tissue locating member and the second locating member rotating about different rotational centers to transition between the pre-deployed position and the deployed position; and an actuation assembly slidable with respect to the elongate body and configured to move the first tissue locating member to transition between the pre-deployed position and the deployed position.
18. The apparatus of claim 17, wherein in the deployed position the first tissue locating member is positioned longitudinally along an inside of a wall of the blood vessel.
19. The apparatus of claim 17, wherein the first tissue locating member and the second tissue locating member are asymmetrical.
20. The apparatus of claim 17, wherein the first tissue locating member transitions between the pre-deployed position the deployed position differently from the second tissue locating member.
Description
CROSS-REFERENCE TO RELATED APPLICATIONS
[0001] This application is a continuation of U.S. patent application Ser. No. 15/192,481, filed Jun. 24, 2016, now U.S. Patent No. ______, which is a continuation of U.S. patent application Ser. No. 14/094,352, filed Dec. 2, 2013, now U.S. Pat. No. 9,375,211, which is a continuation of U.S. patent application Ser. No. 13/615,530, filed Sep. 13, 2012, now U.S. Pat. No. 8,597,309, which is a continuation of U.S. patent application Ser. No. 12/247,012, filed Oct. 7, 2008, now U.S. Pat. No. 8,419,753, which is a Divisional Application of U.S. patent application Ser. No. 10/746,210, filed Dec. 23, 2003, now U.S. Pat. No. 7,449,024, the disclosures of which are each incorporated herein by this reference.
BACKGROUND
1. Background and Relevant Art
[0002] The present invention relates generally to apparatus and methods for the suturing of body lumens. More particularly, the present invention relates to techniques for percutaneous closure of arterial and venous puncture sites, which are usually accessed through a tissue tract.
[0003] A number of diagnostic and interventional vascular procedures are now performed translumenally. A catheter is introduced to the vascular system at a convenient access location and guided through the vascular system to a target location using established techniques. Such procedures require vascular access, which is usually established during the well-known Seldinger technique, as described, for example, in William Grossman's "Cardiac Catheterization and Angioplasty," 3.sup.rd Ed., Lea and Febiger, Philadelphia, 1986, incorporated herein by reference. Vascular access is generally provided through an introducer sheath, which is positioned to extend from outside the patient body into the vascular lumen.
[0004] When vascular access is no longer required, the introducer sheath is removed and bleeding at the puncture site stopped. One common approach for providing hemostasis (the cessation of bleeding) is to apply external force near and upstream from the puncture site, typically by manual or "digital" compression. This approach suffers from a number of disadvantages. It is time consuming, frequently requiring one-half hour or more of compression before hemostasis is assured. Additionally, such compression techniques rely on clot formation, which can be delayed until anticoagulants used in vascular therapy procedures (such as for heart attacks, stent deployment, non-optical PTCA results, and the like) wear off. This can take two to four hours, thereby increasing the time required before completion of the compression technique. The compression procedure is further uncomfortable for the patient and frequently requires analgesics to be tolerable. Moreover, the application excessive pressure can at times totally occlude the underlying blood vessel, resulting in ischemia and/or thrombosis. Following manual compression, the patient typically remains recumbent from four to as much as twelve hours or more under close observation so as to assure continued hemostasis. During this time renewed bleeding may occur, resulting in blood loss through the tract, hematoma and/or pseudoaneurysm formation, as well as arteriovenous fistula formation. These complications may require blood transfusion and/or surgical intervention.
[0005] The incidence of complications from compression-induced hemostasis increases when the size of the introducer sheath grows larger, and/or when the patient is anticoagulated. It is clear that the compression technique for arterial closure can be risky, and is expensive and onerous to the patient. Although the risk of complications can be reduced by using highly trained individuals, dedicating such personnel to this task is both expensive and inefficient. Nonetheless, as the number and efficacy of translumenally performed diagnostic and interventional vascular procedures increases, the number of patients requiring effective hemostasis for a vascular puncture continues to increase.
[0006] To overcome the problems associated with manual compression, the use of bioabsorbable fasteners or sealing bodies to stop bleeding has previously been proposed. Generally, these approaches rely on the placement of a thrombogenic and bioabsorbable material, such as collagen, at the superficial arterial wall over the puncture site. While potentially effective, this approach suffers from a number of problems. It can be difficult to properly locate the interface of the overlying tissue and the adventitial surface of the blood vessel. Locating the fastener too far from that interface can result in failure to provide hemostasis, and subsequent hematoma and/or pseudo-aneurysm formation. Conversely, if the sealing body intrudes into the arterial lumen, intravascular clots and/or collagen pieces with thrombus attached can form and embolize downstream, causing vascular occlusion. Also, thrombus formation on the surface of a sealing body protruding into the lumen can cause a stenosis, which can obstruct normal blood flow. Other possible complications include infection, as well as adverse reaction to the collagen or other implant.
[0007] A more effective approach for vascular closure has been proposed in U.S. Pat. Nos. 5,417,699, 5,613,974; and PCT published Patent Application No. PCT/US96/10271 filed on Jun. 12, 1996, the full disclosures of which are incorporated herein by reference. A suture-applying device is introduced through the tissue tract with a distal end of the device extending through the vascular puncture. One or more needles in the device are then used to draw suture through the blood vessel wall on opposite sides of the puncture, and the suture is secured directly over the adventitial surface of the blood vessel wall to provide highly reliable closure.
[0008] While a significant improvement over the use of manual pressure, clamps, and collagen plugs, certain design criteria have been found to be important to successful suturing to achieve vascular closure. For example, it is highly beneficial to properly direct the needles through the blood vessel wall at a significant distance from the puncture so that the suture is well anchored in the tissue and can provide tight closure. It is also highly beneficial to ensure that the needle deployment takes place when the device is properly positioned relative to the vessel wall. The ease of deployment and efficacy of the procedure can further be enhanced by reducing the cross-section of that portion of the device, which is inserted into the tissue tract and/or the vessel itself, which may also allow closure of the vessel in a relatively short amount of time without imposing excessive injury to the tissue tract or vessel.
[0009] For the above reasons, it would be desirable to provide improved devices, systems, and methods for suturing vascular punctures. The new device should have the capability of delivering a pre-tied knot to an incision site. It would be particularly beneficial if these improved devices provided some or all of the benefits while overcoming one or more of the disadvantages discussed above.
2. Description of the Background Art
[0010] U.S. Pat. Nos. 5,700,273, 5,836,956, and 5,846,253 describe a wound closure apparatus and method in which needles are threaded with suture inside a blood vessel. U.S. Pat. No. 5,496,332 describes a wound closure apparatus and method for its use, while U.S. Pat. No. 5,364,408 describes an endoscopic suture system.
[0011] U.S. Pat. No. 5,374,275 describes a surgical suturing device and method of use, while U.S. Pat. No. 5,417,699 describes a device and method for the percutaneous suturing of a vascular puncture site. An instrument for closing trocar puncture wounds is described in U.S. Pat. No. 5,470,338, and a related device is described in U.S. Pat. No. 5,527,321. U.S. Pat. No. 5,507,757 also describes a method of closing puncture wounds.
[0012] U.S. Patent 6,245,079, describes another suturing system, the complete disclosure of which is incorporated herein by reference in its entirety for all purposes.
BRIEF SUMMARY
[0013] The present invention provides a device for suturing an opening in a tissue. In various embodiments, the device includes an elongated shaft with a pair of deployable arms. When deployed, these arms are non-perpendicular to the longitudinal axis of the shaft. In one embodiment, the arms are independently deployable. In one embodiment, a first arm is an anterior arm which is deployed by being rotated less than 90 degrees to the longitudinal axis of the shaft, and the second arm is a posterior arm which is deployed by being rotated more than 90 degrees to the longitudinal axis of the shaft. A pivot stop may be provided on the elongated shaft to limit rotation of the arms when they reach their fully deployed position. Each of the first and second arms may include a needle receiving portion thereon. Needles may be advanced longitudinally along the shaft toward the needle receiving portions on the arms. The needles may exit through a side wall of the shaft at a location proximal to the arms
BRIEF DESCRIPTION OF THE DRAWINGS
[0014] FIG. 1 is a cross-sectional view of a suturing system with its distal end inserted through an arterial wall. (FIG. 1 corresponds to FIG. 41 of U.S. Pat. No. 6,245,079).
[0015] FIG. 2 is a cross-sectional view of the device of FIG. 41 in a partially deployed state. (FIG. 2 corresponds to FIG. 42 of U.S. Pat. No. 6,245,079).
[0016] FIG. 3 is cross-sectional view of the device of FIG. 1 with the suture clasp member fully deployed. (FIG. 3 corresponds to FIG. 47 of U.S. Pat. No. 6,245,079).
[0017] FIG. 4A is a front plan view of the present invention in its compact position (i.e. prior to deployment).
[0018] FIG. 4B is a left side elevation view of the present invention prior to deployment.
[0019] FIG. 5A is a front plan view of the present invention after deployment.
[0020] FIG. 5B is a right side elevation view of the present invention after deployment.
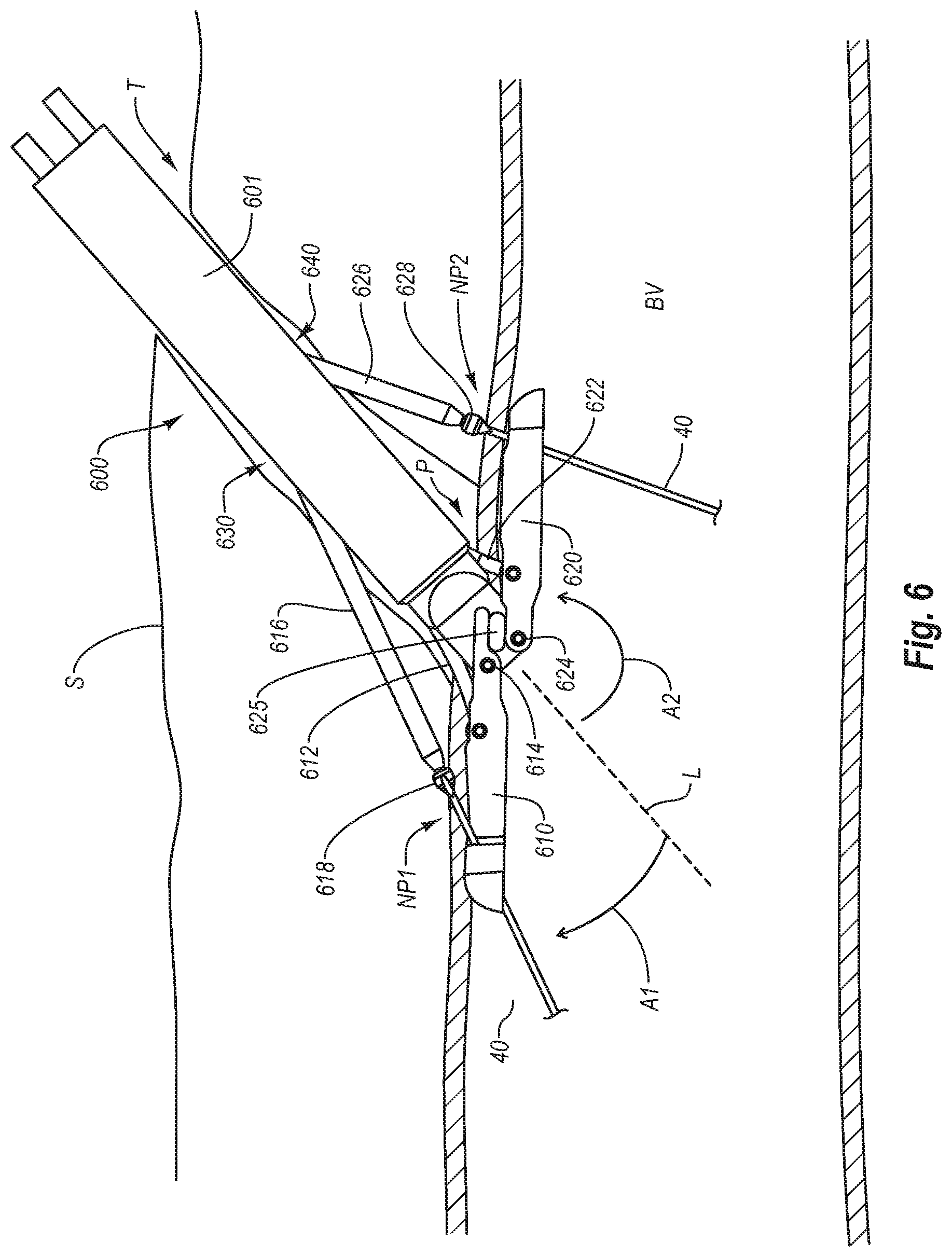
[0021] FIG. 6 is an illustration of the system of FIG. 5B deployed at a non-perpendicular angle relative to the axis of a blood vessel while the first and second arms 610 and 620 are positioned longitudinally along the inside of the wall of blood vessel.
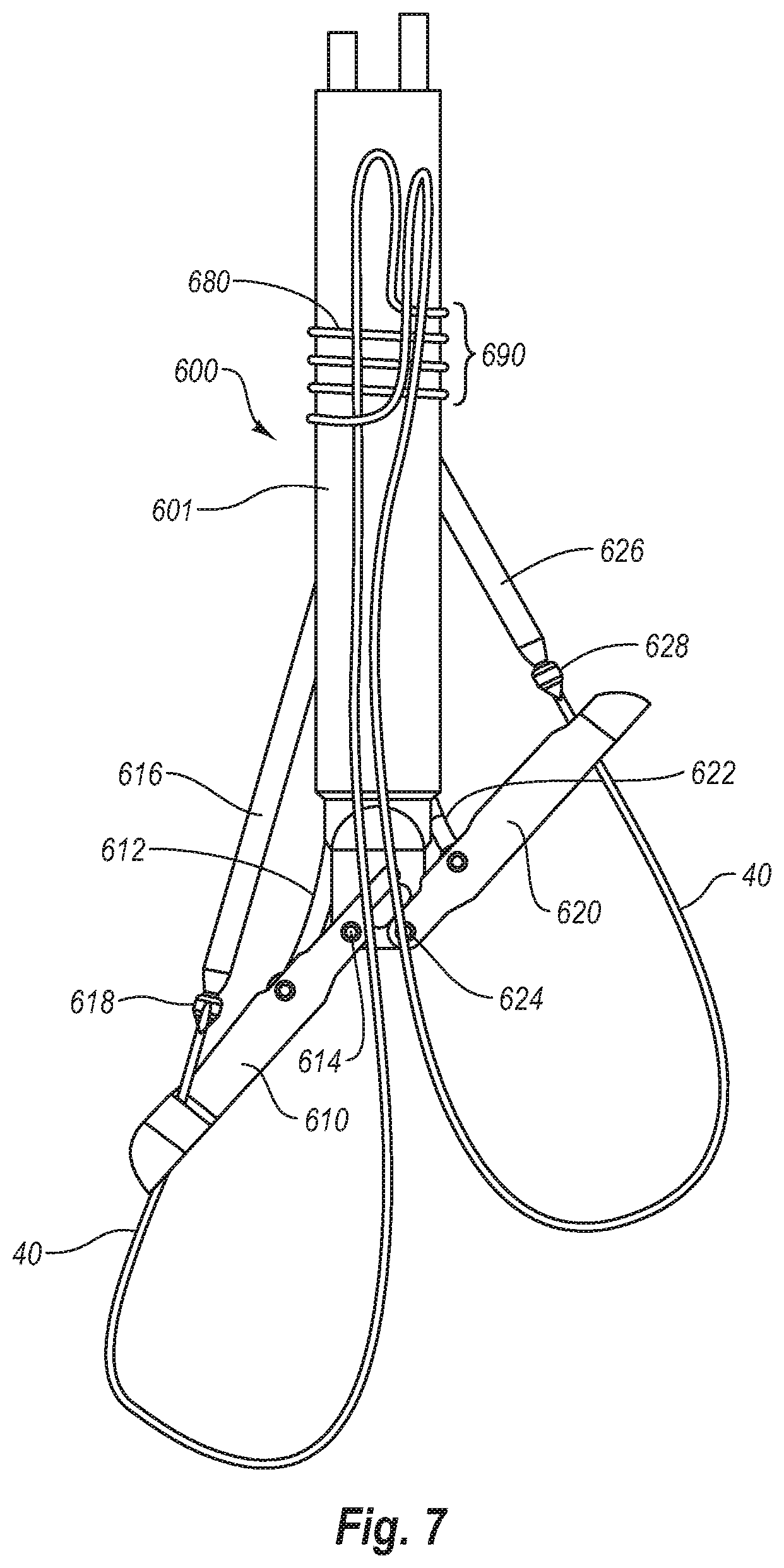
[0022] FIG. 7 is an embodiment of the present split arm invention, incorporating a pre-tied knot.
DETAILED DESCRIPTION
[0023] FIGS. 1, 2 and 3 show a suturing device corresponding to the suturing device described in U.S. Pat. No. 6,245,079, the complete disclosure of which is incorporated herein by reference in its entirety for all purposes. Specifically, FIGS. 1, 2, and 3 correspond to FIGS. 41, 42 and 47 of U.S. Pat. No. 6,245,079.
[0024] Referring to FIG. 1, distal portion of the suturing device 520 is positioned in femoral artery 16. Suturing device 520 comprises a suture introducer head 522 attached to the distal end of a hollow elongated body 514. Suture clasp member 500 and the needles 546 reside in the same longitudinal space. In other words, the needles 546 share the same housing as the suture clasp member 500 (while they are all in their retracted state), but are higher up (proximally) in the suturing device 520 than the suture clasp member 500. Flexible needles 546 bend outward, away from the axis of the device 520, when in the extended position (as shown in FIG. 3).
[0025] As shown in FIGS. 2 and 3, the suture introducer head 522 has two needle ports or apertures 510 formed therein (one per needle 546) proximal to the suture clasp arms 524. Each needle port includes a needle guiding portion 512 ("needle guide"), in the form of an outwardly curved groove or channel, which guides the corresponding needle 546 along a particular path. The needle guides 512 may be formed within the suture introducer head 522 (as shown in FIG. 1) as part of a mold, or may be separate pieces (not shown) that are inserted into the suture introducer head 522 during manufacture.
[0026] Bleed back is accomplished by the hole 540 at the distal end 504 of the suture introducer head 522, the suture clasp arm apertures 508 and any other openings in the suture introducer head 522. The direction of blood flow for bleed back is shown by the dashed arrows in FIG. 1.
[0027] Suture 40 closes the artery vessel opening 26 transverse to the flow of blood. Proper insertion of the needles 546 reduces the risk of damage to the vessel walls 22, 506.
[0028] Suturing device 520 includes a single, resilient suture clasp member 500 attached to the actuating rod 50. The suture clasp member 500 comprises a center or hinge portion 542 and two suture clasp arms 524 (one for each needle 546). Each suture clasp arm 524 has a suture clasp 544 at the end thereof.
[0029] The hinge portion 542 of the suture clasp member 500 acts as a "living hinge" because it has a memory which causes the member 500 to return to a partially open, unretracted position (FIG. 2) when a force (applied via rod 50) is released. This can be seen in FIGS. 1 and 2. In FIG. 2, the suture clasp member 500 is deployed in the artery 16 in its predisposed (relaxed or natural) position. In FIG. 1, the suture clasp member 500 is retracted into the suture introducer head 522 in its compressed (stressed or tensed) position. The arms 524 are moved to the retracted position by applying a distal force to the actuator rod 50, which causes the arms to contact deflection surfaces 518 (FIG. 2).
[0030] This suture clasp member 500 is preferably composed of a resilient shape memory material such as NITINOL, but may alternatively be composed of another material with spring-like characteristics, such as plastic, spring steel, stainless steel or any variations thereof. Further, the suture clasp member 500 could be composed of two arms that are hingedly connected to the actuating rod 50 without the use of a resilient hinge.
[0031] Needles 546 are flexible and preferably made from a material with shape memory, such as SUPERFLEX NITINOL. Alternatively, the needles 546 may be composed of spring steel, surgical stainless steel or any variation thereof.
[0032] When the needles 546 are advanced distally and come in contact with the needle insertion guides 512, the needle insertion guides cause the needles 546 to bend radially outward. The needles 546 also preferably further bend slightly (radially outward) when they come in contact with the angled surfaces 545 of the suture clasp arms 524, as shown in FIG. 3. When the needles 546 are retracted into the needle lumens 516, they resume a straight configuration as a result of their resiliency.
[0033] The proximal portion of the suturing device 520 preferably includes a handle which allows the physician to externally operate the suture clasp arms 524 and the needles 546 inside the blood vessel 16. This handle preferably has three actions: a first action in which the actuating rod 50 applies a proximal force to the hinge portion 542 to deploy and maintain arms 524 in a fully outward position (FIG. 3); a second action to advance the needles 546 distally (FIG. 3) and pull the needles 546 back proximally using one or more springs; and a third action in which the actuating rod 50 applies a distal force to the hinge portion 542 to retract the arms 524 (FIG. 1).
[0034] The locked position of the suture clasp arms 524 provides a stable base or foundation for holding the looped ends of the suture 40 while the needles 546 come in contact with the suture clasp arms 524 and capture the suture 40. The suture clasp arms 524 are locked in the locked position by the proximal force of the actuating rod 50, the stationary inside edges 536 of the apertures 508 and the protrusions 528 at the `elbow` end of each arm 524 (FIG. 3). Specifically, when the suture clasp arms 524 become substantially parallel with each other (i.e., each arm 524 is at an angle of approximately 90 degrees from the actuating rod 50), the protrusions 528 at the `elbow` end of each arm 524 come into contact with each other and prevent the arms 524 from bending any further than the configuration shown in FIG. 3. The suture clasp member 500 cannot open any farther, even when the needles 546 are inserted distally and come in contact with the suture clasp arms 524. The protrusions 528 prevent the suture clasp member 500 from moving unintentionally (opening any farther) when the needles 546 come in contact with the suture clasp arms 524. This reduces the risk of the looped ends of the suture 40 being accidentally displaced from the suture clasps 544 when the needles 546 engage the suture clasps 544. Thus, the combination of forces asserted by the actuating rod 50, the proximal inside edges 536 of the aperture 508 and the two protrusions 528 sustain the suture clasp arms 524 in a rigid, locked position to facilitate the proper removal of the suture looped ends from the suture clasps 544.
[0035] The slits of the suture clasps 544 are angled in a proximal, radially inward direction. Thus, the face of the looped ends of the suture 40 face in a proximal, radially inward direction. In this configuration, there is less chance of the looped ends of the suture 40 falling off the suture clasps 544 improperly or prematurely. When the needles 546 engage the suture clasp arms 524, the only direction the looped ends may move is in a proximal, radially inward direction, which is in the opposite direction of the inserted needles 546. When the needles 546 retract proximally (as shown in FIG. 3), the looped ends reliably fall into the suture catches 38 of the needles 546. It is the proximal movement of the needles 546 which causes the suture catches 38 on the needles 546 to catch the looped ends of the suture 40. This configuration does not rely on a radially outward tension in the looped ends to fasten the looped ends onto the suture catches 38 when the needles 546 are inserted distally.
[0036] The description of each of introducer sheath 6, suture catches 38, needle incisions 248, pivot pin 502 and lumen 530 is provided by reference to identically numbered elements in U.S. Pat. No. 6,245,079.
[0037] A first important disadvantage of the suturing system illustrated in FIGS. 1, 2 and 3 is that both of the arms 524 deploy to a position that is exactly 90 degrees from the axis of suturing device. This is because protrusions 528 abut one another when suture clasp 500 is fully opened (as shown in FIG. 3). As described above, and in U.S. Pat. No. 6,245,079, it is an advantage of the system of FIGS. 1 to 3 that arms 542 of suture clasp 500 do not open more than 90 degrees to reduce the risk of the looped ends of the suture 40 being accidentally displaced from the suture clasps 544 when the needles 546 engage the suture clasps 544.
[0038] Unfortunately, this is particularly problematic when suturing inside a blood vessel, since it may be preferred to enter the blood vessel at a non-perpendicular (e.g.: oblique) angle. In the system of FIGS. 1 to 3, the distal end of the suturing device must therefore be extended to some distance into the blood vessel during operation.
[0039] A first feature of the embodiments of the present split arm suturing device is that each of its arms may be extended to different angles from the body of the device. In various embodiments, such angles are non-perpendicular to the longitudinal axis of the suturing device. More particularly, one arm may be extended to a position less than 90 degrees to the body of the device, whereas the other arm may be extended to a position more than 90 degrees to the body of the device.
[0040] A second feature of various embodiments of the present split arm suturing device is that each of its arms may be extended one at a time.
[0041] Separately, or taken together, these two features of the present invention provide a system which may be conveniently positioned to enter the blood vessel at a non-perpendicular angle, thus minimizing the potential for damage to the blood vessel, while ensuring proper placement of the suture. Thus, an operator can gain better access to smaller arteries and maintain a smaller elbow height, as compared to the suturing device of FIGS. 1 to 3. Thus, the present independently operable split arm suturing device offers significantly increased flexibility to the operator, as compared to the suturing device of FIGS. 1 to 3.
[0042] Referring first to FIG. 4A and 4B, split arm suturing device 600 is shown prior to deployment (i.e. in its compact position). Suturing device 600 has moveable arms 610 and 620 which can be pivoted relative to the longitudinal axis L of suturing device 600. Arms 610 and 620 may be independently moveable. As will be shown herein, when deployed, arm 610 will preferably be deployed in an anterior direction, and arm 620 will preferably be deployed in a posterior direction.
[0043] Anterior arm 610 and posterior arm 620 may be made independently moveably by any of a variety of mechanisms, all keeping within the scope of the present invention. In the illustrated embodiments, arms 610 and 620 are independently actionable (i.e. moveable between compact and deployed positions) by flexible linkages in tension or compression. It is to be understood, however, that any push pull wire, gear or cam system, or any other suitable actuation system may be used, all keeping within the scope of the present invention. As illustrated in FIG. 5B, arm 610 may be deployed by moving linkage 612, and arm 620 may be deployed by moving linkage 622. Specifically, by pulling linkage 612 proximally, anterior arm 610 rotates around pivot 614 until finger 611 contacts pivot stop 625. Similarly, by pulling linkage 622 proximally, posterior arm 620 rotates (in an opposite direction) around pivot 624 until stop surface 621 contacts pivot stop 625. Specifically, anterior arm 610 moves through angle Al when moved from its compact position to its deployed position. Referring to FIG. 6, posterior arm 620 moves through angle A2 when moved from its compact position to its deployed position. As can be appreciated, by instead distally pushing linkages 612 and 622, arms 610 and 620 can be moved back to their compact (i.e.: non-deployed) position.
[0044] After deploying arms 610 and 620 (by retracting linkages 612 and 622) a first needle 616, and a second needle 626 can then be advanced toward the distal ends of arms 610 and 620, respectively to retrieve opposite ends of a suture 40. In various embodiments, needles 616 and 626 are longitudinally advanceable along the shaft 601 of suturing device 600, and exit through side wall openings 630 and 640 at locations proximal to the arms 610 and 620, respectively.
[0045] FIG. 6 shows an embodiment of the present invention deployed at a non-perpendicular angle relative to the axis of a blood vessel BV while the anterior arm 610 and posterior arm 620 are positioned longitudinally along the inside of the wall of blood vessel BV. Specifically, the distal end of suturing device 600 is positioned though a puncture P in blood vessel BV.
[0046] Needles 616 and 626 are advanced longitudinally along through shaft, and exit through side wall openings 630 and 640, and then puncture through respective needle punctures NP1 and NP2 in the wall of blood vessel BV. Thereafter, needles 616 and 626 can be retracted pulling the opposite ends of suture 40 upwardly through punctures NP1 and NP2 in the wall of blood vessel BV.
[0047] In various embodiments, cuffs 618 and 628 can be provided at opposite ends of suture 40 to ensure that the distal ends of needles 616 and 626 connect securely onto the opposite ends of suture 40. Various embodiments of cuffs, links, barbs, fasteners, or combinations thereof are also contemplated to ensure that the distal ends of needles 616 and 626 connect securely onto the opposite ends of suture 40. Thus, cuffs 618 and 628 may be any of a variety of different designs.
[0048] Referring again to FIGS. 5A and 5B, by moving linkages 612 and 622 independently, and to different distances, arms 610 and 620 may be independently deployed to different angles relative to the longitudinal axis L of the body of suturing device 600. For example, as shown in FIGS. 5A and 5B, arm 610 may be rotated less than 90 degrees from the axis of the elongated body of suturing device 600, whereas 620 may be rotated more than 90 degrees from the axis of the elongated body of suturing device 600.
[0049] As shown in FIG. 6, this advantageously allows the elongated body of suturing device 600 to be positioned through tissue Tract T (entering through skin S) at a non-perpendicular angle relative to the axis of a blood vessel BV while the first and second arms 610 and 620 are positioned longitudinally along the inside of the wall of blood vessel BV for placement of the suture axially along the blood vessel and across the puncture. Specifically, suturing device 600 can be used to position the ends of suture 40 at locations such that they can be retrieved by needles 616 and 626, and pulled upwardly through needle punctures NP1 and NP2, respectively.
[0050] In various embodiments, the elongated body of suturing device 600 is sufficiently rigid to maintain alignment of needles 616 and 626 with arms 610 and 620, respectively. As can be seen, in various embodiments, needles 616 and 626 may be of different lengths.
[0051] As shown in FIG. 7, a pre-tied knot feature may also be incorporated into suturing device 600. The pre-tied knot may initially be positioned wrapped around an exterior surface of the suturing device. Specifically, a length of suture 40 having opposite ends and a bight 680 of suture therebetween may be provided with bight 680 being disposed around an exterior surface of device 600. Bight 680 may alternately be pre-arranged around one of the needles and within the elongated body.
[0052] Bight 680 includes one or more loops of suture that form a pre-tied knot 690 when one or more ends of suture 40 are advanced through bight 680. Bight 680 of suture may be prearranged in any of several configurations on the device. For example, bight 680 may be pre-arranged so as to define a square knot, a clinch knot or a variety of known or new surgical knots.
[0053] In various embodiments, suture 40 is arranged to provide the pre-tied knot 680 that automatically travels down from the shaft of the device 600 where it is stored prior to delivery to the tissue wall. In various embodiments, to distinguish the ends of suture 40, during deployment, the ends of the suture may be distinguished from each other by changing the color of one end (e.g. with dye), providing an attachment on one end (e.g. shrink wrap tubing, a bead, etc.) or with the suture itself (e.g. tying a knot in one end).
[0054] In accordance with the present invention, suture bight 680 is disposed on the outside surface of device 600, as shown. In this embodiment, suture 40 does not pass through the interior of the device. It should be understood, however, that other embodiments of the invention may include suture 40 and bight 680 stored inside the shaft or housing of the device rather than on the outside. Yet other configurations may include detachable tips and connecting filaments to enable a pre-tied knot.
[0055] After needles 616 and 626 retrieve opposite ends of suture 40, and pull these ends of the suture back up through the center of bight 680 to define the pre-tied knot 690, and arms 610 and 620 are rotated back to a non-deployed position, device 600 may be removed from the patient. Pre-tied knot 690 will slide down the shaft, resulting in a suture pattern in which the opposite ends of suture 40 pass upwardly through the center of bight 680.
[0056] While embodiments and applications of this invention have been shown and described, it will be apparent to those skilled in the art that various modifications are possible without departing from the scope of the invention. It is, therefore, to be understood that within the scope of the appended claims, this invention may be practiced otherwise than as specifically described.
* * * * *
D00000
D00001
D00002
D00003
D00004
D00005
D00006
D00007
XML
uspto.report is an independent third-party trademark research tool that is not affiliated, endorsed, or sponsored by the United States Patent and Trademark Office (USPTO) or any other governmental organization. The information provided by uspto.report is based on publicly available data at the time of writing and is intended for informational purposes only.
While we strive to provide accurate and up-to-date information, we do not guarantee the accuracy, completeness, reliability, or suitability of the information displayed on this site. The use of this site is at your own risk. Any reliance you place on such information is therefore strictly at your own risk.
All official trademark data, including owner information, should be verified by visiting the official USPTO website at www.uspto.gov. This site is not intended to replace professional legal advice and should not be used as a substitute for consulting with a legal professional who is knowledgeable about trademark law.